Serum hypoxia-inducible factor-1α protein level as a diagnostic marker of obstructive sleep apnea



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Serum hypoxia-inducible factor-1α protein level as a diagnostic marker of obstructive sleep apnea
Introduction
The prevalence of obstructive sleep apnea (OSA) syndrome has greatly increased in recent years. It is estimated that almost 50% of men and 24% of women are affected by at least moderate OSA (apnea–hypopnea index [AHI] ≥15/h).1 Multiple screening tools have been developed to assess the risk of OSA, including various questionnaires2 and parameters (eg, body mass index).3 Similarly, there is an ongoing search for biochemical markers that might serve as predictors of the disorder. However, currently, none of them has a high predictive value for the diagnosis of OSA.4,5
One of the typical complications of OSA is intermittent hypoxemia, which manifests as desaturations on polysomnography.6 Hypoxia‑inducible factor 1 (HIF‑1) is a key regulator of cellular oxygen metabolism. It consists of 2 subunits: α, which is oxygen sensitive, and β, which is produced in a continuous manner and is not oxygen dependent. Since hypoxia is characteristic for rapidly proliferating tissues, such as tumor tissue, a considerable number of studies investigating HIF‑1α focused on its effect on the formation and growth of tumor tissue. An increased expression of HIF‑1α was observed in multiple cancers and correlated with a worse prognosis.7 The protein is also thought to be responsible for activation of a vast number of genes. For example, it activates genes associated with angiogenesis (eg, vascular endothelial growth factor) or glucose uptake by cells (glucose transporters 1 and 3).7 This explains the mechanisms whereby HIF‑1α is involved in tumor progression and suggests its possible role in the development of OSA comorbidities. Thus, HIF‑1α protein is a potential candidate for a diagnostic marker in OSA. In this study, we aimed to assess the value of the serum HIF‑1α level as a predictor of OSA.
Patients and methods The study group included 84 patients who were referred to Sleep and Respiratory Disorders Center in Łódź (Poland) with a presumptive diagnosis of OSA. All patients underwent standard nocturnal polysomnography examination (Jaeger, Viasys Healthcare, Höchberg, Germany), and the results were scored according to the American Academy of Sleep Medicine guidelines.8 Patients with chronic respiratory disorders (such as bronchial asthma, chronic obstructive pulmonary disease, or any chronic pulmonary disorder resulting in respiratory failure) were excluded from the study, as individuals with these conditions have been shown to have increased serum HIF‑1α protein levels.9 Other exclusion criteria were chronic inflammatory diseases (such as lupus or inflammatory bowel disease), infection within 1 month of blood collection, and diagnosis of cancer (active or in medical history). Peripheral blood samples were collected in the evening before and in the morning after polysomnography, and then centrifuged. Serum was collected and stored at a temperature of –80ºC. The HIF‑1α concentration was assessed using an enzyme‑linked immunosorbent assay kit (Invitrogen, Carlsbad, California, United States).
The study was approved by the Ethics Committee of the Medical University of Lodz (RNN/77/18/KE). All patients provided written informed consent to participate in the study. Statistical analysis was performed with Statistica 13.1 (StatSoft, Tulsa, Oklahoma, United States). The receiver operating curve was created to assess the value of serum HIF‑1α concentrations as a predictor of OSA.
Results
The severity of OSA was assessed on the basis of AHI.8 In 24 patients (28.6%), the AHI was lower than 5 (healthy controls). Mild (15> AHI ≥5), moderate (30> AHI ≥15), and severe OSA (AHI ≥30) was reported in 17 (20.2%), 19 (22.6%), and 24 patients (28.6%), respectively.
The median HIF‑1α protein concentration in the morning was 1252.6 pg/ml (interquartile range, 762.3–1795.4 pg/ml). Based on the Youden index, the cutoff point of 1055.6 pg/ml was chosen as having the best diagnostic value in OSA (AHI ≥5) (Figure 1). The calculated area under the curve (AUC) was 0.841 (95% CI, 0.753–0.929; P <0.001). For this cutoff point, the sensitivity, specificity, as well as positive (PPV) and negative predictive values (NPV) were 80%, 83%, 92%, and 63%, respectively. Furthermore, the cutoff points of serum HIF‑1α concentrations for at least moderate and severe OSA were 1055.6 pg/ml and 1694.4 pg/ml, with an AUC of 0.689 (95% CI, 0.583–0.813; P <0.001) and 0.62 (95% CI, 0.478–0.762; P = 0.098), respectively, with lower diagnostic values than in the case of AHI of 5 or higher (data not shown).
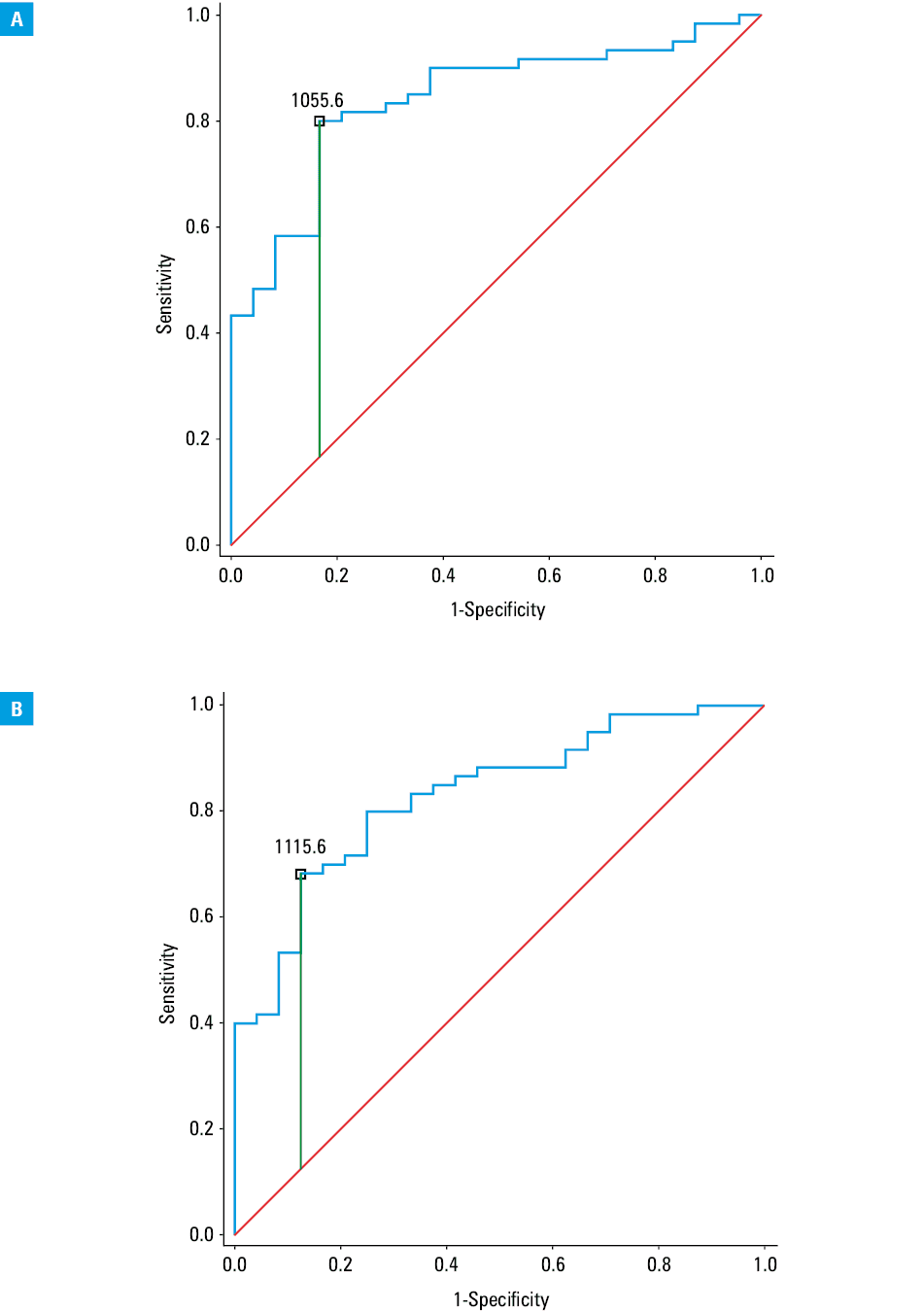
Similar results were obtained for serum HIF‑1α protein concentrations in the evening, with a median of 1178.8 pg/ml (interquartile range, 851.1–1876.9; P = 0.601), which suggests circadian stability. Based on the Youden index, the cutoff point of 1115.6 pg/ml was chosen as having the best diagnostic value. The AUC was 0.831 (95% CI, 0.740–0.921; P <0.001). For this cutoff point, the sensitivity, specificity, PPV, and NPV were 68%, 88%, 93%, and 53%, respectively.
The absence of HIF‑1α protein upregulation should possibly have a high NPV in the diagnosis of OSA. In our study, chronic hypoxemia unrelated to OSA was excluded with high probability by the negative history of chronic lung diseases and normal blood oxygen saturation. Consequently, in our group of patients that excluded those with hypoxemia unrelated to OSA, the specificity of HIF‑1α protein might have increased. We analyzed the diagnostic utility of morning serum HIF‑1α concentrations at standard AHI cutoff values of 5, 15, and 30. The pretest probability of OSA was 71.4%, which was similar to the value obtained in a large cohort of over 1000 patients from our sleep laboratory.3 At the level of at least 1750 pg/ml, HIF‑1α was not sensitive (38%), but had a specificity of 100%, which resulted in a PPV of 100%. Fifty‑one percent of patients had at least moderate OSA. In this group, the highest PPV was observed for the same level of HIF‑1α (1750 pg/ml), but it was only 78% due to a lower specificity of 88%. The prevalence of severe OSA was 28.6% and specificity reached 80% at this cutoff value, which resulted in a PPV of only 48%.
On the other hand, the highest NPV for at least mild OSA was observed at a HIF‑1α level of 750 pg/ml and reached 68%. Similar results were obtained for at least moderate OSA. The highest NPV of 82% was observed for severe OSA at a HIF‑1α level of 1500 pg/ml.
Discussion
Currently, there is no biochemical marker useful in the diagnosis of OSA. One of the proposed markers is C‑reactive protein (CRP). A meta‑analysis revealed a significantly higher level of both CRP and high‑sensitivity CRP (hs‑CRP) among patients with moderate OSA in comparison with healthy controls.10 However, the AUC calculated for CRP and hs‑CRP was under 0.8: 0.73 mg/l (95% CI, 0.60–0.85) and 0.72 mg/l (95% CI, 0.63–0.81), respectively.4,10 These AUC values were lower than those obtained in our study for HIF‑1α protein. Similar values to CRP or lower were obtained for glycated hemoglobin, interleukin 6, and erythropoietin.11 The diagnostic panel including these variables revealed an AUC of 0.84 (95% CI, 0.75–0.94).11 Subsequent validation on a new patient group showed an AUC of 0.78 (95% CI, 0.71–0.86).4 In a recent study, Lebkuchen et al12 described a metabolomic and lipidomic profile among male patients with OSA. However, none of the metabolomic parameters had an AUC over 0.7. Higher results were obtained for lipidomic parameters, with the highest AUC reaching 0.73 (95% CI, 0.578–0.882).12
The obtained diagnostic values of HIF‑1α protein levels indicate the usefulness of this parameter in comparison with the currently proposed biomarkers and scales.2,4 Serum HIF‑1α concentrations may be a quite specific marker of OSA provided that other chronic causes of hypoxemia are excluded. High HIF‑1α levels (≥1750 pg/ml) were observed only in patients with the diagnosis of OSA, which resulted in a relatively high PPV. Conversely, at any level of this marker, false negative results reduced the NPV. In conclusion, high serum levels of HIF‑1α protein are compatible with the diagnosis of OSA, while low levels can exclude severe OSA with high probability. However, our findings are limited to the population with specific exclusion criteria, and further research is needed to extrapolate the results to a more general population.
- Heinzer R, Vat S, Marques‑Vidal P, et al. Prevalence of sleep‑disordered breathing in the general population: the HypnoLaus study. Lancet Respir Med. 2015; 3: 310‑318. | Crossref
- Prasad KT, Sehgal IS, Agarwal R, et al. Assessing the likelihood of obstructive sleep apnea: a comparison of nine screening questionnaires. Sleep Breath. 2017; 21: 909‑917. | Crossref
- Mokros Ł, Kuczynski W, Gabryelska A, et al. High negative predictive value of normal body mass index for obstructive sleep apnea in the lateral sleeping position. J Clin Sleep Med. 2018; 14: 985‑990. | Crossref
- Fleming WE, Holty J‑EC, Bogan RK, et al. Use of blood biomarkers to screen for obstructive sleep apnea. Nat Sci Sleep. 2018; 10: 159‑167. | Crossref
- Bromińska B, Cyrańska‑Chyrek E, Kuźnar‑Kamińska B, et al. Association between bone remodeling and inflammatory markers in obstructive sleep apnea in relation to disease severity. Pol Arch Intern Med. 2018; 128: 9‑14. | Crossref
ARTICLE INFORMATION