Endoscopic treatment of walled-off pancreatic necrosis complicated by delayed splenic artery hemorrhage



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Endoscopic treatment of walled-off pancreatic necrosis complicated by delayed splenic artery hemorrhage
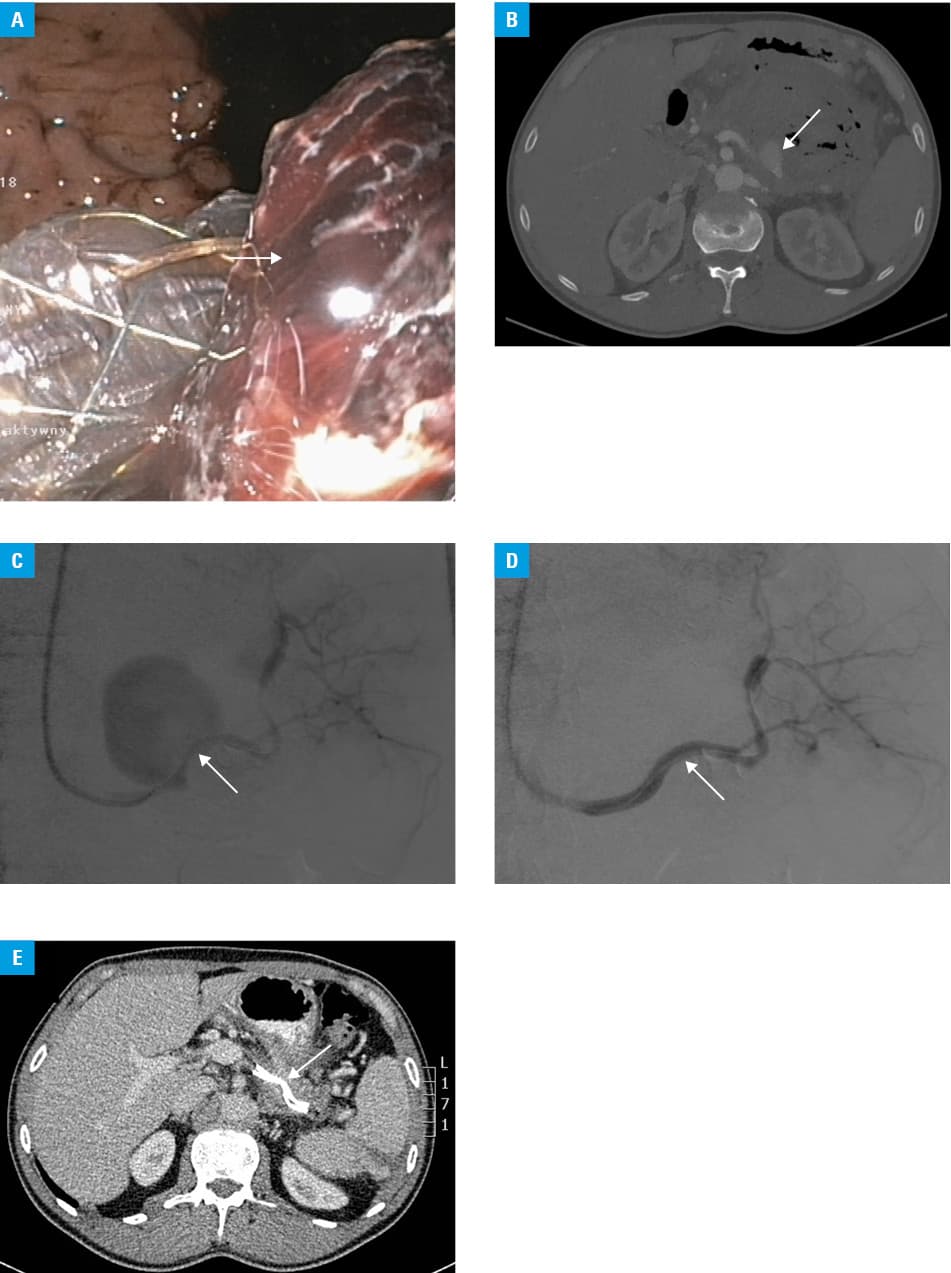
A 44‑year‑old man with a history of acute necrotizing alcohol–related pancreatitis diagnosed 8 weeks earlier was admitted to our department to undergo interventional treatment for symptomatic walled‑off pancreatic necrosis (WOPN). Contrast‑enhanced computed tomography (CECT) of the abdomen and pelvis revealed a necrotic collection (130 × 97 × 82 mm in size) in the pancreatic area. The patient underwent endoscopic transmural drainage of the WOPN, and a lumen‑apposing metal stent (LAMS; NAGI Stent 20 × 16 mm, TaeWoong, South Korea) was inserted through the gastric wall under endoscopic ultrasound guidance. Signs of upper gastrointestinal bleeding appeared on day 4 of passive endoscopic drainage, including hematemesis and melena, and laboratory blood test results indicated anemia. Gastroscopy (Figure 1A) showed biliary contents in the stomach. Moreover, a completely obstructed transmural endoprosthesis containing numerous blood clots was observed. Abdominal CECT revealed a necrotic collection (115 × 97 × 77 mm in size), filling with a contrast agent and escaping from a perforated splenic artery (Figure 1B). Therefore, the patient was eligible for endovascular treatment. Access through the left brachial artery was obtained, and a contrast agent was injected into the splenic artery, which confirmed leakage of contrast into the lumen of the WOPN (Figure 1C). However, the contrast agent did not flow into the gastric lumen due to transmural endoprosthesis obstruction. A stentgraft (BeGraft peripheral 6 × 58 mm, Bentley, Germany) was inserted into the splenic artery to bridge the site of contrast leakage in the vascular wall. Control arteriography did not show any signs of contrast media extravasation (Figure 1D). On hospital day 8, the patient’s general condition improved; therefore, endotherapy was continued. An endoscopic procedure was undertaken to unclog the transmural stent and insert a gastroscope through its lumen to gain access to the WOPN. The necrotic collection was flushed, resulting in the outflow of a large number of blood clots. Two plastic stents were inserted through the lumen of the LAMS. Passive transmural drainage continued for 48 additional days. Following control abdominal CECT (Figure 1E) that showed complete regression of the WOPN and symptom resolution without signs of recurrent gastrointestinal bleeding, endoscopic treatment was terminated and the stents were removed during an endoscopic procedure.
Endoscopic WOPN drainage is an effective therapeutic approach.1 Using a LAMS for transmural drainage improves endotherapy results,1 but some publications described an increased number of adverse events related to LAMS.2 Massive bleeding from a perforated splenic artery is associated with high mortality rates.3,4 In the present case, perforation of the artery was a result of pancreatic juice affecting the vascular wall, as well as a drop in pressure within the necrotic collection following transmural cystostomy during the drainage procedure. Obstruction of the transmural metal stent prevented blood from entering the gastric lumen and limited the bleeding. Inserting a stentgraft into the splenic artery enabled us to control the bleeding to the necrotic collection and to continue endoscopic treatment. To the best of our knowledge, this is the first report of a successful endoscopic drainage of the WOPN complicated by delayed massive hemorrhage from a ruptured splenic artery treated with endovascular stent grafting.5
- Arvanitakis M, Dumonceau J‑M, Albert J, et al. Endoscopic management of acute necrotizing pancreatitis: European Society of Gastrointestinal Endoscopy (ESGE) evidence‑based multidisciplinary guidelines. Endoscopy. 2018; 50: 524‑546. | Crossref
- Kozieł M, Jagielski M, Jarczyk G, et al. A rare case of a spontaneous duodenum fistula in a patient on endoscopic ultrasound‑guided treatment of large walled‑off pancreatic necrosis. Pol Arch Intern Med. 2018; 128: 704‑705. | Crossref
- Berek P, Stefanic P. Surgical treatment of splenic artery aneurysm. Eur J Vasc Endovasc Surg. 2017; 54: 11. | Crossref
- Barrionuevo P, Malas MB, Nejim B, et al. A systematic review and meta‑analysis of the management of visceral artery aneurysms. J Vasc Surg. 2019; 70: 1694‑1699. | Crossref
- Ouchi T, Kato N, Nakajima K, et al. Splenic artery aneurysm treated with endovascular stent grafting: a case report and review of literature. Vasc Endovascular Surg. 2018; 52: 663‑668. | Crossref
ARTICLE INFORMATION