Of horses and zebras: a gastrointestinal infection with Pasteurella canis in a patient with acute myeloid leukemia



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Of horses and zebras: a gastrointestinal infection with Pasteurella canis in a patient with acute myeloid leukemia
A 22‑year‑old woman was diagnosed with acute myeloid leukemia (AML) with t(9;11)(p21;q23) KMT2A/MLLT3 in May 2016. After induction chemotherapy during aplasia, she developed fever, malaise, and psychiatric symptoms, followed by rapidly progressing pneumonia and acute respiratory failure (Figure 1A). As the patient required respiratory support, she was transferred to an intensive care unit. She responded to therapy with broad‑spectrum antibiotics, and her condition improved along with hematologic recovery. Bone marrow biopsy confirmed complete remission.
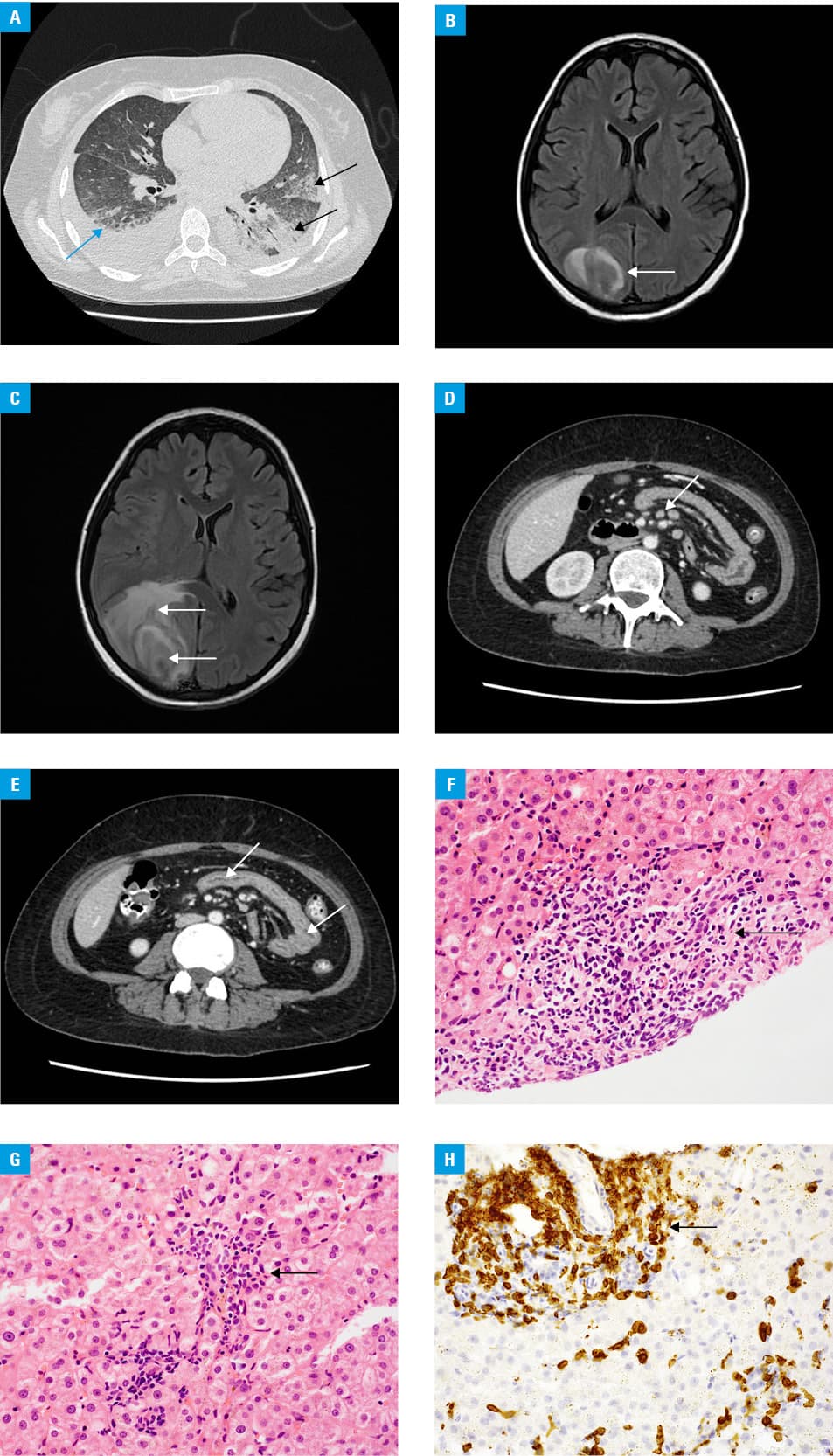
One week after the administration of intrathecal chemotherapy, the patient developed an epileptic state. Brain computed tomography (CT) and magnetic resonance imaging revealed a gradually growing tumor in the right occipital lobe (Figure 1B and 1C). Stereotactic biopsy was inconclusive, and a surgical excision of the tumor was performed. Histopathology revealed brain abscess with significant necrosis. Unfortunately, microbiological examination was not performed.
In September 2016, during neutropenia after consolidation chemotherapy, pneumonia classified as probable pulmonary aspergillosis was diagnosed on the basis of high‑resolution computed tomography (HRCT) of the chest and positive serum galactomannan test results. Broad‑spectrum antimicrobial therapy was started. The patient’s condition improved after hematologic recovery. However, as nonspecific gastrointestinal symptoms persisted, the patient underwent further diagnostic workup. Abdominal CT imaging (Figure 1D and 1E) yielded abnormal findings, which prompted a liver biopsy. It revealed low‑grade liver inflammation, classified as G2, F1/2 according to the Batts–Ludwig system (Figure 1F–1H). Cell culture was positive for penicillin‑susceptible, ciprofloxacin- and cefotaxime‑resistant Pasteurella canis. The patient received oral phenoxymethylpenicillin therapy for 6 months, and in July 2017, she was subjected to allogeneic hematopoietic stem cell transplantation with myeloablative conditioning. During neutropenia, she developed fever and asymmetric erythematous swelling of the left forearm at the site of a scar from a dog bite several years earlier. At the same time, pulmonary infiltrates were found on HRCT of the chest. After broad‑spectrum antimicrobial therapy and hematologic recovery, the symptoms rapidly resolved. The further posttransplant clinical course was uneventful.
Pasteurella is a genus of small, nonmotile, facultatively anerobic Gram‑negative bacteria.1,2 In cats and dogs, it naturally occurs in the flora of the nose and mouth. Most human infections are caused by dog and cat bites.1,3 Based on literature review, this is the first case report of a gastrointestinal infection with P. canis in a patient with AML. There have been several reports of peritonitis caused by a more common pathogen, P. multocida, in patients with diabetes, on dialysis, and with chronic liver disease.1-3 Patients with AML, especially those with neutropenia, are highly predisposed to developing an infection. However, the majority of infections are caused by Enterobacteriaceae and fungi. Empirical antimicrobial strategies have been developed to manage patients with these pathogens.4,5 In our case, blood culture results revealed that the patient experienced extended‑spectrum beta‑lactamase–positive Klebsiella bacteremia and 2 episodes of Candida glabrata fungemia. Furthermore, pulmonary aspergillosis was suspected. However, the unusual course with severe infection episodes complicating every neutropenia period (pneumonia, brain abscess, and gastroenteritis) prompted further diagnostic workup. Imaging techniques followed by liver biopsy with microbiological examination allowed us to diagnose untypical gastrointestinal pasteurellosis. The etiology of brain abscess remains unknown.
- Wilson BA, Ho M. Pasteurella multocida: from zoonosis to cellular microbiology. Clin Microbiol Rev. 2013; 26: 631‑655. | Crossref
- Nollet V, Souply L, Rosolen B, et al. Risk factors for invasive pasteurellosis: a retrospective case study. Eur J Clin Microbiol Infect Dis. 2016; 35: 1975‑1981. | Crossref
- Vesza Z, Boattini M, Pinto M, Marques da Silva P. Pasteurella infections in a tertiary centre – from cellulitis to multiple‑organ failure: retrospective case series. SAGE Open Med Case Rep. 2017; 5: 2050313X17748286. | Crossref
- Averbuch D, Orasch C, Cordonnier C, et al. European guidelines for empirical antibacterial therapy for febrile neutropenic patients in the era of growing resistance: summary of the 2011. 4th European Conference on Infections in Leukemia. Haematologica. 2013; 98: 1826‑1835. | Crossref
- Neofytos D, Lu K, Hatfield‑Seung A, et al. Epidemiology, outcomes, and risk factors of invasive fungal infections in adult patients with acute myelogenous leukemia after induction chemotherapy. Diag Microbiol Infec Dis. 2013; 75: 144‑149. | Crossref
ARTICLE INFORMATION