Low back pain and osteosclerotic bone lesions suggestive of metastases: a mask of osteopoikilosis



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Low back pain and osteosclerotic bone lesions suggestive of metastases: a mask of osteopoikilosis
A 46‑year‑old woman was referred for diagnostic workup due to low back pain. Magnetic resonance imaging (MRI) of the spine revealed a herniated L5‑S1 disc and degenerative vertebral lesions. Additionally, a left adrenal tumor was found.
The patient was admitted to our Department of Endocrinology to evaluate the adrenal mass. Clinically, except low back pain, the patient denied any other complaints. Hormonal tests confirmed a nonsecreting adrenal tumor. Computed tomography (CT) showed a tumor in the left adrenal gland of 13 × 11 × 12 mm in size and a density of –70 Hounsfield units. The lesion was comparable with that detected on the previous MRI scan and diagnosed as myelolipoma. Apart from that, multiple osteosclerotic lesions of different size and unclear characteristics, possibly metastases, were detected in the pelvic bones and the ribs, which required further diagnostic workup (Figure 1A and 1B). The levels of parathormone, calcium, phosphorus, and alkaline phosphatase were normal, but serum 25‑hydroxyvitamin D concentration was lowered. Both thyroid function and morphology on ultrasound scans showed no abnormalities. The levels of thyroid peroxidase and thyroglobulin antibodies were low.
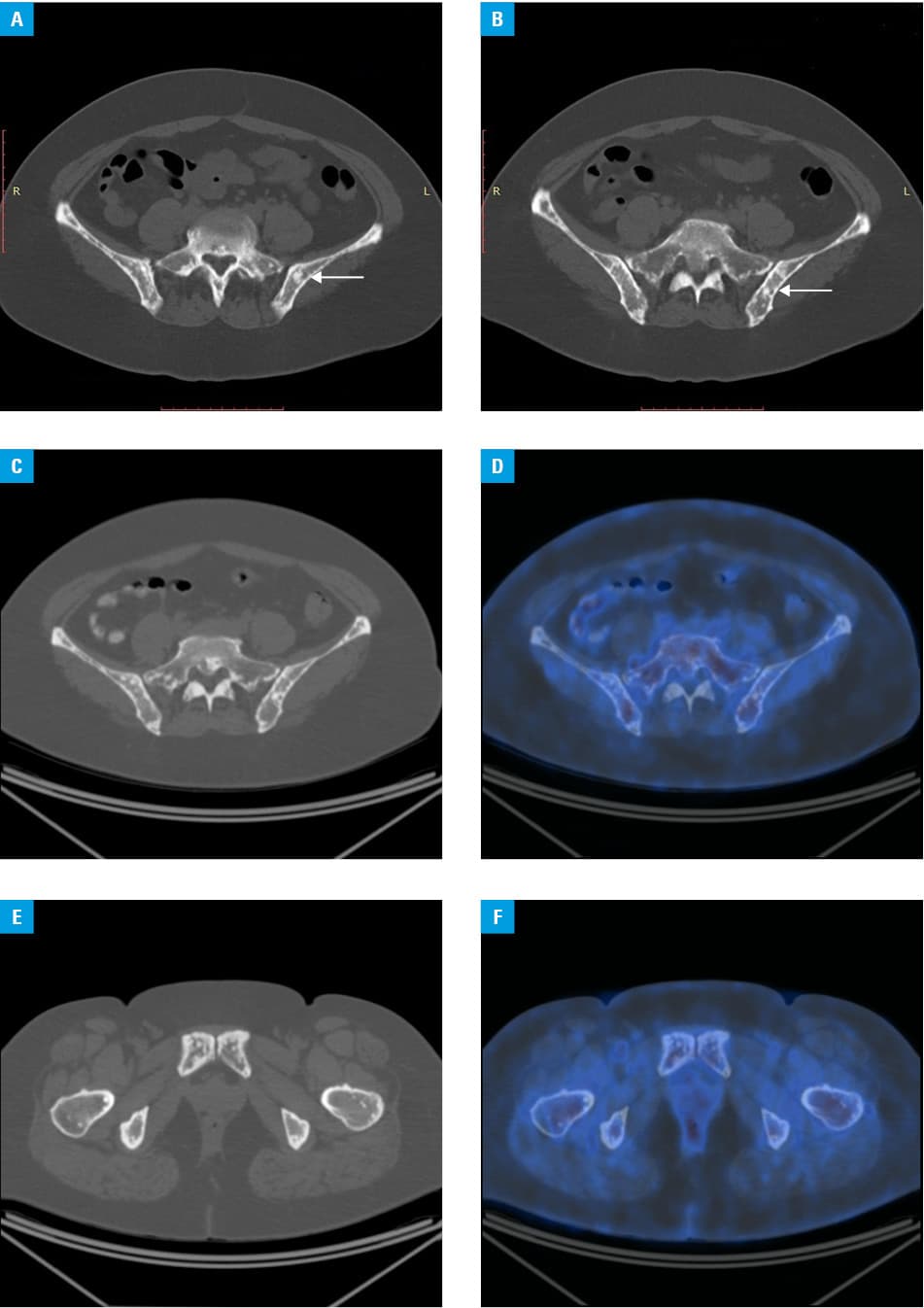
Bone mineral density of the lumbar spine, femoral neck, and forearm was normal for the patient’s age. The L1‑L4 trabecular bone score was unremarkable. Breast ultrasound and chest X‑ray revealed no abnormalities. Then, 18F‑fluorodeoxyglucose positron emission tomography/CT was performed to exclude multiple bone metastases and showed numerous small osteosclerotic lesions with a low uptake of 18F‑fluorodeoxyglucose, particularly in the vertebral column, shoulder girdle, and pelvic bones (Figure 1C-1F). The metastases were excluded and we diagnosed osteopoikilosis (OPK).
Osteopoikilosis is a rare genetic disorder with autosomal dominant pattern of transmission, caused by heterozygous loss‑of‑function mutations in the LEM domain‑containing protein 3 gene (LEMD3). It is usually inherited but may also present sporadically. It affects 1 in 50000 subjects and occurs equally often in men and women.1,2
The disease is characterized by dense bone islands, or improperly developed tissues. The mutation of the LEMD3 gene predisposes to excessive fibrous tissue formation. It carries a high risk of joint immobilization and disability after surgical procedures.2 Osteopoikilosis may be detected at any age and usually incidentally because only up to 20% of the patients present with joint pain, and the remaining subjects are asymptomatic.3
Imaging plays a key role in establishing the diagnosis. Both X‑ray and CT reveal numerous round, ovoid, and linear sclerotic lesions. They are different in size, usually of a few millimeters in diameter, concentrated symmetrically around the metaphyses and epiphyses of the long, carpal, and tarsal bones as well as the pelvis. They are typically absent in the spine, ribs, and skull. On MRI, these lesions are small and dark both in the T1- and T2‑weighted images as they are composed of mature dense bone.4 In our patient, we found typical changes indicative of OPK.
The OPK lesions may occur alone or in association with melorheostosis—a sclerosing bone disease with hyperostosis of the tubular bone cortex, resembling candle wax dripping on the surface of the long bones, usually unilaterally and asymmetrically—or Buschke–Ollendorff syndrome, which is a connective tissue disorder manifested by multiple subcutaneous nevi or nodules.5 Patients with OPK might have autoimmune diseases because the LEMD3 gene influences the expression of transforming growth factor β1, a modulator of immune responses.
Scattered osteosclerotic bone lesions should be differentiated with OPK. Establishing the proper diagnosis is crucial and saves patients a lot of stress and unnecessary diagnostic testing. Occurring alone, OPK is a benign disease and does not require any routine follow‑up. However, it might be comorbid with autoimmune diseases.
- Ng C, Schwartzman L, Moadel R, Haigentz M Jr. Osteopoikilosis: a benign condition with the appearance of metastatic bone disease. J Clin Oncol. 2015; 33: e77‑e78. | Crossref
- Korman B, Wei J, Laumann A, et al. Mutation in LEMD3 (Man1) associated with osteopoikilosis and late‑onset generalized morphea: a new Buschke‑Ollendorf syndrome variant. Case Rep Dermatol Med. 2016; 2483041. | Crossref
- Boulet C, Madani H, Lenchik L, et al. Sclerosing bone dysplasias: genetic, clinical and radiology update of hereditary and nonhereditary disorders. Br J Radiol. 2016; 89: 20150349. | Crossref
- Wallace S, Towbin RB, Towbin AJ. Osteopoikilosis. Appl Radiol. 2019; 48: 40‑41.
- Kotwal A, Clarke BL. Melorheostosis: a rare sclerosing bone dysplasia. Curr Osteoporos Rep. 2017; 15: 335‑342. | Crossref
ARTICLE INFORMATION