Bleeding in anticoagulated patients with atrial fibrillation: practical considerations
Key words: anticoagulation, atrial fibrillation, biomarkers, bleeding, comorbidities



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Bleeding in anticoagulated patients with atrial fibrillation: practical considerations
Major bleeding (especially intracranial hemorrhage) is the most feared adverse event observed in patients with atrial fibrillation (AF) receiving oral anticoagulation. Clinical risk factor–based scores have modest ability to predict major or clinically relevant bleeds, and blood biomarkers are increasingly implemented to improve bleeding prognostication in patients with AF on life‑long anticoagulation. To improve the safety of anticoagulation in the era of non–vitamin K antagonist oral anticoagulants (NOACs, or direct oral anticoagulants [DOACs], including dabigatran, rivaroxaban, apixaban, and edoxaban), specific demographic, clinical, and laboratory variables should be considered. The current review summarizes practical challenges in the management of oral anticoagulation with emphasis on the risk assessment tools, elderly or underweight patients, cancer patients, impact of chronic kidney disease, liver cirrhosis, and thrombocytopenia in the context of bleeding risk in patients with AF.
Introduction
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia in clinical practice, and it is associated with an increased risk of ischemic stroke and systemic thromboembolism (SE) from less than 1% to about 20% per year.1 Of all ischemic strokes, 20% to 30% are associated with AF and high morbidity and mortality. Oral anticoagulation therapy reduces the risk of stroke and SE by more than 60% in patients with AF,2,3 yet clinicians and patients need to consider these benefits as compared with the risk of major bleeding.4
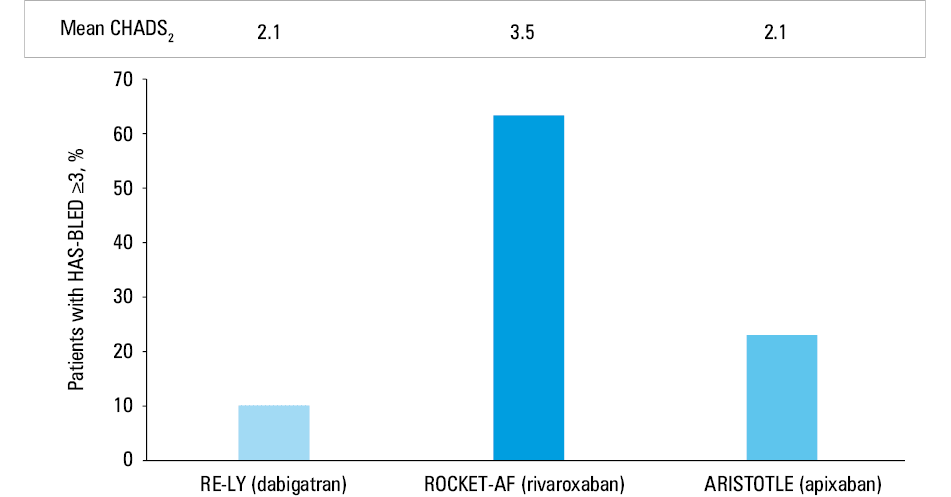
Non–vitamin K antagonist oral anticoagulants (NOACs, or direct oral anticoagulants [DOACs] as recommended by the International Society on Thrombosis and Hemostasis [ISTH], including dabigatran, rivaroxaban, apixaban, and edoxaban), have been shown in landmark phase 3 randomized trials to be at least noninferior to warfarin for the prevention of stroke and SE and are preferred over warfarin in patients with nonvalvular AF.5,6 When compared with vitamin K antagonist (VKA), the efficacy of NOACs is similar or higher, but they are safer and more convenient.7,8 In a meta‑analysis of pivotal phase 3 AF randomized controlled trials (RCTs), NOACs reduced the risk of stroke or SE by 19% compared with warfarin (relative risk [RR], 0.81; 95% CI, 0.73–0.91), largely due to a markedly lower rate of hemorrhagic strokes (RR 0.49, 95% CI, 0.38–0.64) and intracranial bleeding (ICB) (RR, 0.48; 95% CI, 0.39–0.59).9 However, the use of NOACs (in particular, full‑dose dabigatran and rivaroxaban) was significantly associated with an increased risk of gastrointestinal (GI) bleeding (RR, 1.25; 95% CI, 1.01–1.55).7 Of note, the differences between baseline stroke and bleeding risks among different NOAC trials could have affected the reported bleeding rates (Figure 1). Residual incidence of stroke or SE despite NOAC use among patients with AF is estimated at 1.5% to 2.5% per year and that of major bleeding at 2% to 4% per year.9 As compared with warfarin, NOACs slightly reduced all‑cause mortality (RR, 0.89; 95% CI, 0.85–0.94), vascular mortality (RR, 0.88; 95% CI, 0.82–0.94), and bleeding‑related mortality (RR, 0.54; 95% CI, 0.44–0.67).10 Importantly, in the phase 3 AF trials, NOACs were more effective than warfarin in the prevention of stroke or SE among patients with AF aged 75 years or older.11
A systematic review by Chai‑Adisaksopha et al,12 which included 12 RCTs involving 102607 patients at the average age of 70 to 73 years in the 5 AF trials and 54 to 57 years in the 7 venous thromboembolism (VTE) trials, clearly demonstrated that the incidence of ICB, the most feared hemorrhagic adverse event, in patients receiving NOACs is reduced by over 50% compared with warfarin. Of all major bleeding episodes among VKA users, 8.7% were ICB with a 46% to 55% mortality rate.13,14 Patients with AF or VTE on NOACs had a lower risk of overall major bleeding (RR, 0.72; number needed to treat [NNT], 156), fatal bleeding (RR, 0.53; NNT, 454), clinically relevant nonmajor bleeding (RR, 0.78; NNT, 99), and all bleeding (RR, 0.76; NNT, 18), without increased risk of GI bleeding (RR, 0.94; 95% CI, 0.88–1.34).12 Several systematic reviews comparing NOACs with standard care demonstrated a 20% higher GI bleeding rate in patients on a NOAC.15,16 A significant increase in the risk of GI bleeding was observed in the RCTs evaluating dabigatran and rivaroxaban in patients with AF.17,18 In the RE‑LY (Randomized Evaluation of Long‑Term Anticoagulation Therapy) trial, dabigatran 150 mg bid (but not dabigatran 110 mg bid) was associated with an increased risk of major GI bleeding compared with warfarin (RR, 1.50; 95% CI, 1.19–1.89),17 whereas in the ROCKET‑AF (Rivaroxaban Once‑daily Oral Direct Factor Xa Inhibition Compared with Vitamin K Antagonism for Prevention of Stroke and Embolism Trial in Atrial Fibrillation), rivaroxaban 20 mg once daily increased this annual risk by 1% (3.2% vs 2.2%).18 Of note, NOAC‑associated GI bleeding is probably related to the presence of the active drug in the GI tract, thus facilitating bleeding from vulnerable lesions.19
Scoring systems to predict bleeding in atrial fibrillation
The most commonly used definition of major bleeding in nonsurgical patients according to the ISTH includes:
1 fatal bleeding, and/or
2 symptomatic bleeding in a critical area or organ, for example, intracranial, intraspinal, intraocular, retroperitoneal, intraarticular or pericardial, or intramuscular bleeding with compartment syndrome, and/or
3 bleeding accompanied by a decrease in the hemoglobin level of 2 g/dl or higher or leading to transfusion of 2 or more units of whole bloodor packed red blood cells.20
The annual rates of major bleeding range from 1.3% to 7.2% in patients with AF on VKA treatment.21 Various bleeding risk scores (Table 1) have been developed to assess the risk of bleeding in patients with AF taking oral anticoagulant therapy.22,23 All these scores have a relatively modest ability to predict bleeding events (as reflected by the C statistic values in the range from 0.50 to 0.65), and numerous studies comparing 2 or more bleeding risk scores yielded conflicting results.24-33 In a systemic review commissioned by the Patient‑Centered Outcomes Research Institute34 of 38 studies on bleeding risk prediction, the HAS‑BLED (hypertension, abnormal renal and/or liver function, history of stroke or thromboembolism, history of bleeding or bleeding diathesis [eg, severe anemia], age >65 years, use of aspirin or nonsteroidal anti‑inflammatory drugs, and alcohol abuse) score had the best evidence for predicting bleeding risk (moderate strength of evidence), consistent with other systematic reviews and meta‑analyses comparing bleeding risk prediction scores.35,36
Scale | Risk factors | Scoring point | Bleeding risk stratification |
Abbreviations: ATRIA, Anticoagulation and Risk Factors in Atrial Fibrillation; CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate; HEMORR2HAGES, Hepatic or Renal Disease, Ethanol Abuse, Malignancy, Older Age, Reduced Platelet Count or Function, Re‑Bleeding, Hypertension, Anemia, Genetic Factors, Excessive Fall Risk and Stroke; INR, international normalized ratio; NSAID, non‑steroidal anti‑inflammatory drug; ORBIT‑AF, Outcomes Registry for Better Informed Treatment of Atrial Fibrillation; SBP, systolic blood pressure; TIA, transient ischemic attack; others, see Figure 1 | |||
HAS‑BLED | Hypertension (SBP >160 mm Hg) | 1 | Low risk, 0–2
High risk, 3–9 |
Abnormal renal and/or liver function | 1 point each | ||
Stroke | 1 | ||
Bleeding history | 1 | ||
Labile INR | 1 | ||
Elderly (>65 y) | 1 | ||
Drugs (antiplatelets/NSAIDS)/concomitant/≥8 units alcohol per week) | 1 point each | ||
HEMORR2HAGES | Hepatic or renal disease | 1 | Low risk, 0–1
Intermediate risk, 2–3
High risk, 4–12 |
Ethanol abuse | 1 | ||
Malignancy | 1 | ||
Older (>75 y) | 1 | ||
Reduced platelet count | 1 | ||
Re‑bleeding risk | 2 | ||
Hypertension (uncontrolled) | 1 | ||
Anemia | 1 | ||
Genetic CYP2C9 polymorphisms | 1 | ||
Excessive fall risk | 1 | ||
Stroke/TIA history | 1 | ||
ATRIA | Anemia | 3 | Low risk, 0–3
Intermediate risk, 4
High risk, 5–10 |
Severe CKD | 3 | ||
Age ≥75 y | 2 | ||
Previous bleeding | 1 | ||
Hypertension | 1 | ||
ORBIT‑AF | Age (≥75 y) | 1 | Low risk, 0–2
Medium, risk 3
High risk ≥4 |
Reduced hemoglobin (<13 g/dl in men and <12 g/dl in women) | 2 | ||
Hematocrit (<40% in men and <36% in women) or history of anemia | 2 | ||
Bleeding history | 2 | ||
Insufficient kidney function (eGFR <60 ml/min/1.73 m2) | 1 | ||
Treatment with an antiplatelet agent | 1 | ||
ABC‑bleeding score | Age | Digitally calculated | Low risk <1% per year
Moderate risk, 1%–2% per year
High risk >2% per year |
Biomarkers (growth differentiation factor‑15, high‑sensitivity cardiac troponin T, hemoglobin/hematocrit) | |||
History of previous bleeding | |||
The latest AF guidelines issued by the European Society of Cardiology in 2016 were focused on modifiable risk factors and their elimination, if possible, including the use of antiplatelet agents, alcohol abuse, unstable anticoagulation with a VKA, and uncontrolled hypertension (to reduce the risk of ICB).7 However, nonmodifiable bleeding risk factors such as prior major bleeding or stroke, cancer, or advanced age should not be ignored. Whereas modifiable bleeding risk factors should be identified and managed, the important interaction between these and nonmodifiable bleeding risk factors should be acknowledged, and such high‑risk patients should be scheduled for an earlier and more frequent clinical follow‑up after oral anticoagulant therapy has been initiated. Indeed, a formal bleeding risk assessment using the HAS‑BLED score has been shown to be superior to the less well‑structured approach of addressing modifiable bleeding risk factors only.37-39
Potential new biomarkers in bleeding prediction
Most risk prediction models for bleeding in patients with AF, including HAS‑BLED, ATRIA (Anticoagulation and Risk Factors in Atrial Fibrillation), and ORBIT‑AF (Outcomes Registry for Better Informed Treatment of Atrial Fibrillation) score, do not incorporate biomarkers, although they may improve discrimination of traditional risk scores. In the ARISTOTLE (Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation) trial comparing apixaban with warfarin, blood biomarkers, namely high‑sensitivity cardiac troponin T, growth differentiation factor 15, and hemoglobinor hematocrit showed stronger association with bleeding than most of clinical parameters.40 The ABC‑bleeding score including those 3 biomarkers was validated in the population of the RE‑LY trial and performed better than the HAS‑BLED and ORBIT scores.41 However, these biomarkers are also nonspecifically associated with other cardiovascular outcomes (eg, stroke, death, heart failure)42 and some are not readily available in routine clinical practice.
Other biomarkers reflecting cardiovascular physiology, coagulation and fibrinolysis, are promising candidates for the development of new bleeding risk scores in AF.
We tested characteristics of plasma fibrin clot structure as potential new biomarkers which might help predict bleeding in patients with AF, given evidence indicating that fibrin clots composed of thinner fibers, which are more compact and less permeable, are less susceptible to fibrinolysis.43 Recently, dense fibrin fiber networks, characterized by low plasma clot permeability, have been described as an independent predictor of both thromboembolic events and major bleedings in patients with AF on VKA.44 We reported that patients with lower clot permeability had an increased risk of ischemic stroke or transient ischemic attack (TIA) (hazard ratio [HR], 6.55; 95% CI, 2.17–19.82) and major bleeds (HR, 10.65; 95% CI, 3.52–32.22), while patients with high permeability had elevated risk of minor bleeding compared with those with low fibrin clot permeability (11.63% per year vs 3.55% per year).45 Hypofibrinolysis, as reflected by prolonged clot lysis time, resulted in an 8‑fold increase in stroke or TIA rate in AF patients on a VKA (8.67% per year vs 1.1% per year).46 It was also observed that in patients with AF on rivaroxaban, lower plasma clot permeability, determined as 24 to 30 hours since the intake of rivaroxaban, predicted ischemic cerebrovascular events (HR, 6.64; 95% CI, 2.2–20.1) and major bleedings (HR 7.38; 95% CI, 2.58–21.10), but not deaths, during follow‑up.47,48 Minor persistent bleeding was associated with increased clot permeability in patients with AF on rivaroxaban.47 Recently, an association between higher ORBIT bleeding risk score along with enhanced fibrinolysis and looser clot structure in AF has been reported.33 Despite still poorly understood mechanisms underlying the above observations, it might be speculated, based on experimental work, that denser clot meshwork within thrombi in vessels impair wound healing and adversely affect cell adhesion, migration, proliferation, which might enhance bleeding in particular from the GI tract.49 It remains to be established whether assessing abnormalities in fibrin network structure in AF may be helpful in predicting bleeding events during treatment with VKA and NOAC.
Specific atrial fibrillation patient populations at risk of bleeding on anticoagulation
Advanced age
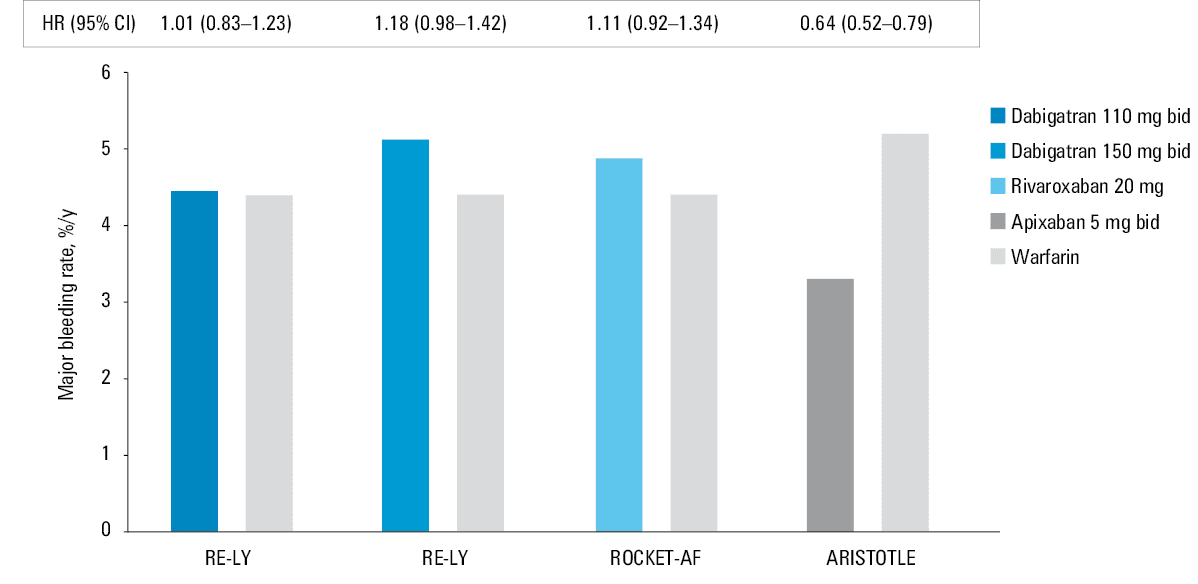
Older patients have a higher risk of bleeding; however, in the age group above 75 years, reduced ICB and increased GI bleeding on NOACs as compared with VKA share the same pattern as that observed in younger patients with AF.9 In phase 3 AF trials, there were some differences in the bleeding risk in patients aged 75 years or older depending on the specific anticoagulants (Figure 2). Assessment of NOACs in elderly patients with AF showed increased rates of extracranial major bleeding in those receiving both doses of dabigatran,50 and similar rates of bleeding regardless of age were reported in RCTs with apixaban, edoxaban, or rivaroxaban.51-53 Compared with warfarin, only apixaban was associated with a lower risk of major bleeding in patients above 75 years.53,54
Low body mass
The risk of all‑cause death, stroke and SE, and major bleeding is higher in anticoagulated patients with lower weight compared with those with normal weight.55 Low body weight may increase exposure to any NOAC and as such increases the risk of bleeding.56 Body weight of 60 kg or less is a dose‑reduction criterion for apixaban.57 In the largest study evaluating NOACs in relation to body weight in patients with AF, apixaban was at least as efficacious as warfarin but safer across the range of weight, with the greatest reduction in the risk of bleeding and hemorrhagic stroke in the group with body weight of 60 kg or less.55 In patients with very low body weight (<50 kg), dabigatran’s efficacy and safety were similar to those observed in the remainder of the study cohort.58 However, observational studies suggested that low body mass index (<23.9 kg/m2) may predict bleeding in patients on dabigatran.59 Of note, frequently coexisting renal insufficiency may make dabigatran a less preferable option for the underweight older patients with AF. Patients with low body weight on oral anticoagulation should be monitored for bleeding risk.
Chronic kidney disease
Patients with AF and chronic kidney disease (CKD) have an increased morbidity and mortality due to their excessive risk for both thromboembolic and severe bleeding events, and risk stratification and treatment of patients with AF and CKD may be challenging.60 All NOACs are eliminated by the kidneys, albeit to a different extent with the maximum value for dabigatran (80%), whereas 50%, 35%, and 27% of edoxaban, rivaroxaban, and apixaban, respectively, are cleared via the kidneys in unchanged form. In all patients on NOACs, renal function needs to be monitored at least yearly. Importantly, intercurrent acute illness (eg, infections, acute heart failure) may transiently affect renal function. Of note, renal function may be overestimated in underweight patients due to their reduced muscle mass (especially when calculated with the Modification of Diet in Renal Disease formula). Compared with warfarin, all 4 NOACs showed consistent efficacy and safety in patients with mild to moderate CKD compared with non‑CKD patients in the respective subgroup analyses of pivotal NOAC trials.40,61-63 The ARISTOTLE trial data analysis suggests that the bleeding benefit with apixaban compared with warfarin becomes more prominent at lower creatinine clearance (CrCl) values, while the stroke reduction benefit is maintained.40,60 In contrast, the bleeding benefit of dabigatran at a dose of 110 mg twice a day over warfarin was not observed in patients with CrCl of less than 50 ml/min while a similar stroke risk reduction compared with VKA was maintained.62
All available trials on NOACs essentially excluded patients with a CrCl of less than 30 ml/min (except for a few patients on apixaban with CrCl 25–30 ml/min in the ARISTOTLE trial). Rivaroxaban, apixaban, and edoxaban (but not dabigatran) are approved in Europe for the use in patients with severe CKD (Stage 4, ie, a CrCl of 15–29 ml/min), with the reduced dose regimen. In Europe, NOACs should not be prescribed to patients with AF and severe renal dysfunction (CrCl <15 ml/min) as well as to patients on dialysis, whereas in the United States, apixaban was approved for hemodialyzed patients in 2014. Since VKA use leads to a high risk of bleeding in this subset of patients, the decision to use a VKA in such patients is challenging and should be based on the individual patient’s risk of stroke, anticipated net benefit, and patient’s preferences.60
Regarding patients with AF after kidney transplantation, high‑quality evidence is lacking, but NOACs might be used with the dosing regimen adjusted to the estimated renal function, and consideration of possible drug–drug interactions between NOACs and immunosuppressive agents.64
Liver disease
Patients with active liver disease, including cirrhosis, or those with persistent (2 measurments at least 7 days apart) elevation of the liver enzymes or bilirubin (eg, alanine transaminase or aspartate transaminase ≥2–3 times the upper limit of normal or total bilirubin ≥1.5 times the upper limit of normal) were excluded from the landmark NOAC trials in AF.13,14,18,58 NOACs are contraindicated in patients with hepatic disease associated with coagulopathy and clinically relevant bleeding risk including class C cirrhosis according to the Child–Pugh classification, while rivaroxaban should not be used even in patients with AF and Child–Pugh class B cirrhosis due to a more than a 2‑fold increase in drug exposure in these individuals.65 Dabigatran, apixaban, and edoxaban may be used with caution in patients with Child–Pugh class B cirrhosis. A reduced‑dose NOAC should be considered in patients with liver disease at high bleeding risk, and close surveillance is advised in this subset. Lee et al,66 in a registry‑based study in patients with liver cirrhosis treated predominantly with low‑dose dabigatran and rivaroxaban, demonstrated the risk of stroke/SE and ICB comparable with warfarin and a reduced risk of major bleeding including GI bleeding. The advantage of NOACs over warfarin in the bleeding risk reduction was observed in the groups with nonalcoholic and nonadvanced cirrhosis. In patients with advanced cirrhosis who presented with any complications such as ascites, encephalopathy, spontaneous bacterial peritonitis, or prior bleeding from esophageal varices, this benefit from NOACs was diminished, presumably due to reduced drug metabolism and impaired hepatobiliary excretion.59
Of note, hepatotoxicity has been observed in less than 1% of patients with AF in the NOAC trials at a similar rate to the warfarin arms.67 Usually, drug withdrawal normalized liver function markers within a few days. Search for underlying liver pathologies and hepatotoxic drugs, for example, amiodarone, should be performed.
Prior serious bleeding
In most bleedings due to secondary (eg, bleeding post‑trauma) or reversible causes (eg, GI bleed due to colon polyps or peptic ulcer), anticoagulation can be resumed once the cause of the bleed is eliminated. Re‑initiation of anticoagulation should be considered after 4 to 7 days after a GI bleed if benefits outweigh potential risks of re‑bleeding.68,69 Factors that need to be taken into consideration before preinitiation or withholding of anticoagulation include identification of the bleeding site, presence of reversible/treatable cause of bleeding and angiodysplasia in the GI tract, older age, chronic alcohol abuse, and need for antiplatelet therapy. Results from observational studies on patients after GI bleeding suggest benefits from resuming anticoagulation without an increase in recurrent GI bleeding in the majority of patients with AF.70
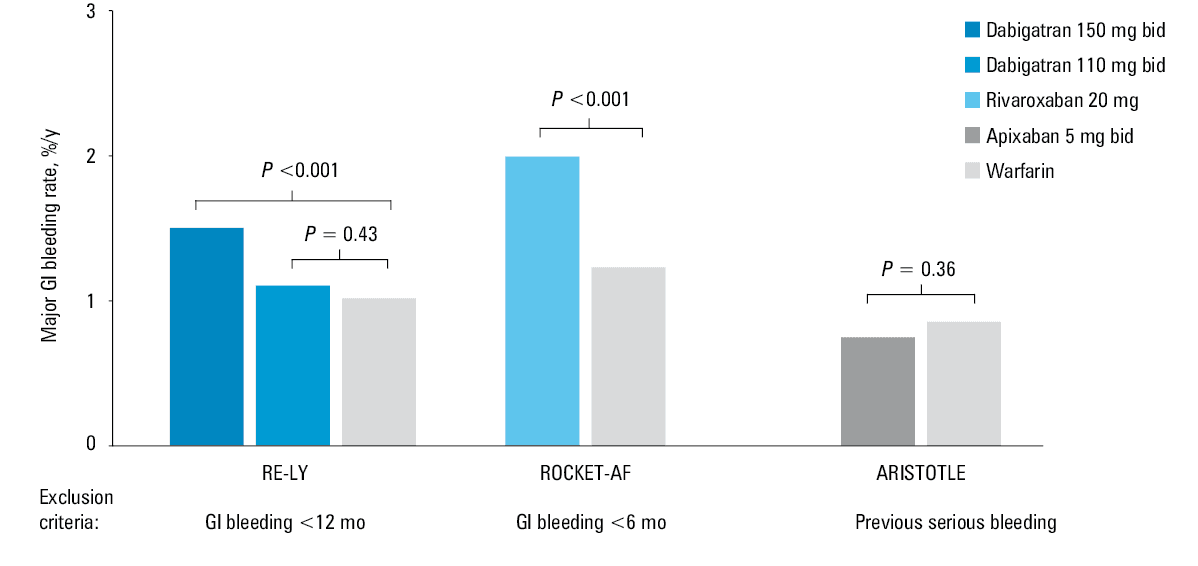
In patients with AF at a high‑risk of GI bleeding, the 2016 European Society of Cardiology guidelines recommend using VKAs or NOACs other than dabigatran at a dose of 150 mg bid, rivaroxaban, 20 mg once daily, and edoxaban, 60 mg once daily (class IIa, level of evidence B). The elimination of modifiable bleeding risk factors, in particular alcohol abuse and cyklooxygenase‑1 inhibitors, is of key importance to minimize bleeding risk on anticoagulation. Importantly, the landmark AF RCTs indicate that, compared with warfarin, the risk of GI bleeds is not increased for dabigatran 110 mg bid and apixaban 5 mg bid7 (Figure 3).
Co‑therapy with protein pump inhibitors is associated with 25% to 51% less hospitalizations due to GI bleeding during VKAs and NOACs use, with the most pronounced reduction observed for dabigatran, as the result of reduced direct mucosal toxicity of the drug and decreased dabigatran bioavailability71 (Figure 4). Approximately 1 in 12 major bleedings in patients receiving warfarin or dabigatran is caused by an underlying cancer of the GI tract, most commonly colorectal cancer. Cancer‑related bleedings manifest sooner and are more frequently chronic than those of a nonmalignant or unidentified source. There was no difference observed in the short‑term outcome between dabigatran- and warfarin‑related bleedings; however, the majority of patients required blood transfusions and prolonged hospital stay.71 Further prospective studies are required to determine if GI cancer screening before and after initiation of anticoagulation, in particular the most common colorectal cancer, may allow earlier cancer detection and treatment; however, baseline screening in high‑risk populations should be considered. Figure 4. The incidence of hospitalizations for upper gastrointestinal (GI) bleeding in relation to oral anticoagulants and proton‑pump inhibitor (PPI) cotherapy (based on Ray et al71)Abbreviations: IRR, incidence rate ratio; RD, risk difference per 10000 person‑years; others, see Figure 1A history of a spontaneous ICB is a contraindication for anticoagulation with VKAs and NOACs based on the manufacturer’s recommendations, unless the cause of the bleeding (like uncontrolled hypertension, aneurysm or arteriovenous malformation, or triple antithrombotic therapy) has been reversed.7,72 Reasons for not resuming or initiating anticoagulation in patients with ICB and AF should be assessed on an individual basis.73 Patients with (probable) cerebral amyloid angiopathy have a very high risk of recurrent ICB and should not be anticoagulated.74 Adequate blood pressure control is of paramount importance in all patients after ICB.73 Left atrial appendage occlusion may be considered in some patients with AF after ICB as well as after recurrent intractable or untreatable major bleeding, although evidence on the role of left atrial appendage occlusion in such patients is lacking.7,75However, antiplatelet treatment for at least 1 month post left atrial appendage occlusion is associated with increased bleeding risk in such patients, which should be taken into account especially in elderly patients with AF.ThrombocytopeniaIt is estimated that up to 3% of patients with AF have thrombocytopenia, defined as a platelet count below 100000/µl.76 Although thrombocytopenia does not protect against thromboembolic events, patients with AF with platelet count below 90000 to 100000/µl were excluded from the landmark phase 3 NOAC trials.51-53The current guidelines for the management of patients with AF do not provide any recommendations for the use of NOACs in thrombocytopenic patients.68,69In a retrospective study, the use of VKAs in patients with moderate thrombocytopenia of 50000 to 100000/µl (mean platelet count, 87900/µl) who had AF or VTE was associated with a 3‑fold higher incidence of minor bleeding (5.55 vs 1.84 per 100 patient‑years) and a tendency toward a higher risk of major bleeding. All the recorded bleeding complications occurred at INRs above 2.5, which suggests using narrower INR targets and lower intensity oral anticoagulation.77 Sadowska et al76 demonstrated the acceptable safety and effectiveness of anticoagulation with NOAC at reduced doses in a cohort of patients with AF with moderate thrombocytopenia (mean platelet count, 78000/µl). The risk of bleeding was unaffected by the type of NOAC (rivaroxaban, 15 mg once daily; dabigatran, 110 mg bid; or apixaban, 2.5 mg bid), and was predicted only by age. Despite the dose reduction of a NOAC, similar rates of stroke or TIA and death were observed in thrombocytopenic and normocytopenic patients. Of note, several cases of NOAC‑induced thrombocytopenia have been reported in the literature, which supports platelet count monitoring during treatment.78In patients with severe thrombocytopenia (<50000/µl) and AF, the anticoagulation should be individualized and closely monitored given the lack of evidence from trials.Cancer patientsAtrial fibrillation is present in approximately 5% of patients with cancer at the time of diagnosis or within the first months of treatment.79 Based on the current guidelines, about 80% of patients with AF and cancer had indications for chronic anticoagulation.80 Of note, cancer is associated with an increased risk of bleeding related to thrombocytopenia, metastases, kidney and liver damage, vessel damage caused by a tumor infiltrating its wall, invasive procedures, and radiation therapy.69Regarding patients with cancer and AF, most data are from observational studies.81 Randomized studies of patients with cancer and VTE, including the Hokusai VTE Cancer trial with edoxaban and SELECT‑D (Anticoagulation Therapy in Selected Cancer Patients at Risk of Recurrence of Venous Thromboembolism) trial with rivaroxaban, showed that NOACs use compared with dalteparin was associated with reduction in the recurrence rate of VTE and increased risk of major bleeding, mainly GI bleeding. The highest bleeding risk was observed in patients with esophageal, gastroesophageal, and urologic cancer.82,83Shah et al,84 in a registry‑based study in a population of patients with AF and cancer, reported lower or similar rates of bleeding and stroke, and a lower rate of VTE in NOAC users as compared with VKA users. Although limited by the sample size, the lowest rates of VTE and severe bleeding were observed for apixaban. Data from registries suggested a higher number of hemorrhagic complications in patients with cancer and AF with concomitant metastatic disease, advanced CKD, recent bleeding (<30 days), and longer immobility.85The 2019 ISTH guidelines regarding the use of NOACs in patients with AF and cancer receiving chemotherapy recommend individualized anticoagulation, based on the risk of stroke, bleeding, and patient preferences. NOACs should be considered in patients with clinically relevant interactions between VKAs and anticancer medications that are not expected with NOACs, or in those unable to comply with INR monitoring. The use of NOACs over VKAs or heparins is suggested in patients on chemotherapy with newly diagnosed AF, with the exception of patients with luminal GI cancer and an intact primary tumor or active GI mucosal abnormalities.86 In a recent study in patients with colorectal cancer after surgery and first‑line chemotherapy treated with a NOAC, mainly rivaroxaban in a dose of 20 mg daily, the rate of TIA and stroke as well as major bleeding was relatively low, 4.0% and 1.9%, respectively. A reduced dose of a NOAC was associated with higher risk of thromboembolic events.87 Real‑world data on the effectiveness and safety of NOACs in oncological patients suggest a clear benefit, especially in patients with favorable prognosis; however, the safety in specific subgroups of patients with cancer remains to be clarified.88,89Reversal agentsThe use of specific and nonspecific reversal agents in patients with AF on NOACs should be restricted to life‑threatening situations, predominantly ICB or posttraumatic bleeding.90Idarucizumab is a humanized monoclonal antibody fragment which is a specific reversal agent for dabigatran. It binds with 350 times higher affinity than thrombin to free and thrombin‑bound dabigatran within minutes. This reaction is irreversible.90Idarucizumab was approved in Europe in November 2015. It has become the standard of care for the reversal of dabigatran when it is available. The RE‑VERSE AD (Reversal Effects of Idarucizumab on Active Dabigatran) study assessed the safety and efficacy of 5 g idarucizumab (administered as 2 rapid 2.5 g intravenous boluses) in dabigatran‑treated patients who presented with uncontrolled or life‑threatening bleeding (group A) or nonbleeding patients who required emergent surgery or intervention (group B). The primary outcome of the RE‑VERSE AD study was maximum percentage reversal of the anticoagulant effect of dabigatran. The RE‑VERSE AD study, published as an interim analysis of the first 90 patients in 201591 and then a final analysis of 503 patients in 2017,92 showed the utility of idarucizumab in the 2 groups of patients. Now, idarucizumab is the best therapeutic option for patients with AF on dabigatran who experience life‑threatening bleeding.Andexanet alfa, which binds with high affinity to direct factor Xa inhibitors and also low‑molecular‑weight heparins and fondaparinux,93 is a modified human recombinant factor Xa decoy protein that lacks catalytical activity following replacement of an active‑site serine with alanine and with removal of the membrane‑binding domain, which precludes this protein to participate in the formation of the prothrombinase complex.15,92 Because of its pharmacodynamic half‑life of 1 hour, andexanet was administered as a bolus followed by an infusion, which leads to the normalization of anti–factor Xa activity within 2 hours.The results of 2 RCTs (Andexanet Alfa, a Novel Antidote to the Anticoagulation Effects of FXA Inhibitors trials [ANNEXA]) performed in healthy volunteers aged 50 to 75 years who received apixaban (ANNEXA‑A) and rivaroxaban (ANNEXA‑R)93 demonstrated the efficacy and safety of andexanet alfa. The phase 3b to 4 ANNEXA‑4 study confirmed the efficacy and safety of andexanet alfa in patients treated with factor Xa inhibitors with acute major bleeding.In May 2018, andexanet alfa, which is a specific reversal agent for oral factor Xa inhibitors, was approved in the United States, and in 2019 in Europe, but currently it is unavailable in many countries. For this reason, the available Xa inhibitor reversal strategies rely on nonspecific strategies of unknown effectiveness, in particular prothrombin complex concentrates (PCCs). Prothrombin complex concentrates are plasma‑derived products that contain 3 (factors II, IX, and X) or 4 (addition of factor VII) clotting factors in addition to variable amounts of heparin and natural coagulation inhibitors, protein C and protein S, which are used among others to reverse anticoagulant effects of VKAs in patients with severe bleeding. Activated PCC (also known as factor VIII inhibitor bypassing activity) contains mostly activated factor VII along with mainly nonactivated factors II, IX, and X. A dose of 50 U/kg of PCC or activated PCC is recommend in patients treated with rivaroxaban or apixaban if life‑threatening bleeding occurs.16,19A prospective multicenter observational study showed that in the real world,94 reversal strategies in bleeding patients on rivaroxaban or apixaban differ largely. A Swedish case series of 84 bleeding patients (75% with AF) who required reversal of factor Xa inhibition after 9 to 16 hours since the last dose of the anticoagulant showed that in most cases (70% ICB and 16% GI bleeds), PCC at a dose of 2000 units was used in patients with body weight of 65 kg or more, while 1500 units were administered in patients weighted below 65 kg.95 No hemostatic effect of PCC was observed in 30.9% of patients, largely in those with ICB. Of note, 15 patients died, including 13 patients following ICB (30‑day mortality rate, 32%), whereas 2 patients had fatal ischemic stroke at 5 and 15 days after the index bleeding.96Analysis of 460 bleeds observed in patients on NOACs showed that almost 20% of those patients received vitamin K, which is useless in such clinical situations.94 It has absolutely no possibility of any effect, but was given probably because many of these patients had a prolonged INR due to rivaroxaban.97Tranexamic acid, an antifibrinolytic agent effective in trauma or postpartum hemorrhages, acts as a lysine analog that impairs plasminogen activation on fibrin. In patients on NOACs, its efficacy is uncertain; however, it might be used.Fresh frozen plasma is ineffective in patients bleeding on NOACs but was used in about 10% of patients reported by Xu Y et al.94 Fresh frozen plasma may be used as a plasma volume expander in patients following transfusions; however, its shortcomings are numerous, including risk of transfusion reactions, and acute heart failure.Experts strongly recommend that an institutional policy concerning bleeding management is defined in every hospital. In patients on NOACs, the recommendations, including a protocol containing the availability and indications of specific and nonspecific reversal agents, should be developed by cardiologists, hemostasis experts, intensivists and others, and this policy should be easily accessible for all physicians in a given institution.31,68Patient preferences and knowledge in reducing bleeding riskOptimal treatment strategies for stroke prevention incorporate patient preferences and values, which may differ from those of the physician. Results from a survey suggest that patients with AF who initiate oral anticoagulation are willing to sustain 4 major bleeds to avoid 1 serious stroke.98 About half of the patients, mainly older, with minor or major bleeds on anticoagulation and without history of cerebrovascular events, accept a low number of bleeds (0–3). Our recent findings confirmed that patients with AF fear a major stroke more than bleeding, but they are less willing to accept such adverse events after a serious bleed in the past as well as in the presence of persistent minor bleeding, for example, easy bruising.98 From a practical point of view, it is important to remember that only 1 out of 2 patients with AF treated with NOACs or VKAs is aware that the safest painkiller is paracetamol, and 1 out of 4 patients knows what to do when an anticoagulant dose is missed. Among patients with AF, women, patients with diabetes, prosthetic heart valve, and minor bleedings were found to be better informed about those issues.99 Better education about the disease and anticoagulation is likely to improve compliance and therapy outcomes in patients with AF,100 and activities aiming at improving knowledge should be strongly supported in everyday practice.Monitoring Patients treated with NOACs are likely to be followed less frequently compared with patients receiving VKAs because NOAC plasma levels do not require routine monitoring.The 2018 European Heart Rhythm Association guidelines on the use of NOACs in patients with AF recommend regular follow‑up assessment during NOAC use, particularly in high‑risk groups with older age, renal failure, multiple comorbidities, and frailty.68 At each visit, the following should be evaluated: adherence to treatment, comedications, presence of thromboembolic and bleeding complications as well as other side effects. Particular attention should be directed to minimizing modifiable bleeding risk factors and to assess an optimal NOAC and its correct dosing. In patients on NOACs without renal impairment, CrCl using the Cockcroft–Gault method should be monitored at least yearly. In case of kidney failure, a more frequent evaluation should be performed (recheck interval in months may be calculated from equation CrCl/10). Hemoglobin concentration and liver function should be measured at least once every 6 months in patients aged 75 years or older (especially if on dabigatran) or with frailty, and yearly in other patients.Limited data support the measurement of plasma levels of NOACs in emergencies, before elective procedures, and during long‑term exposure. There are several special situations in which the assessment of drug exposure and anticoagulant effect may support clinical decisions. They include: 1) thrombolytic therapy in stroke, 2) surgery or invasive procedure, 3) a need for immediate reversal of anticoagulation, 4) extreme body weight, 5) substantial drug–drug interactions (eg, after transplantation, anti‑HIV treatment), 6) suspected noncompliance or overdosage in case of thrombosis or hemorrhage, respectively.97ConclusionsOverall, NOACs were comparable or superior to VKAs in most patients with AF as shown in RCTs and observational studies. Individualization of anticoagulant therapy based on benefit and safety profiles as well as patient characteristics should be considered in particular in patients with AF at elevated risk of bleeding, such as the elderly patients with several comorbidities and those with cancer (Table 2). Given a high risk of stroke in most patients with AF as compared with bleeding risk, appropriate dosing regimen should be used and reduced‑dose regimen should be restricted to the recommended settings. Modifiable bleeding risk factors such as use of nonsteroidal anti‑inflammatory drugs available over the counter should be eliminated whenever feasible. Table 2. Non–vitamin K antagonist oral anticoagulants and approved/studied daily doses in stroke prevention in atrial fibrillation (based on Diener et al54 and Steffel et al)68NOACStandard doseDose reductionApixaban2 × 5 mg2 × 2.5 mg if 2 out of 3:• Weight ≤60 kg• Age ≥80 y• Serum creatinine ≥133 μmol/l (1.5 mg/dl) (or if CrCl, 15–29 ml/min)Dabigatran2 × 150 mgNo prespecified dose‑reduction criteriaBased on SmPC, 2 × 110 mg if: • Age ≥80 y • Concomitant verapamil • Increased risk of gastrointestinal bleedingEdoxaban1 × 60 mg1 × 30 mg if: • Weight ≤60 kg • CrCl ≤50 ml/min • Concomitant therapy with strong P‑Gp inhibitorRivaroxaban1 × 20 mg1 × 15 mg if CrCl ≤50 ml/minBased on clinical and pharmacokinetic data, dose adjustment or NOAC change should be considered if: age ≥75 years, cancer, concomitant antiplatelet drugs or significant drug–drug interactions, frailty/fall risk, chronic kidney disease stage 4, hepatic injury, history of bleeding or predisposition, recent surgery on critical organ and thrombocytopenia.Abbreviations: CrCl, creatinine clearance; NOAC, non–vitamin K antagonist oral anticoagulant; SmPC, summary of product characteristics
- Camm AJ, Lip GY, De Caterina R, et al. 2012 focused update of the ESC Guidelines for the management of atrial fibrillation: an update of the 2010 ESC Guidelines for the management of atrial fibrillation. Developed with the special contribution of the European Heart Rhythm Association. Europace. 2012; 14: 1385‑1413.
- Banerjee A, Lane DA, Torp‑Pedersen C, Lip GY. Net clinical benefit of new oral anticoagulants (dabigatran, rivaroxaban, apixaban) versus no treatment in a “real world” atrial fibrillation population: a modelling analysis based on a nationwide cohort study. Thromb Haemost. 2012; 107: 584‑589. | Crossref
- Potpara TS, Mujovic N, Lip GY. Meeting the unmet needs to improve management and outcomes of patients with atrial fibrillation: Fitting global solutions to local settings. Pol Arch Intern Med. 2019; 129: 574‑576. | Crossref
- Devereaux PJ, Anderson DR, Gardner MJ, et al. Differences between perspectives of physicians and patients on anticoagulation in patients with atrial fibrillation: observational study. BMJ. 2001; 323: 1218‑1221. | Crossref
- Camm AJ, Fox KAA, Peterson E. Challenges in comparing the non‑Vitamin K antagonist oral anticoagulants for atrial fibrillation‑related stroke prevention. Europace. 2018; 20: 1‑11. | Crossref
ARTICLE INFORMATION