A 28‑year‑old male patient was admitted to an orthopedic department with a 4‑year history of severe systemic pain, especially in the chest, bilateral hips, and back. There were no other constitutional symptoms, and no history of trauma or surgery during the past years.
On physical examination, the patient showed a slightly decreased muscle strength in bilateral limbs. The results of general physical examination were also remarkable in terms of sternal tenderness, tapping pain, and crushing chest pain. Routine laboratory investigation and endocrine tests demonstrated hypophosphatemia as well as elevated levels of β-C‑terminal telopeptide of type I collagen and serum alkaline phosphatase. X‑ray imaging of the knee joint showed a significant quasi‑circular high‑density shadow in the right proximal tibia (Figure 1A). Computed tomography and magnetic resonance imaging revealed a tumor with irregular hyperintense signals on T1- and T2‑weighted images, involving the right tibial plateau (Figure 1B–1D). 68Ga‑DOTA‑TATE and 99mTc‑octreotide positron emission tomography and computed tomography identified a high‑intake nodule in the right tibial plateau, with high suspicion of oncogenic osteomalacia (Figure 1E).
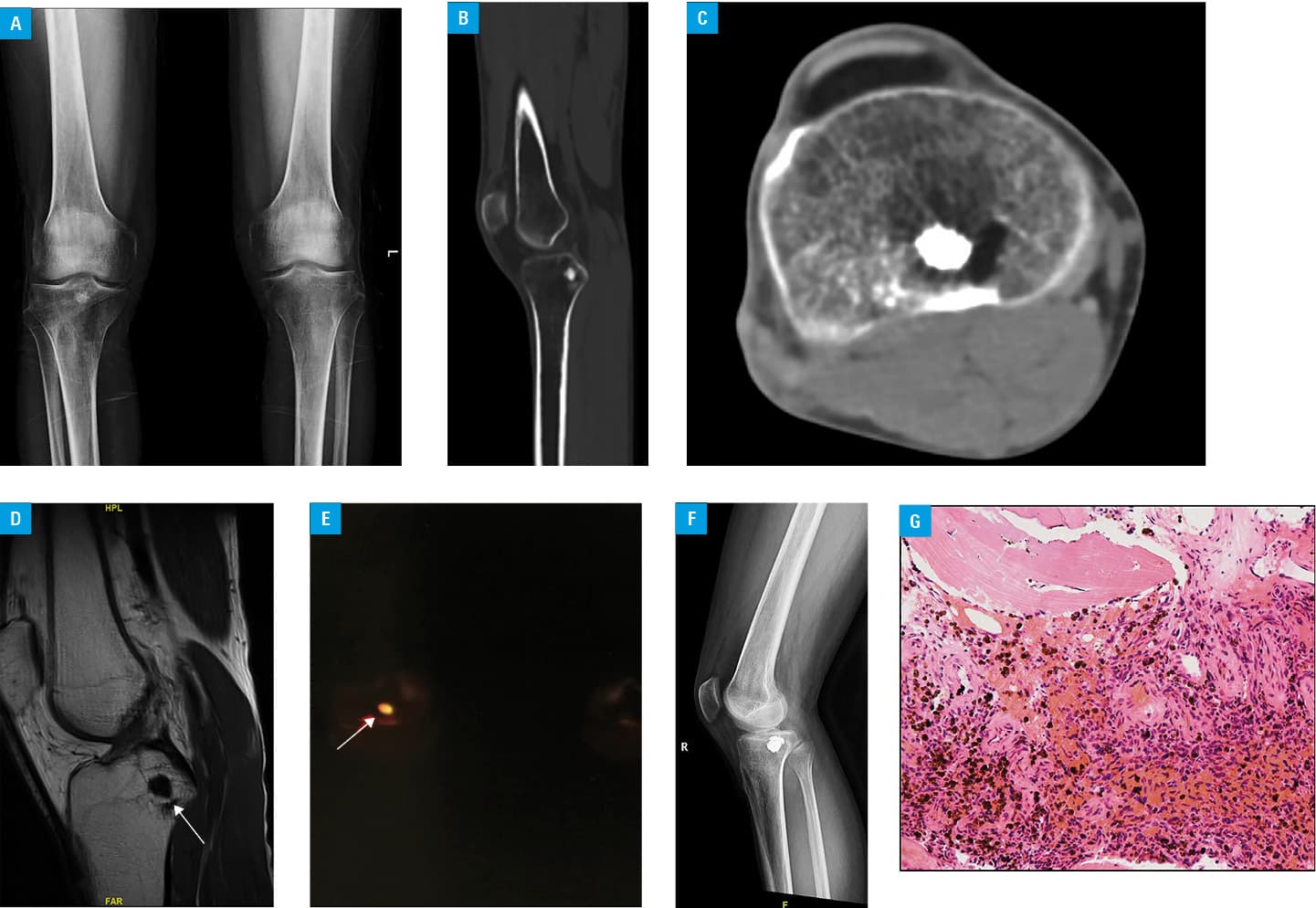
After a detailed analysis, we performed osteoplasty with bone cement, and a postoperative posteroanterior radiograph of the hip showed that cement augmentation was satisfactory (Figure 1F). Pathologic examination confirmed oncogenic osteomalacia with evidence of a phosphaturic mesenchymal tumor (Figure 1G). Serum phosphate levels returned to normal following surgery, and the symptoms improved significantly compared with the preoperative status. Moreover, a visual analogue scale score of bone pain improved to 1 to 2 points, as compared with the preoperative status (6 points). Postoperatively, the patient declined adjuvant treatment and was monitored as an outpatient. This is an extremely unique case of surgical management of tumor‑induced osteomalacia with cement augmentation.
Oncogenic osteomalacia was first described by McCance in 1947, and only 500 cases have been reported worldwide.1,2 Its pathogenesis is underlined by the ability of the disease‑causing tumor to produce phosphatonins, including fibroblast growth factor 23, which affects phosphorus reabsorption and vitamin D metabolism by regulating proximal renal tubular sodium–phosphate cotransporter and influencing the function of l-α hydroxylase. This, in turn, leads to a decrease in blood phosphorus levels, an increase in urinary phosphorus levels, and impairment of bone mineralization.2,3
Surgery has been proved to be the first‑choice treatment for patients with oncogenic osteomalacia, which requires a complete removal of tumors and a sufficient resection scope for radical management.4 Blood phosphorus levels gradually increase after resection of the pathogenic tumors, generally returning to normal levels within 2 to 7 days after surgery, and the clinical symptoms can be significantly relieved.5 However, surgery may also seriously affect the local skeletal stability and at the same time limit local motor function of patients. Bone cement has the potential to inhibit the growth of tumors and is expected to become an effective treatment option for patients with oncogenic osteomalacia who cannot undergo an appropriate surgical procedure or refuse open surgery. Cementoplasty has its own advantages over other surgical treatment options in terms of surgical injury and postoperative rehabilitation.4,5 The present case highlights the importance of an accurate diagnosis and proper treatment for patients with oncogenic osteomalacia.
- McCance RA. Osteomalacia with Looser’s nodes (Milkman’s syndrome) due to a raised resistance to vitamin D acquired about the age of 15 years. Q J Med. 1947; 16: 33‑46.
- Zhang Y, Xu C, Yang Y. Tumor‑induced osteomalacia with IgG4‑related lymph node disease. Chin Med J (Engl). 2019; 132: 994‑995. | Crossref
- Shi X, Jing H, Li F, et al. 99mTc‑HYNIC‑TOC in the Evaluation of Recurrent Tumor‑Induced Osteomalacia. Clin Nucl Med. 2019; 44: 209‑213. | Crossref
- Vollbrecht JE, Rao DS. Images in clinical medicine. Tumor‑induced osteomalacia. N Engl J Med. 2008; 358: 1282. | Crossref
- Feng J, Jiang Y, Wang O, et al. The diagnostic dilemma of tumor induced osteomalacia: a retrospective analysis of 144 cases. Endocr J. 2017; 64: 675‑683. | Crossref
ARTICLE INFORMATION