Primary splenic angiosarcoma: a very rare and aggressive neoplasm with a poor prognosis



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Primary splenic angiosarcoma: a very rare and aggressive neoplasm with a poor prognosis
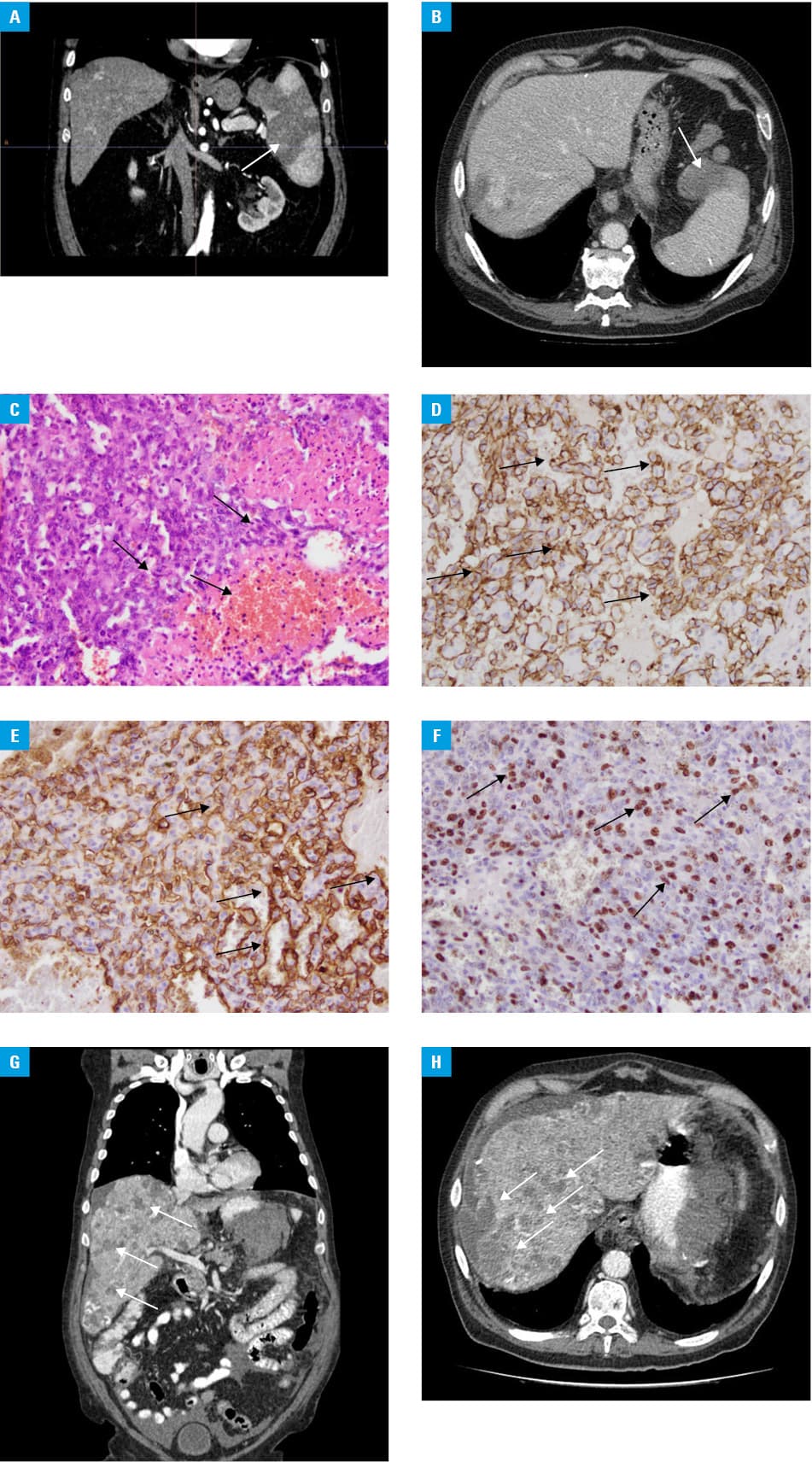
A 78‑year‑old man was admitted to hospital due to persistent pain in the left side of the abdomen and under the left scapula. On physical examination tenderness on palpation in the left epigastric region was observed. Laboratory tests showed: normocytic anemia, red blood cell count of 3.72 × 106/μl, thrombocytopenia (platelet count, 90 × 103/μl), increased alkaline phosphatase (277 U/I; reference range 40–129U/I), D‑dimer level of 5055 ng/ml (reference range 0–500 ng/ml), C reactive‑protein level of 23.09 mg/l (reference range, 0–5 mg/l), and elevated erythrocyte sedimentation rate of 160 mm/h. First abdominal ultrasound revealed an enlargement of the spleen (150 × 87 mm) with a focal angioma‑like lesion in the lower part. In the central segment of the spleen, another area with an increased echogenicity, 45 × 46 mm, surrounded by a thoroughly encapsulated surface was found, which may indicate hematoma around the angioma. An abdominal computed tomography scan revealed an enlarged spleen (up to 145 mm in the longest axis) with multiple heterogeneous focal lesions of different sizes affecting a significant part of the splenic parenchyma and remarkably distorting its outer outline (Figure 1A and 1B). Due to persisting pain in the left subcostal region of the abdomen, another ultrasound was performed (16 days after the first examination). It showed that the angioma‑like lesion in the central segment of the spleen increased in size (81 × 54 × 68 mm). The patient was transferred to the Department of General and Vascular Surgery, where he was qualified for splenectomy. The histopathological examination of the resected spleen, microscopic evaluation, and immunohistochemical profile (CD34+, CD31+, cytokeratin CK AE1/AE3, Ki67 proliferation index about 60%—in the fields of the highest activity) indicated splenic angiosarcoma (Figure 1C-1F). Three weeks after the diagnosis, computed tomography of the chest, abdomen, and pelvis showed numerous small liver metastatic lesions and an infiltration of the gastric and peritoneal region (Figure 1G and 1H). The patient died a few weeks later.
Primary splenic angiosarcoma is a very rare malignant neoplasm arising from splenic endothelial cells. The annual incidence rate of the neoplasm is between 0.14 and 0.25 of cases per 1 million individuals with the peak incidence in patients aged 50 to 60 years.1,2 Its pathogenesis still remains unknown. Some authors claim that angiosarcoma can be a result of benign lesions such as hemangioma and hemangioendothelioma. There is also some data on the impact of toxic substances such as thorium, arsenic, and vinyl chloride on the risk of developing angiosarcoma.2 Splenic angiosarcoma does not have specific clinical signs. The only symptom occurring in over 80% of patients is nonspecific pain in the left epigastric area. Splenic rupture is sometimes the only manifestation of splenic angiosarcoma.3 The prevalence of metastasis in this disease ranges from 69% to 100%, and the main organs usually involved are the liver (89%), lungs (78%), lymph nodes (56%), and bones (22%). Like in most angiosarcoma, surgical resection is the main treatment. Early adjuvant chemotherapy is highly unlikely to inhibit the metastatic potential of angiosarcoma.4 The average survival is 12 months since diagnosis.5 Splenic angiosarcoma should be suspected in each patient with atypical pain in the left subcostal area, an enlarged spleen with atypical focal lesions, thrombocytopenia, and anemia of unknown etiology.
- Fotiadis C, Georgopoulos I, Stoidis C, Patapis P. Primary tumors of the spleen. Int J Biomed Sci. 2009; 5: 85‑91.
- Myoteri D, Despoina M, Dellaportas D, et al. Primary angiosarcoma of the spleen: an oncological enigma. Case Rep in Oncol Med. 2014; 193036.
- Coppola S, Leva A, Pagni F, et al. Demanding diagnosis of splenic angiosarcoma as cause of delayed treatment of spontaneous splenic rupture: a case report and literature review. Case Rep Surg. 2017; 2017: 6256102. | Crossref
- Kudlicki J, Kania A, Frania‑Baryluk A, et al. Right atrial angiosarcoma in a pregnant woman: diagnostic and therapeutic dilemmas. Pol Arch Intern Med. 2018; 128: 129‑131. | Crossref
- Hara T, Tsurumi H, Kasahara S, et al. Long‑term survival of a patient with splenic angiosarcoma after resection, high dose chemotherapy, and autologous peripheral blood stem cell transplantation. Intern Med. 2010; 49: 2253‑2257. | Crossref
ARTICLE INFORMATION