Three-dimensional printed trachea helps develop tailored treatment for tracheobronchomalacia



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Three-dimensional printed trachea helps develop tailored treatment for tracheobronchomalacia
Tracheobronchomalacia is a rare disease of the central airways, which manifests with impaired ventilation with expiratory collapse of the tracheal wall.1 Patients with severe symptoms and confirmed obstruction of the central airways can be offered surgical treatment, namely, tracheobronchoplasty.
A 39‑year‑old male patient presented with diabetes and asthma. He required multiple hospitalizations due to exacerbations of respiratory failure. He also reported distressing symptoms, such as recurrent episodes of wheezing, cough, and shortness of breath. Further diagnostic workup revealed tracheobronchomalacia with the dynamic narrowing of the thoracic trachea and main bronchi.
Chest computed tomography (CT) with respiratory phase gating (4D‑CT) and bronchoscopy showed the narrowing of the airways during the expiratory phase (Figure 1A–1C). Before the surgery, we performed 3‑dimensional (3D) visualization and developed the airway pattern (Figure 1D). The pattern was then transformed to a 3D‑printed plastic model, using the AW program (GE Healthcare, Chicago, Illinois, United States), Inventor Software (Autodesk, San Rafael, California, United States), and Prime3D software (Monkeyfab, Warsaw, Poland), and the model was printed using polylactide filament (Figure 1E).2
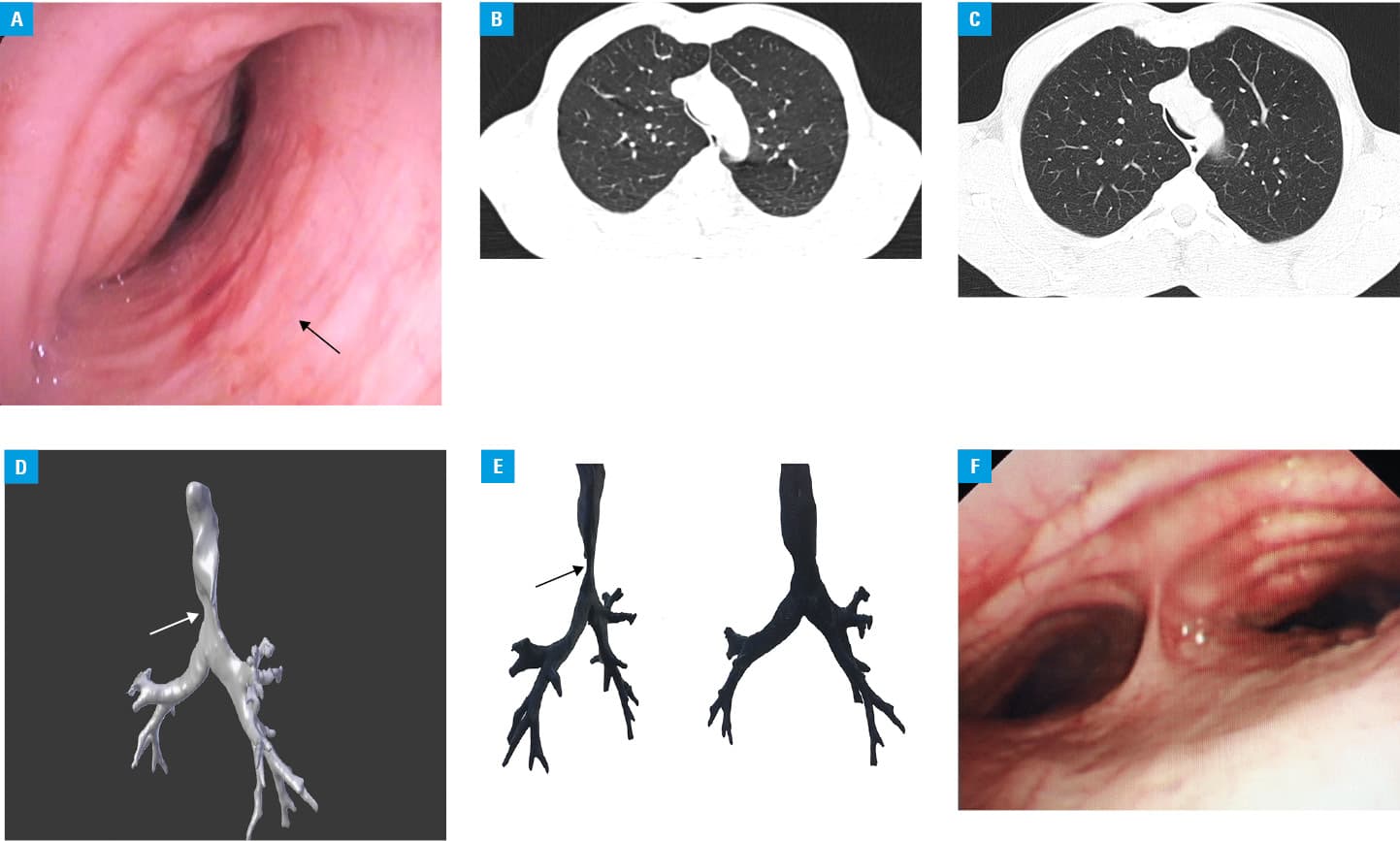
Using right posterolateral thoracotomy, the trachea and main bronchi were exposed after ligation of the azygous vein. The membranous wall of the trachea and main bronchi was plicated and narrowed with polypropylene mesh by a series of 4 mattress sutures. A narrowing of the membranous wall was obtained, which resulted in a satisfactory widening of the trachea and main bronchi (Figure 1F). The patient was extubated on the first day and required bronchoscopic aspiration as well as antibiotic therapy due to respiratory infection.
Control bronchoscopy at 3, 6, and 12 months after the operation showed satisfactory widening of the airways. Although there was no significant change in spirometry results (forced expiratory volume in 1 second, 33% vs 27%), the patient reported a considerable improvement after surgery. The St. George’s Respiratory Questionnaire (SGRQ) indicated that the symptoms subsided and the patient remained asymptomatic for more than 1 year after the operation. Before surgery, the components of the SGRQ test, namely, Symptoms Score, Activity Score, Impact Score, and Total Score were 95, 93, 94, and 94, respectively, as compared with 49, 30, 8, and 22, respectively, at more than 1 year after procedure.
Tracheobronchoplasty, by which the mesh is sewn into the membranous wall, is considered to be an effective treatment option for tracheobronchomalacia.3,4 It requires a meticulous preparation and design of implanted materials before surgery. The 4D‑CT reconstruction enables a visualization of the tracheal shape and helps design meshes and rings that should be prepared in detail due to anticipated anatomical circumstances. Low resolution and inability to directly create a 3D model are the main limitations of CT, so it was considered insufficient in our patient. The solution in such cases is rapid prototyping. The 3D printing of the trachea further facilitates performing surgery. As tracheobronchomalacia is a rare condition and our patient presented with an exceptionally wide extension of the membranous wall, we decided to search for any available means to effectively plan the surgery.
In conclusion, the 3D model of the airways printed in advance of a nonstandard surgical strategy can facilitate tailoring therapy.
- Murgu SD, Colt HG. Tracheobronchomalacia and excessive dynamic airway collapse. Respirology. 2006; 11: 388‑406. | Crossref
- Rengier F, Mehndiratta A, von Tengg‑Kobligk H, et al. 3D printing based on imaging data: review of medical applications. Int J Comput Assist Radiol Surg. 2010; 5: 335‑341. | Crossref
- Wright CD, Mathisen DJ. Tracheobronchoplasty for tracheomalacia. Ann Cardiothorac Surg. 2018; 7: 261‑265. | Crossref
- Grillo HC. Surgery for tracheomalacia, tracheopathia osteoplastica, tracheal compression, and staged reconstruction of the trachea. In: Grillo HC. Surgery of the Trachea and Bronchi. Hamilton, Ontario: BC Decker Inc; 2004: 645‑663.
ARTICLE INFORMATION