Pneumomediastinum (PM) and subcutaneous emphysema (SCE) can lead to life‑threatening conditions such as pulmonary embolism, extravascular pressure, and obstructive shock.1 Their high dynamics requires an immediate and accurate diagnosis, which subsequently guarantees proper treatment.2,3 Dental procedures represent a very rare cause of PM and SCE, so patients are often misdiagnosed with allergic reactions to locally administered anesthetic agents.4 We present a case of a patient with PM and SCE as complications of dental extraction.
A 21‑year‑old woman visited a dental clinic for extraction of the right upper third molar. An injection of 1% lidocaine with adrenaline was administered for local anesthesia. The patient’s local and general preparation for dental extraction was good, which was important for clinical, economic, and social reasons.5 During surgery, the patient felt severe central chest pain, exhibited shortness of breath, and developed acute dyspnea. The dentist interrupted the surgical procedure to call an ambulance. The rescuer performed a physical examination, which revealed additional soft‑tissue swelling on the right side of the face and neck. On auscultation, sounds in the chest were symmetric and normal. The patient was transported to the emergency department, where she was diagnosed with an allergic reaction to the local anesthetic agent. She received standard antihistamine drugs. The vital signs normalized; however, the swelling of the cheek remained. The patient felt better and went home.
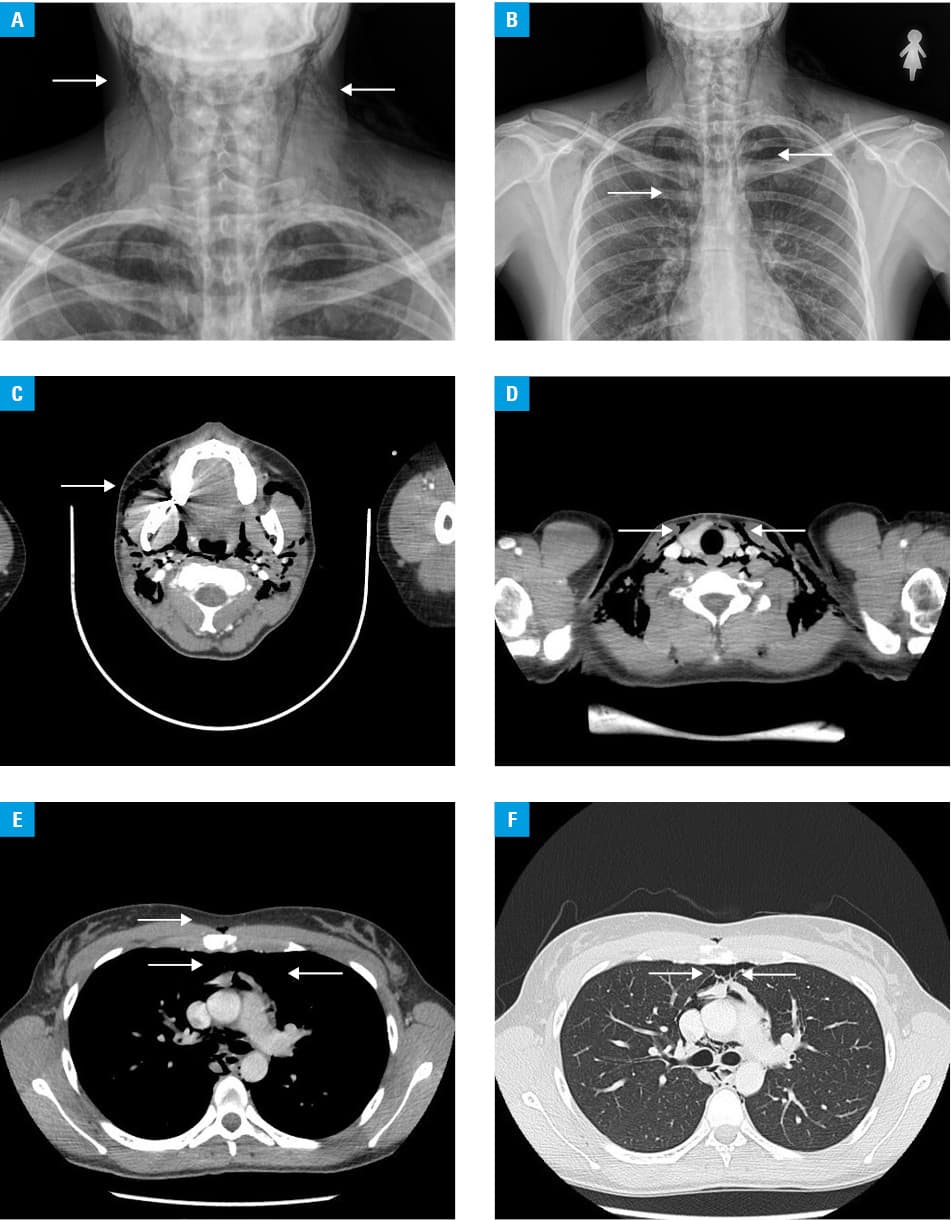
At night, dyspnea persisted and chest pain recurred. The patient visited a night clinic, and she was transported to the nearest hospital. In the emergency room, her vital signs upon arrival were as follows: temperature, 37 °C; blood pressure, 130/80 mm Hg; and heart rate, 92 beats per minute. Extensive SCE with crepitations was found, involving the tissues of the right infraorbital region, right cheek, both sides of the neck, both supraclavicular fossae, and the anterior chest wall. Both SCE and PM were detected on X‑ray of the neck and chest (Figure 1A and 1B). The patient was transported to the tertiary university hospital where computed tomography was performed. It revealed massive mediastinal emphysema that extended from the diaphragm to the upper thoracic aperture, including the paraoesophageal and paratracheal regions, upward into the soft tissues around the neck and right cheek (Figure 1C and 1D) along the anterior surface of the sternum (Figure 1E and 1F). The case was discussed with maxillofacial and thoracic surgeons, who confirmed the diagnosis of PM and SCE. No abnormalities were found on gastro- and bronchoscopy. An otolaryngology consultation did not reveal any changes in the mucosa of the oral cavity or pharynx. The patient was treated conservatively and received fluids intravenously, analgesics, and prophylactic antibiotics. After 5 days of hospitalization, the radiological and physical symptoms subsided, and the patient was discharged.
Our patient’s case highlights dental extraction as one of the potential causes of PM and SCE. The diagnosis may be established with plain anterior chest and neck images. Physicians must be aware of these rare complications of dental procedures to avoid misdiagnosing specific symptoms.
- Pich H, Heller AR. Obstructive shock. Anaesthesist. 2015; 64: 403‑419. | Crossref
- Richards JB, Wilcox SR. Diagnosis and management of shock in the emergency department. Emerg Med Pract. 2014; 16: 1‑22.
- Dentali F, Cei M, Mumoli N, Gianni M. How to predict short- and long‑term mortality in patients with pulmonary embolism? Pol Arch Med Wewn. 2015; 125: 82‑88. | Crossref
- Shackelford D, Casani JA. Diffuse subcutaneous emphysema, pneumomediastinum, and pneumothorax after dental extraction. Ann Emerg Med. 1993; 22: 248‑250. | Crossref
- Lewandowski B, Wojnar J, Brodowski R, et al. Dental extractions in patients with mild hemophilia A and hemophilia B and von Willebrand disease without clotting factor supplementation. Pol Arch Intern Med. 2018; 128: 488‑490. | Crossref
ARTICLE INFORMATION