A 75‑year‑old woman, who had undergone appendectomy in the 1980s, was admitted to our department in November 2018 for endoscopic removal of an ileocecal polyp diagnosed during routine colonoscopy in September 2018. The patient complained of pain in the right lower abdomen and episodes of lower gastrointestinal bleeding for approximately 5 years. During this period, she had lost around 20 kg in weight.
The first colonoscopy performed in March 2013 detected a large polyp of the ileocecal valve. However, repeat colonoscopy in September 2013 and February 2014 did not show the polyp. Contrast‑enhanced computed tomography of the abdomen and pelvis performed in June 2014 did not reveal any abnormalities. Due to persistent gastrointestinal bleeding, the patient underwent another colonoscopy in January 2016, which showed a polypoid lesion in the ileocecal valve. A colonoscopy performed in April 2016 revealed normal appearance of the cecum and distal part of the ileum. However, the pain in the right lower abdomen and intermittent lower gastrointestinal bleeding persisted. Therefore, in August 2018, another colonoscopy was scheduled, which showed a cecal polyp.
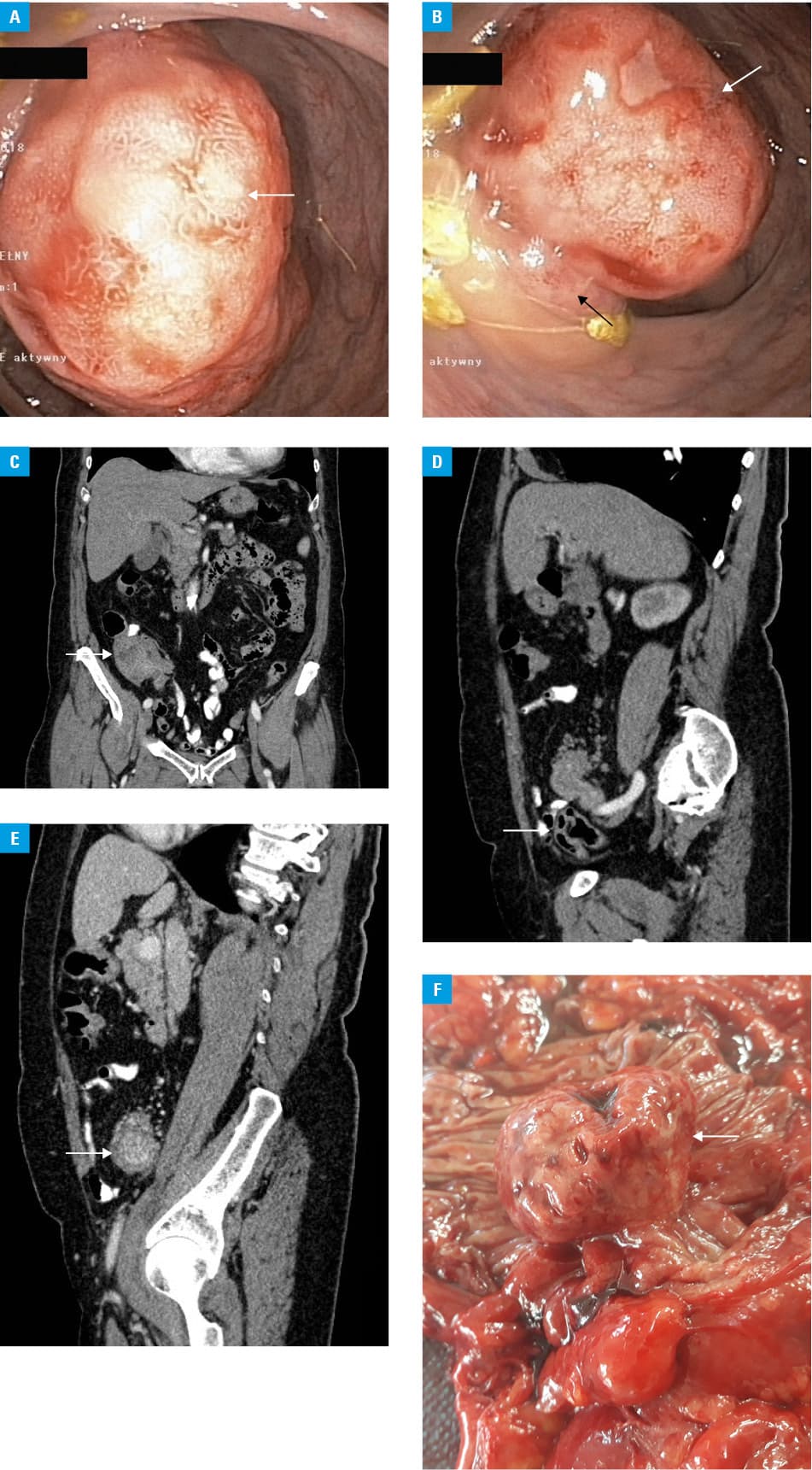
The patient was referred to our department for endoscopic treatment. A colonoscopy performed in October 2018 revealed an ileal tumor (Figure 1A and 1B), which suggested intussusception of the distal part of the ileum through the ileocecal valve and into the lumen of the cecum. Abdominal and pelvic contrast‑enhanced computed tomography confirmed the diagnosis (Figure 1C–1E). The patient was referred for surgical treatment. A laparoscopic right hemicolectomy was performed. Intraoperative examination revealed intussusception of the distal ileum through the ileocecal valve and a coexisting ileal tumor, which acted as a pathological lead point (Figure 1F). No complications occurred in the postoperative period. The patient was discharged in good condition on the fourth postoperative day. Histopathologic examination of the specimen confirmed the neuroendocrine tumor of the ileum (T3N1M0 according to the TNM classification; carcinoid CD56(+) Ki67(+) in less than 2% of tumor cells). The patient was followed in an outpatient clinic, and subsequent imaging studies did not reveal any signs of cancer recurrence.
Intussusception is a telescoping of the proximal part of the intestine into its distal part, which is rarely detected in adult patients.1,2 In most cases, it is an acute condition that requires immediate surgical intervention.3 Chronic intussusception is rarely reported.4,5 However, in our case, chronic intussusception of the ileum through the ileocecal valve was diagnosed on the basis of clinical presentation, additional diagnostic tests, and histopathologic examination. At the early stage of the disease, intermittent intussusceptions of the ileum through the ileocecal valve occurred. Progression of an endocrine‑inactive ileal tumor and a gradual increase in tumor volume, which was the anatomical cause of the intussusception and which acted as a pathological lead point, resulted in a very rare medical condition, namely, chronic intussusception.
- Sivit CJ. Gastrointestinal emergencies in older infants and children. Radiol Clin North Am. 1997; 35: 865‑877.
- Sorantin E, Lindbichler F. Management of intussusception. Eur Radiol. 2004; 14: 146‑154. | Crossref
- Bisset GS 3rd, Kirks DR. Intussusception in infants and children: diagnosis and therapy. Radiology. 1988; 168: 141‑145. | Crossref
- Rees BI, Lari J. Chronic intussusception in children. Br J Surg. 1976; 63: 33‑35. | Crossref
- Jawad AJ, Shibli SY, Sahni PS, Malabarey T. Chronic intussusception. Ann Saudi Med. 1997; 17: 545‑547. | Crossref
ARTICLE INFORMATION