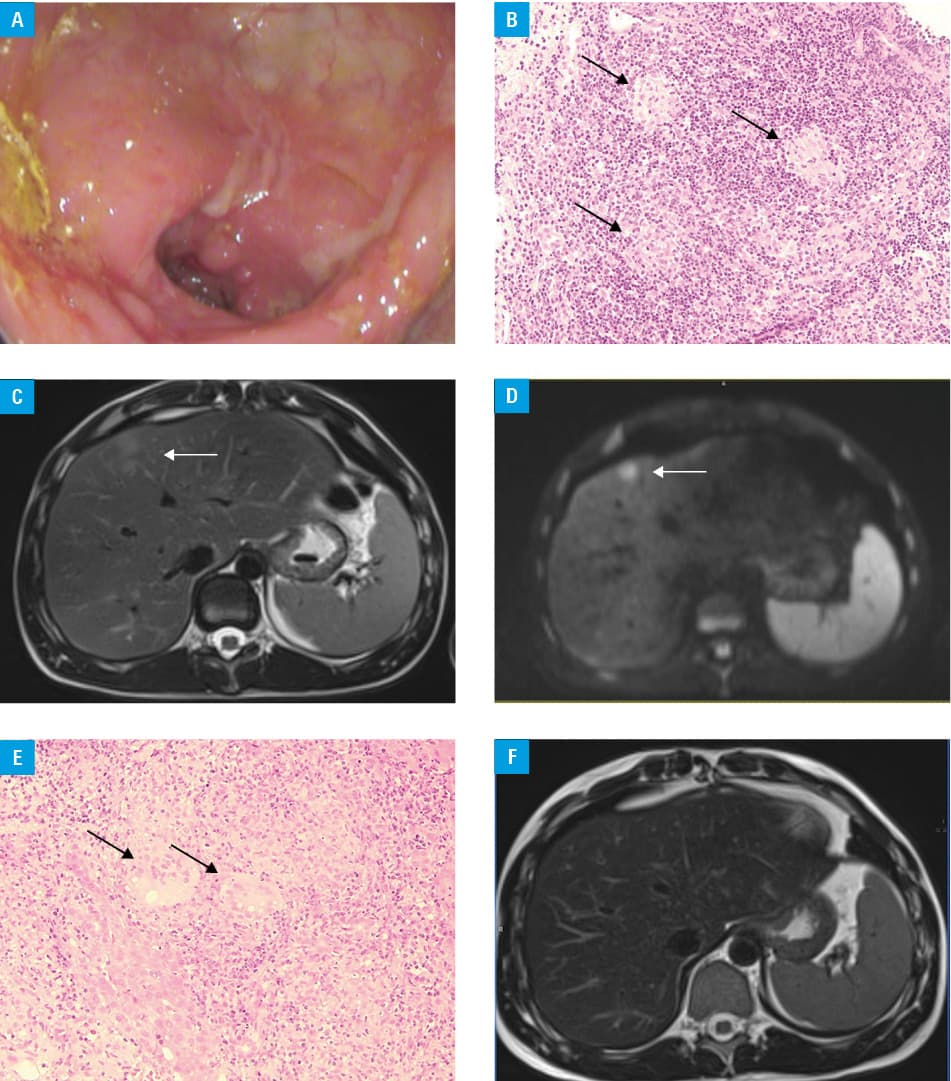
A 22‑year‑old man with Crohn disease diagnosed 5 years earlier was admitted to the hospital due to abdominal pain, diarrhea, fever, and weight loss. His medical history was significant for perianal disease. Previous treatment included 1‑year therapy with infliximab that led to clinical remission. Colonoscopy was performed and revealed stricture in the ascending colon with mucosal edema and ulcerations (Figure 1A). Features of chronic inflammation and noncaseating granulomas were observed in colonic biopsy specimens (Figure 1B). Imaging studies revealed focal liver lesions that raised suspicion of malignancy. Contrast‑enhanced computed tomography showed hypodense liver lesions suggestive of metastases. Magnetic resonance imaging (MRI) was performed, and a T2‑weighted image demonstrated moderately hyperintense nodules (Figure 1C) that showed restricted diffusion in the diffusion‑weighted imaging sequence (Figure 1D). Multiple additional studies were performed to look for the primary neoplastic tumor, but no abnormalities were found. Ultrasound‑guided biopsy of hepatic lesions revealed noncaseating granulomas (Figure 1E). Infectious etiology and autoimmune liver diseases were excluded. The patient was treated with steroids and azathioprine. After 2 months of therapy, he presented no symptoms of Crohn disease. A complete regression of hepatic lesions was observed on follow‑up MRI (Figure 1F).
Crohn disease is characterized by transmural inflammation and granulomas. Deep transmural ulcerations may lead to formation of fistulas that cause significant morbidity and lower quality of life. The occurrence of perianal disease varies between 21% and 23%.1 Small‑bowel fistulas are observed in 10% to 20% of patients.2 Another important group of complications are extraintestinal manifestations that affect up to 35% of patients with Crohn disease.1 They can mimic other conditions, making a precise diagnosis difficult.3 The prevalence of hepatic granulomas as a complication of Crohn disease is unknown. Only a few cases have been reported in the literature.4 Hepatic granulomas can be present in various conditions, the most frequent being sarcoidosis, tuberculosis, primary biliary cholangitis, and drug reactions.5
- Gionchetti P, Dignass A, Danese S, et al. 3rd European evidence‑based consensus on the diagnosis and management of Crohn’s disease 2016: part 2: surgical management and special situations. J Crohns Colitis. 2017; 11: 135‑149. | Crossref
- Iraha A, Koga E, Ohira T, et al. The clover sign of internal fistulas in Crohn disease. Pol Arch Intern Med. 2019; 129: 707‑708. | Crossref
- Danese S, Semeraro S, Papa A, et al. Extraintestinal manifestations in inflammatory bowel disease. World J Gastroenterol. 2005, 11: 7227‑7236. | Crossref
- Patedakis Litvinov BI, Pathak AP. Granulomatous hepatitis in a patient with Crohn’s disease and cholestasis. BMJ Case Rep. 2017; 2017: bcr‑2017‑220988. | Crossref
- Drebber U, Kasper HU, Ratering J, et al. Hepatic granulomas: histological and molecular pathological approach to differential diagnosis – a study of 442 cases. Liver Int. 2008, 28: 828‑834. | Crossref
ARTICLE INFORMATION