Adult secondary hemophagocytic lymphohistiocytosis with cerebral and meningeal symptoms early after allogeneic hematopoietic stem cell transplantation



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Adult secondary hemophagocytic lymphohistiocytosis with cerebral and meningeal symptoms early after allogeneic hematopoietic stem cell transplantation
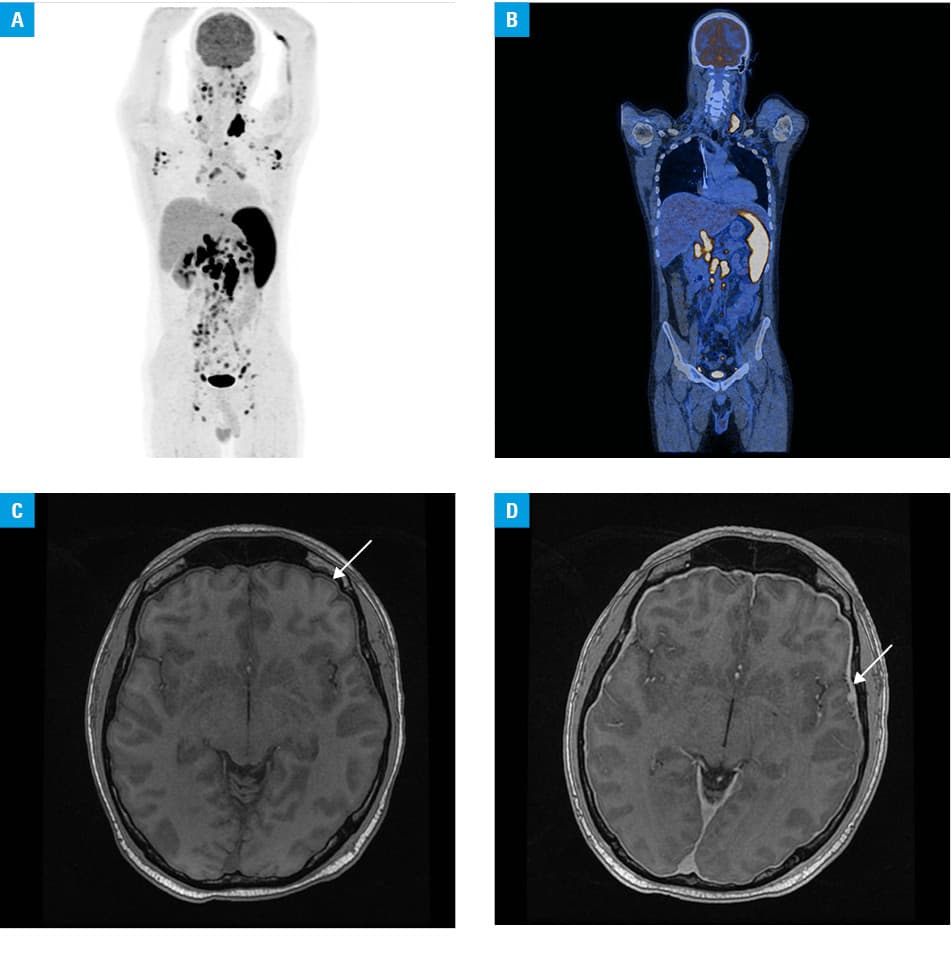
A 28‑year‑old man with Ph‑negative acute lymphoblastic leukemia was readmitted to the Bone Marrow Transplant Unit on day 42 after matched unrelated donor allogeneic hematopoietic stem cell transplantation (allo‑HSCT), presenting with fever, general malaise, tonsillitis, lymphadenopathy, and splenomegaly. The pretransplant patient/donor cytomegalovirus (CMV) status was positive/negative, and the Epstein–Barr virus (EBV) status was positive/positive. On admission, a high blood EBV load (1.2 × 105 copies/ml) was detected. Due to progressing organomegaly and elevation of lactate dehydrogenase levels after standard treatment with rituximab (375 mg/m2 intravenously [IV]), 18F‑fluorodeoxyglucose positron emission tomography–computed tomography was performed. It revealed abnormally increased metabolic activity in multiple enlarged lymph nodes and the spleen (Figure 1A and 1B). Because of pancytopenia progression, additional blood tests were performed. Prominent hyperferritinemia (ferritin levels, 74000 µg/l; reference range, 13–400 µg/l) with hypertriglyceridemia (triglyceride levels, 3.73 mmol/l; reference range, <2.26 mmol/l) were noted. Peripheral blood lymphocyte immunophenotyping showed a sparse natural killer (NK) cell population. A tentative diagnosis of posttransplant lymphoproliferative disorder (PTLD), accompanied by hemophagocytic lymphohistiocytosis (HLH), was made.1,2 Despite the administration of the second and third rituximab dose and a reduction of cyclosporine A (CsA) dosage, the patient developed neurologic symptoms, particularly in the range of cortical activities: deterioration in verbal contact, memory impairment, and disorientation followed by coma. Brain magnetic resonance imaging suggested meningitis (Figure 1C and 1D). Cerebrospinal fluid analysis revealed high protein levels (283 mg/dl; reference range, 20–40 mg/dl), pleocytosis (white blood cell count, 70/µl), and high EBV load (6.2 × 103 copies/ml). Subsequently, immunosuppression was modified: dexamethasone was introduced (8 mg 3 times daily) with complete CsA withdrawal. Due to the severity of the neurologic status, antiviral acyclovir was switched to foscarnet, and 3 doses of IV etoposide (100 mg) as well as 2 doses of intrathecal methotrexate (15 mg) were administered, in parallel with weekly rituximab (up to 5 infusions). The patient’s general condition improved. Finally, the EBV clearance was achieved. A dose of systemic dexamethasone was gradually tapered, simultaneously with restarting CsA. At present, 5 years after the transplant, the patient is alive and remains in complete remission.
The EBV is a highly immunogenic γ-herpesvirus. Severely immunosuppressed patients develop B‑cell proliferation and a diminished EBV‑specific cytotoxic T‑cell population.3 B‑cell PTLD associated with EBV is a life‑threatening complication after allo‑HSCT, resulting from an outgrowth of infected donor‑origin B cells.3 In patients after allo‑HSCT, EBV is the second most common cause of viral encephalitis, after human herpesvirus 6.4 Hemophagocytic lymphohistiocytosis, characterized by molecular abnormalities and clinical or laboratory findings such as fever, splenomegaly, cytopenia, reduced NK cell activity, hypofibrinogenemia, hemophagocytosis, and increased levels of soluble CD25 protein, ferritin, and triglycerides, has become more widely recognized in adults, predominately as a secondary disease.5 The treatment strategy in EBV‑driven HLH depends on the patient’s condition, from short‑term corticosteroids with or without immunoglobulins in less severe disease to intensive treatment with early etoposide administration in rapidly deteriorating patients.5 There is no established standard of care in patients fulfilling the HLH‑2004 diagnostic criteria for HLH after allo‑HSCT. In our patient, based on the high EBV load and imaging, probable PTLD was diagnosed, complicated by HLH. The differential diagnosis should include EBV meningoencephalitis and advanced HLH with central nervous system involvement. In our case, focusing on HLH as a major life‑threatening event, the adoption of HLH‑2004 therapeutic modalities provided an excellent clinical outcome in a rituximab‑refractory disease. However, the negative pretransplant EBV immunity status in a donor and coreactivation of viruses may impede treatment.
- Styczyński J, van der Velden W, Fox CP, et al. Management of Epstein‑Barr Virus infections and post‑transplant lymphoproliferative disorders in patients after allogeneic hematopoietic stem cell transplantation: Sixth European Conference on Infections in Leukemia (ECIL‑6) guidelines. Haematologica. 2016; 101: 803‑811. | Crossref
- Bergsten E, Horne A, Aricó M, et al. Confirmed efficacy of etoposide and dexamethasone in HLH treatment: long‑term results of the cooperative HLH‑2004 study. Blood. 2017; 130: 2728‑2738. | Crossref
- Heslop HE. How I treat EBV lymphoproliferation. Blood. 2009; 114: 4002‑4008. | Crossref
- Schmidt‑Hieber M, Schwender J, Heinz WJ, et al. Viral encephalitis after allogeneic stem cell transplantation: a rare complication with distinct characteristics of different causative agents. Haematologica. 2011; 96: 142‑149. | Crossref
- La Rosée, P, Horne, A, Hines M, et al. Recommendations for the management of hemophagocytic lymphohistiocytosis in adults. Blood. 2019; 133: 2465‑2477. | Crossref
ARTICLE INFORMATION