Effect of long-term proton pump inhibitor therapy on complete blood count parameters and selected trace elements: a pilot study
Key words: complete blood count, copper, proton pump inhibitors, selenium, zinc



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Effect of long-term proton pump inhibitor therapy on complete blood count parameters and selected trace elements: a pilot study
Introduction: Proton pump inhibitors (PPIs) are widely prescribed for several gastrointestinal conditions, often as long‑term therapy. The effects of long‑term PPI use have not been fully elucidated.
Objectives: We aimed to determine the association between long‑term PPI use and complete blood count parameters, particularly red blood cell (RBC) count, white blood cell (WBC) count, and hemoglobin concentrations, as well as serum levels of selected micronutrients such as selenium (Se), iron (Fe), copper (Cu), and zinc (Zn).
Patients and methods: We enrolled 37 patients on long‑term PPI therapy (mean [SD] age, 57.1 [15.4] years) and 30 healthy controls (mean [SD] age, 39.3 [11.8] years). In each group, complete blood count, and serum Fe levels were performed, and serum Cu, Zn, and Se levels were measured using atomic absorption spectrometry.
Results: Red blood cell and WBC counts were lower in the PPI group compared with controls (mean [SD], 4.24 [0.55] × 106/μl vs 4.7 [0.4] × 106/μl; P <0.001 and 6.13 [1.44] × 103/μl vs 7.3 [1.28] × 103/μl; P <0.001, respectively). Hemoglobin and serum Fe concentrations were also lower in the PPI group (mean [SD], 12.5 [1.8] g/dl vs 14.3 [0.8] g/dl; P <0.001 and 16.3 [5.4] μmol/l vs 23.4 [2.7] μmol/l; P <0.001, respectively). Serum Zn and Cu concentrations were higher in PPI users than in controls.
Conclusions: Long‑term PPI therapy may reduce RBC and WBC counts as well as hemoglobin levels, leading to iron deficiency. It may also affect concentrations of some micronutrients, although the underlying mechanism of this association is not fully clear.
What's new?
The study demonstrated that long‑term proton pump inhibitor (PPI) therapy may reduce red blood cell count, white blood cell count, and hemoglobin levels, leading to iron deficiency. It may also affect the concentrations of some micronutrients such as copper and zinc, although the underlying mechanism of this association is not clear. We indicated that a change in gastric pH may not be the only factor affecting the intestinal absorption of trace elements in patients taking PPIs. Other such factor might be oxidative stress. On the other hand, gastroprotective effects of PPIs can not only be explained by their antisecretory function. Our findings showed that PPIs should be prescribed with awareness. Monitoring of prolonged therapy should be introduced, particularly in the population of elderly or malnourished patients. This is especially important as PPIs are extensively prescribed both in primary care and hospital settings.
Introduction
Proton pump inhibitors (PPIs) are widely prescribed for treatment of acid‑related gastrointestinal disorders such as peptic ulcer disease, gastroesophageal reflux disease, or dyspepsia. They also play a role in prevention of gastric ulcers in some clinical situations.1
The efficacy and perceived safety of PPIs have led to their widespread prescription and over‑the‑counter availability. In the United States, they are the most overprescribed medications in adults.2 Proton‑pump inhibitors should only be used when appropriate, in accordance with label instructions, and for the shortest duration to achieve symptom response, but several reports have described inappropriate prescription of PPIs both in primary care and hospital settings.1,3 Prolonged PPI therapy is associated with adverse events and pharmacologic interactions.3-5 Undesirable effects include small intestinal bacterial overgrowth, hypomagnesemia, decreased cyanocobalamin absorption, acute interstitial nephritis, bone fractures, and diarrhea associated with Clostridioides difficile (formerly Clostridium difficile).6 The use of PPI increases mortality and hepatic decompensation in patients with liver cirrhosis.5 A correlation between PPI use and cognitive function has been postulated, but the exact effect seems to be unclear.7 A number of studies, discussed below, indicated a possible effect of changes in gastric acidity on the level of micronutrients, such as selenium (Se), zinc (Zn), and copper (Cu).
Selenium is an essential micronutrient that is incorporated in a variety of selenoproteins to render their beneficial physiologic functions. It also plays an important role as an antioxidant and is considered an anticancer nutrient.8 Steevens et al9 reported a negative correlation between the Se status and gastric and esophageal cancers.
Zinc is another micronutrient with a pivotal role in homeostasis, immune function, oxidative reactions, apoptosis, and aging. It is a structural element of Cu/Zn superoxide dismutase, which is intracellularly distributed in red blood cells (RBCs); therefore, it is involved in oxidative reactions. Zinc deficiency is related to several conditions such as malignancies, neuropsychiatric disorders, autoimmune diseases, or aging processes with apoptosis.10
Copper is an essential trace element in human physiology and a major constituent of numerous enzymes. It is a potent antioxidant that plays an important role in the oxidant defense system.11 Its deficiency results in microcytic anemia, leukopenia, and reduced bone density.12
The aim of this study was to determine the effect of PPIs on complete blood count parameters, particularly RBCs, white blood cells (WBCs), and hemoglobin concentrations.
Moreover, we measured serum levels of Se, iron (Fe), Cu, and Zn in PPI users and compared with nonusers (controls).
Patients and methods
Study population
A total of 67 participants were enrolled to the study, including 37 PPI users (55%) and 30 healthy controls (45%) who did not use PPIs. The mean (SD) age of PPI users was 57.1 (15.4) years, and of controls, 39.3 (11.8) years. In the PPI group, 18 patients used pantoprazole; 7, omeprazole; 1, lansoprazole; 9, esomeprazole; and 2, dexlansoprazole. Enrolled patients used the PPI due to gastroesophageal reflux disease and functional dyspepsia. The PPI‑therapy duration varied between 3 and 10 years at referral to Outpatient Gastroenterology and Hepatology Clinic at Jagiellonian University Medical College in Kraków, Poland. Periods without drug use did not exceed 3 months.
The exclusion criteria were as follows: pregnancy, any malignancies, diabetes mellitus, obesity (body mass index ≥30 kg/m2), cardiovascular diseases (hypertension, coronary artery disease, valvular heart disease, cardiac arrhythmias), tobacco smoking, intake of medications that may affect serum Se, Zn, or Cu concentrations, as well as malabsorption syndromes (eg, celiac disease, short bowel syndrome). Patients included in the study did not present overt or occult bleeding symptoms. They did not take medications such as nonsteroidal anti‑inflammatory drugs, steroids, anticoagulant therapy, immunosuppressive, antiviral drugs, selective serotonin reuptake inhibitor treatment and chemotherapy.
Biochemical analysis
The biochemical analyses including complete blood count and the measurement of serum Fe concentrations were conducted at the Biochemical and Molecular Diagnostics Unit of the Department of Clinical Biochemistry at Jagiellonian University Medical College, Kraków, Poland. Complete blood count included the measurement of hemoglobin concentrations, mean corpuscular volume (MCV), WBC, RBC, platelet count, and RBC distribution width (RDW).
The serum levels of Cu and Zn were measured with the Perkin‑Elmer 5100ZL atomic absorption spectrometer using flame technique (PerkinElmer Inc., Norwalk, Connecticut, United States). The calibration curves for Cu and Zn were performed using 0, 0.25, 0.5, 1, 2, and 3 mg/l standards. These solutions were prepared by dilution of standard solutions, 1000 mg/l (Merck, Darmstadt, Germany): Cu (1.19786.0500) and Zn (1.19806.0500). Thawed serum (0.5 ml) was mixed with 2 ml of demineralized water (Milli‑RQ10, Millipore, Vienna, Austria) and analyzed as described above. Each sample was measured 3 times. If the relative standard deviation of the 3 measurements exceeded 5%, then the sample was remeasured. The correctness of the obtained results was checked with Seronorm (200805) and Pathonorm (100705) control serum (Sero, Billingstad, Norway). The parameters for Cu were: wavelength, 324.8 nm; lamp current, 15 mA; slit width, 0.7 nm; air flow, 9.0 l/min; and acetylene, 2 l/min. The parameters for Zn were: wavelength, 213.9 nm; lamp current, 18 mA; slit width, 0.7 nm; air flow, 10.8 l/min; and acetylene 2 l/min.
The Se level was determined using the atomic absorption spectrometer Agilent Technologies 240Z AA (Agilent Technologies, Santa Clara, California, United States) with graphite furnace atomization and Zeeman background correction. The calibration curve was prepared using 3 serum Se standards, namely, 0.35, 0.61, and 1.77 µmol/l. The accuracy of the results was confirmed with Seronorm reference material (Trace Elements Serum L‑1, Sero). A hollow‑cathode lamp with enhanced light intensity (“ultra‑lamp”) (Agilent Technologies, Santa Clara, Califormia, United States) was used as the light source, and high‑purity argon (99.998%) (Linde Gaz Polska Sp. z o.o., Kraków, Poland) was used as inert gas.
Serum samples were mixed with 0.1% Triton solution (150 µl + 100 µl) to improve homogeneity. Owing to the presence of complex organic matrix in the samples, a chemical modifier was used and air‑assisted ashing was included in the temperature program of the graphite furnace. The samples were measured in duplicates unless the obtained precision was not satisfactory (in such case samples were remeasured). The parameters of the analysis were as follows: wavelength, 196.0 nm; lamp current, 12 mA; slit, 1 nm; chemical modifier, 5% HNO3 containing 1500 mg/l Pd and 6000 mg/l Mg(NO3)2; air‑assisted ashing temperature, 400 °C; inert‑gas ashing temperature, 1150 °C; and atomization temperature, 2600 °C.
Ethical approval
The study protocol was approved by the local bioethical committee at Jagiellonian University (no. KBET 122.6120.86.2015, as of May 28, 2015). All participants gave their written informed consent to be included in the study.
Statistical analysis
Data were expressed as mean (SD). The differences between groups were tested using the t test or the Welch test, as appropriate. The Levene test was used to assess the equality of variances in the study groups. A P value of less than 0.05 was considered significant. Pearson correlation coefficients were calculated for pairs of parameters. A partial least square (PLS) model was applied to describe the correlation structure between parameters in a mixed group of controls and patients treated with PPIs (using the analysis of component weights) and to reveal possible differences between controls and patients (using the analysis of PLS score plot). The PLS model showed the correlations between predictive parameters such as age of patients, blood parameters, and concentrations of trace elements, with response parameters including Fe and hemoglobin concentrations (parameters characterizing oxygen binding and transport). Parameters with large weights (>0.3) in the PLS model were assumed to be correlated with one another. To express the strength of bivariate associations, for the pairs of correlated parameters, the algebraic products of their corresponding weights and cosine of the corresponding angle were calculated (these coefficients are called the correlation weights). The corresponding angle was defined as the angle determined by 2 lines connecting the origin with coordinates of both parameters on the PLS weights plot. The PLS approach was also applied with the aim to identify any possible clusters of patients and healthy controls in the PLS score plot. Statistical analyses were carried out using the STATISTICA, version 12 package (Statsoft, Tulsa, Oklahoma, United States) and SIMCA‑P, version 9 (Umetrics, Umeå, Sweden). The software delivered by MP System Sp. z o.o. (Chrzanów, Poland) was used to calculate correlation weights for the pairs of parameters in the PLS model and to detect outliers.
Results
The comparison of analyzed parameters between the PPI and control groups is shown in Table 1. Patients treated with PPIs had lower RBC and WBC counts as well as serum Fe levels than controls. The hemoglobin level was also lower in patients treated with PPIs. There was no difference in platelet counts between groups. Serum Zn and Cu levels were lower in controls than in the PPI group, but no differences were observed for Se levels. The Pearson correlation analysis showed positive correlations between RBC and hemoglobin levels, as well as RBC and serum Fe levels (Table 2). An increase in the RBC count was correlated with higher hemoglobin concentrations and MCV. There was also a positive correlation between serum Se levels and MCV. No correlations between RBC and Cu or Se levels were observed (Table 2).
Parameter | PPI (n = 37) | Controls (n = 30) | P value |
Data are presented as mean (SD).
SI conversion factors: to convert WBC to × 109/l, multiply by 0.001; hemoglobin to g/dl, by 10; Zn to μmol/l, by 15.3; Cu to μmol/l, by 15.7.
Abbreviations: Cu, copper; Fe, iron; MCV, mean corpuscular volume; PPI, proton pump inhibitor; RBC, red blood cells; RDW‑CV, red blood cell distribution width, coefficient of variation; RDW‑SD, red blood cell distribution width, standard deviation; Se, selenium; WBC, white blood cells; Zn, zinc | |||
Age, y | 57.1 (15.4) | 39.1 (11.8) | <0.001 |
RBC, × 1012/μl | 4.24 (0.55) | 4.7 (0.4) | <0.001 |
WBC, × 103/μl | 6.13 (1.44) | 7.3 (1.2) | <0.001 |
Platelets, × 109/μl | 259.1 (58.5) | 263.3 (56) | 0.77 |
Hemoglobin, g/dl | 12.5 (1.8) | 14.3 (0.8) | <0.001 |
Fe, μmol/l | 16.3 (5.4) | 23.4 (2.7) | <0.001 |
RDW‑CV, % | 13.1 (1.4) | 13.6 (3.4) | 0.45 |
RDW‑SD, fl | 41.0 (3) | 40.8 (2.1) | 0.08 |
MCV, fl | 88.1 (5.6) | 84.8 (3.3) | <0.001 |
Zn, mg/l | 0.95 (0.22) | 0.83 (0.13) | 0.01 |
Cu, mg/l | 1.14 (0.25) | 0.97 (0.22) | <0.001 |
Se, μmol/l | 0.98 (0.2) | 0.93 (0.19) | 0.33 |
Pairs of correlated parameters | Correlation weights | Pearson correlation coefficients | P value |
Abbreviations: see Table 1 | |||
RBC with hemoglobin | 0.396 | 0.712 | 0.001 |
RBC with MCV | 0.279 | –0.331 | 0.01 |
RBC with Cu | 0.254 | 0.001 | 0.99 |
RBC with Se | 0.242 | 0.081 | 0.51 |
RBC with Fe | 0.203 | 0.295 | 0.01 |
Se with MCV | 0.156 | 0.325 | 0.01 |
Age with hemoglobin | –0.201 | 0.220 | 0.07 |
Age with RBC | –0.319 | –0.210 | 0.08 |
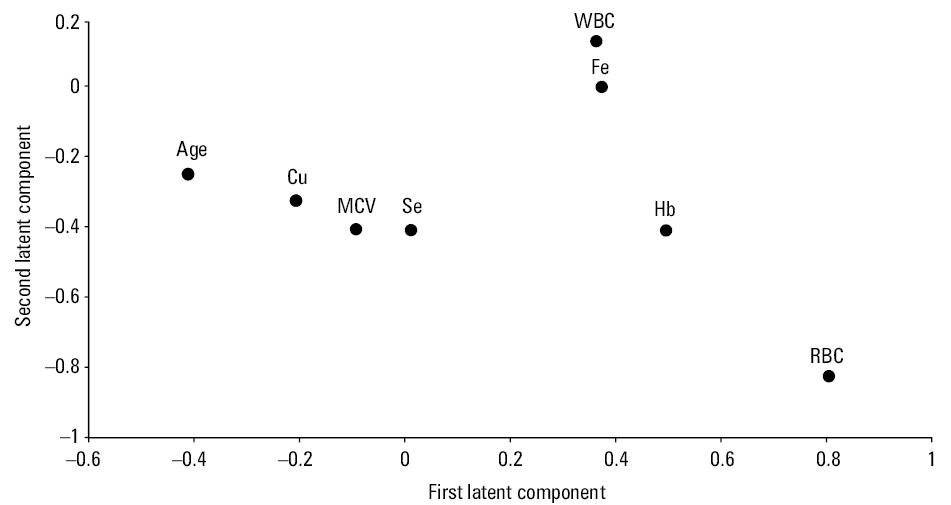
Correlation weights obtained from the PLS model are presented in Table 2. The final PLS model with 2 significant components, according to cross‑validation, explained 50.6% of variance in the predictive parameters, and 38.6% of variance in the response parameters, with eigenvalues of 1.79 and 1.24 for the first and second components, respectively. Five predictive parameters (age, Cu, Se, MCV, and WBC) and 2 response parameters (Fe, hemoglobin) were included in the PLS model, while others were excluded as they were considered noninformative (Figure 1). The first latent component in this model had positive weights predominantly for the RBC count, as well as for hemoglobin and Fe levels, while it had high negative weight for age. The highest positive correlation weights based on this latent component were revealed between RBC count and both hemoglobin and Fe levels. The second latent component was loaded again mainly by RBC count, and 4 other parameters with similar weights: hemoglobin, Se, MCV, and Cu. Therefore, RBC count had high correlation weights with all these parameters. The PLS model revealed correlation structure between the above parameters: RBC and hemoglobin, RBC and Fe, Se, and MCV, and also between RBC and Se, RBC and Cu, age and hemoglobin, as well as age and RBC. For the correlation between RBC count and MCV, we obtained discrepant results using the PLS model and Pearson correlation analysis.
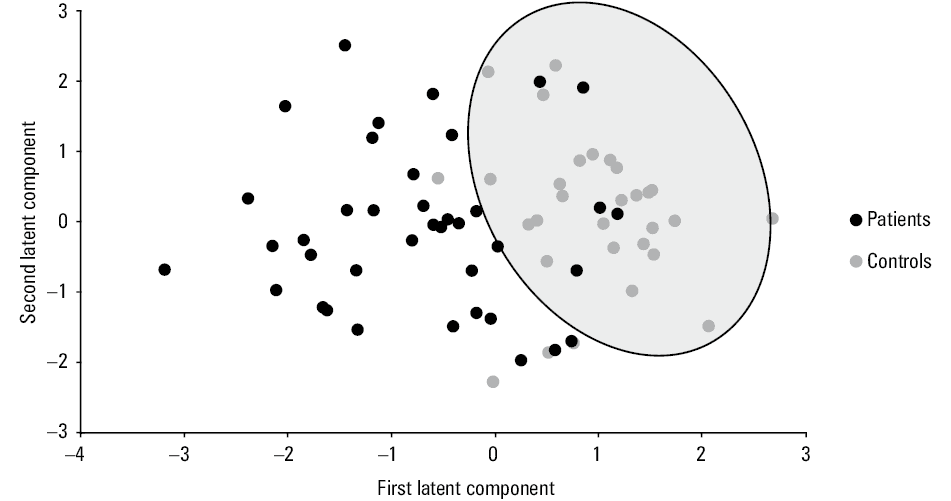
The results of patients determined by the first 2 latent components are shown in Figure 2. A relatively tight cluster of squares representing controls can be distinguished among the cloud of dots representing patients. True positive and negative rates for this cluster were 86.7% and 87.8%, respectively. The separation between this cluster and patients was evident in the direction determined only by the first latent component of the PLS model. Considering this result, controls within this cluster were characterized by apparently higher RBC, WBC, hemoglobin, and Fe levels, as well as lower Cu levels and age compared with patients. This is in line with the results obtained by the t test or the Welch test (Table 1).
Discussion
The effect of prolonged PPI use on complete blood count has not been fully elucidated so far. Our results revealed a relationship between prolonged PPI use and reduced RBC and WBC counts as well as hemoglobin levels. One of the reasons for this finding may be reduced Fe levels demonstrated in patients treated with PPIs in comparison with controls, as reduced Fe levels may lead to subsequent changes in other parameters. In addition, we showed an effect of PPIs on serum concentrations of Cu and Zn.
Data on suppression of gastric acid during long‑term PPI therapy leading to iron‑deficiency anemia are sparse. Patients with Zollinger‑Ellison syndrome during such therapy were shown to have reduced Fe levels.13 On the other hand, Hutchson et al14 showed reduced frequency of phlebotomy and absorption of nondietary Fe in patients with hereditary hemochromatosis on prolonged PPI therapy. In a retrospective cohort study, Sarzynski et al15 reported a decrease in hemoglobin, Ht, and MCV levels among patients on PPI therapy. Moreover, in a case‑control study, Lam et al16 reported that a PPI use longer than 2 years was associated with iron‑deficiency anemia. In an open‑labelled study, Qorray‑Bytygi et al17 assessed ferritin levels at the beginning and after 12 months of PPI therapy. They reported lower ferritin levels at 1 year in comparison with controls.
The presence of gastric acid facilitates dietary Fe absorption by dissociating Fe salts, increasing solubility, and transforming them to the ferrous form.18 The above observations are consistent with the results of our studies indicating decreased RBC count as well as hemoglobin and Fe levels in PPI users.
The PLS model revealed correlation structure between the majority of analyzed parameters. The RBC count was strongly correlated with all parameters except the WBC count. The biochemical basis for the observed correlations between RBC and hemoglobin, Fe, and Cu can be easily explained, because Fe and Cu play a fundamental role in erythropoiesis, and hemoglobin is an essential constituent of RBCs. The negative correlation of age with RBC and hemoglobin may be explained by the fact that lower RBC count and hemoglobin levels were observed in patients who were, at the same time, older than controls. The question of whether this was an accidental finding or whether it occurred in the course of the disease or due to the disease itself needs to be addressed in future studies.
The distinct cluster of squares representing controls (containing only a few patients) on the plane defined by the first 2 latent components of the PLS model reflects a notable difference in biochemical characteristics between patients and controls, which means that the PLS model is effective enough to differentiate between these 2 groups. Our analysis indicated that RBC, hemoglobin, and age were the parameters that differed the most between patients and controls. To the best of our knowledge, no clinical trials on patients taking PPIs have used the PLS approach to interpret the results.
A drawback of this study is a relatively small number of the patients studied and quite a large difference in mean age between the control and treatment groups. To exclude additional effects on blood test and Fe values, included patients did not present overt or occult bleeding symptoms. The study group, despite being older than the control group, did not have more serious, chronic diseases that could affect the parameters tested, did not take medications such as nonsteroidal anti‑inflammatory drugs, steroids, clopidogrel. We tried to eliminate the influence of the age difference of the studied groups on the results of measured parameters by using the PLS model.
In contrast to the RBC count, platelet counts did not differ between groups. Literature data concerning platelet count are conflicting. Only a few case reports and one retrospective study described PPI‑induced thrombocytopenia.19-22
To the best of our knowledge, there have been no studies analyzing the WBC count during PPI therapy. Neutropenia and agranulocytosis are rare adverse effects associated with PPI treatment. So far, only a few case reports of severe neutropenia or agranulocytosis during PPI use (ie, omeprazole) have been published.23-25
The suggested pathomechanisms of neutropenia includes immune reactions and cross‑reactivity. Also, synergic reactions with other potential causes of neutropenia should be considered. In our study, we observed a significantly lower WBC count in patients on PPI therapy than in controls, and only 2 patients had slight leukopenia. Further studies in patients on PPI therapy, with careful monitoring of WBC and its subpopulations, are needed.
It has been shown that gastric acid is required for the release of vitamin B12 from food; therefore, PPIs are believed to cause vitamin B12 deficiency. In our study, we did not measure serum vitamin B12 concentrations. However, in a cross‑sectional study, den Elzen et al26 reported that long‑term PPI use was not associated with vitamin B12 deficiency. On the other hand, Qorraj‑Bytyqi et al17 reported a change in serum cyanocobalamin concentrations at 1 year of PPI therapy.
To the best of our knowledge, there are no literature data on changes in MCV during PPI therapy. Despite differences in Fe levels between patients on PPI therapy and controls, we did not observe any differences in MCV. This finding can be explained by the multifactorial effect of various parameters on the size of erythrocytes. The values of MCV may be affected by Fe deficiency and vitamin B12 deficiency. An interesting observation is the positive correlation between Se levels and MCV, as well as the surprising lack of differences in these parameters between study groups. This relationship requires further research. The high concentration of Se in RBCs (higher than in most other blood fractions or whole blood),27 high activity of selenoenzyme glutathione peroxidase28 as well as Se transfer to and from hemoglobin29 have been already reported by various authors. However, the molecular mechanisms behind the positive correlation between plasma Se levels and RBC count remain to be fully clarified. Of note, Wasowicz and Zachara30 found a correlation between Se levels in erythrocytes and whole blood (r = 0.879; P <0.001).
Hypochlorhydria may contribute to decreased calcium and magnesium absorption and could have the same effect on other cations, such as Zn.1 It should be noted that plasma Zn levels are not affected by mild changes in dietary Zn, and only a significant and prolonged reduction of Zn intake leads to a notable deficiency.31 One study reported inhibited absorption of Zn during PPI therapy.32 On the other hand, Turnbull et al33 indicated that low gastric pH may not be necessary for intestinal absorption of Zn. Serfaty‑Lacrosniere et al34 did not find a difference in intestinal Zn absorption between omeprazole‑treated patients and controls. These observations seem to be in line with our results. Surprisingly, we showed higher serum Zn concentrations in PPI‑treated group than in controls. Moreover, Ergul et al35 showed a negative correlation between vitamin B12 levels and Zn deficiency. This suggests that Zn absorption may be a more complex issue than it has been considered so far. Importantly, Kirchoff et al36 indicated that Zn results in a rapid and prolonged reduction of gastric acid production. Perhaps the observed increase in Zn concentrations in the PPI group may be a manifestation of defense mechanisms in conditions associated with hypersecretion of acid regardless of PPI treatment.
The adverse consequence of Zn excess is Cu depletion.32 A reduction in the Cu level may lead to anemia, nerve damage, and bone loss.37 There are scarce and conflicting data on the effects of PPIs on Cu levels. Plantone et al38 hypothesized that a chronic and prolonged reduction of gastric acidity may reduce Cu absorption. Joshaghani et al39 showed no difference in serum Cu concentrations after 8 weeks of omeprazole use. On the other hand, Ece et al40 found that while hemoglobin values of children with iron‑deficiency anemia were decreasing, their serum Cu concentrations were increasing. Thus, an increase in Cu absorption occurs with increasing Fe deficiency. This is in line with our observations. Patients on PPI therapy in our study showed higher serum Cu levels and lower Fe levels in comparison with controls. Moreover, Cu and Zn levels in the PPI group were higher than in controls. This may indicate that a change in gastric pH may not be the only factor affecting the intestinal absorption of trace elements.
Selenium plays a major role in redox reactions and controls cell‑mediated immunity.41 Selenoproteins determine a protective mechanism against reactive oxygen and nitrogen species. High levels of this micronutrient may have a negative effect on carcinogenesis.42 Nezhad et al43 reported higher Se levels in patients with functional dyspepsia in comparison with those with gastric cancer. Ustundag et al44 reported that Se collected in gastric tissue in patients with Helicobacter pylori–related antral inflammation and then its levels decreased after effective H. pylori eradication. Wu et al45 also reported a reduction in serum Se levels after H. pylori eradication. To our knowledge, there are currently no reports of the PPI impact on Se status. The changes of microbiota in the small intestine because of prolonged PPI treatment may play an important role in the regulation of serum Se levels, because it is mostly absorbed in the duodenum and cecum by active transport through a sodium pump.46 Despite this, we found no difference in Se concentrations between our groups.
Proton‑pump inhibitors may interact with other drugs by reducing gastric acidity, modifying metabolism (generally through the cytochrome P450 enzyme system), or inhibiting extragastric renal proton pumps.47 In order to exclude these potential interactions, patients with serious concomitant conditions requiring use of immunosuppressive, antiviral, selective serotonin reuptake inhibitor treatment or chemotherapy were excluded from the study.
It is understood that short‑time use of over‑the‑counter PPIs does not have any deleterious effect on the absorption of micronutrients such as Fe, calcium, magnesium, and vitamin B1247; however, prescription PPIs in our study were generally administered at higher doses and the durations of treatment were longer.
Our results may indicate that the concentrations of micronutrients such as Zn, Se, or Cu in patients taking PPIs are not only dependent on their absorption potentially impaired due to the reduction of gastric acidity. We hypothesize that their concentrations can be affected also by other factors, such as oxidative stress. All the above trace elements are potent antioxidants involved in the oxidant defense system. On the other hand, gastroprotective effects of PPIs cannot only be explained by their antisecretory function. Recent studies have shown a more direct effect of omeprazole on the integrity of gastric mucosa, including antiapoptotic, anti‑inflammatory, and free radical scavenging functions.48 Because the emerging evidence indicates an involvement of reactive oxygen species in the pathomechanism of gastric lesions,48 the antioxidant actions of PPIs might produce the noted acid‑independent gastroprotective effects. Becker et al49 demonstrated that heme oxygenase‑1 is an antioxidant mediator of PPIs in gastric epithelial cells as well as vascular endothelial cells. High‑dose PPIs have shown promise as chemopreventive agents for esophageal adenocarcinoma in Barrett esophagus fitting with the hypothesis that this cancer is an inflammatory‑mediated malignant response to prolonged acid exposure.50 The involvement of Zn, Se, and Cu in a potential antioxidant reaction induced by PPIs requires further research.
Conclusions
Our findings show that PPIs should be prescribed with caution and awareness. Prolonged PPI use affects complete blood count, in particular RBCs and WBCs. Moreover, PPIs cause changes in iron absorption, with subsequent changes in RBC count and hemoglobin levels.
Monitoring of prolonged therapy should be introduced, particularly in the population of elderly or malnourished patients. Inappropriate PPI use may result in significant adverse effects and potential interactions. Awareness of evidence‑based guidelines and targeted medicine prescription strategies are essential for cost‑effective and safe use of this drug class. Patients overusing PPIs should be screened and properly educated about guideline recommendations and indications for prescription.
The concentrations of some micronutrients may change as a result of PPI use, although the mechanism of this phenomenon is complex and not fully clear. The antioxidant functions of PPIs might account for the noted acid‑independent gastroprotective effects. The involvement of Zn, Se, and Cu in a potential antioxidant reaction induced by a PPI requires further research. Comparative studies on the concentrations of these micronutrients before and after the PPI therapy are needed. Further studies with higher number of enrolled patients with a uniform distribution of age between the groups to support our preliminary observations are necessary.
- Nguyen PV, Tamaz R. Inappropriate prescription of proton pump inhibitors in a community setting. Can J Hosp Pharm. 2018; 71: 267‑271. | Crossref
- Safer DJ. Overprescribed medications for US adults: four major examples. J Clin Med Res. 2019; 11: 617‑622. | Crossref
- Kelly OB, Dillane C, Patchett SE, et al. The inappropriate prescription of oral proton pump inhibitors in the hospital setting: a prospective cross‑sectional study. Dig Dis Sci. 2015; 60: 2280‑2286. | Crossref
- Maes ML, Fixen DR, Linnebur SA. Adverse effects of proton‑pump inhibitor use in older adults: a review of the evidence. Ther Adv Drug Saf. 2017; 8: 273‑297. | Crossref
- De Roza MA, Kai L, Wen Kam J, et al. Proton pump inhibitor use increases mortality and hepatic decompensation in liver cirrhosis. World J Gastroenterol. 2019; 25: 4933‑4944. | Crossref
ARTICLE INFORMATION