Kidney transplant is considered the best form of kidney replacement therapy.1 Improving quality of life and survival are main benefits of this treatment in patients with chronic kidney disease.1 However, an increased risk of infections2 and malignancies3 related to immunosuppressive treatment may worsen patients’ outcomes. Cancers account for 8% to 30% of all deaths in kidney transplant recipients with functioning grafts.4
A 55‑year‑old man, 17 years after kidney transplant from a deceased donor, with the history of hepatitis C, arterial hypertension, and peripheral arterial disease was admitted to the Department of Nephrology due to fever lasting 2 days, diarrhea, and failure of the transplanted kidney. For about 1 year, cortical cysts of a maximum of 15 mm in diameter were seen in the transplanted kidney on abdominal ultrasound (Figure 1A). During hospitalization, Clostridioides difficile infection was diagnosed and the patient received targeted treatment. Moreover, urinary tract infection was confirmed (Pseudomonas aeruginosa and Klebsiella pneumoniae producing extended‑spectrum beta‑lactamases) and treated with appropriate antibiotics. Despite targeted treatment, fever was still observed and new symptoms, including dyspnea and fatigue, occurred. The patient’s general condition worsened. Pneumonia and peripheral pulmonary embolism were diagnosed. The function of the transplanted kidney was significantly impaired and the dose of immunosuppressive drugs was reduced. Since fever was still present, the patient received immunoglobulins intravenously. After that, the patient’s general condition slightly improved. Bronchoscopy did not show any abnormal findings. Due to nonspecific inflammatory lesions found on chest X‑ray, blood tests were performed to detect possible opportunistic infections. Epstein–Barr virus DNA and herpes simplex virus type 1 DNA were found. Morganella morganii was detected in the sputum culture. Test results for Mycobacterium tuberculosis, Pneumocystis jiroveci, and influenza virus were negative. As the function of the transplanted kidney did not improve, abdominal magnetic resonance imaging was performed (Figure 1B and 1C). It revealed multiple cortical cysts in the transplanted kidney, of a maximum of 20 mm in diameter (Figure 1B and 1C). Moreover, a localized fluid collection of 63 mm × 16 mm in size was found between the peritoneal layers near the kidney (Figure 1B). Despite continuous broad‑spectrum treatment, including blood transfusions and ganciclovir administered intravenously, the patient’s condition worsened. On follow‑up abdominal ultrasound, the transplanted kidney was enlarged and showed diminished corticomedullary differentiation. Furthermore, an abnormal mass of 7 mm in diameter was detected in one of the cysts (Figure 1D). Based on positron emission tomography, a bacterial infection of the transplanted kidney was suspected (Figure 1E and 1F). Fever did not resolve and showed no response to antipyretic, antibacterial, antifungal, and antiviral drugs. Apart from that, the enlarged transplanted kidney was tender to palpation and the team decided to perform graftectomy. Histopathological examination confirmed clear cell carcinoma in the renal medulla (Figure 1G and 1H).
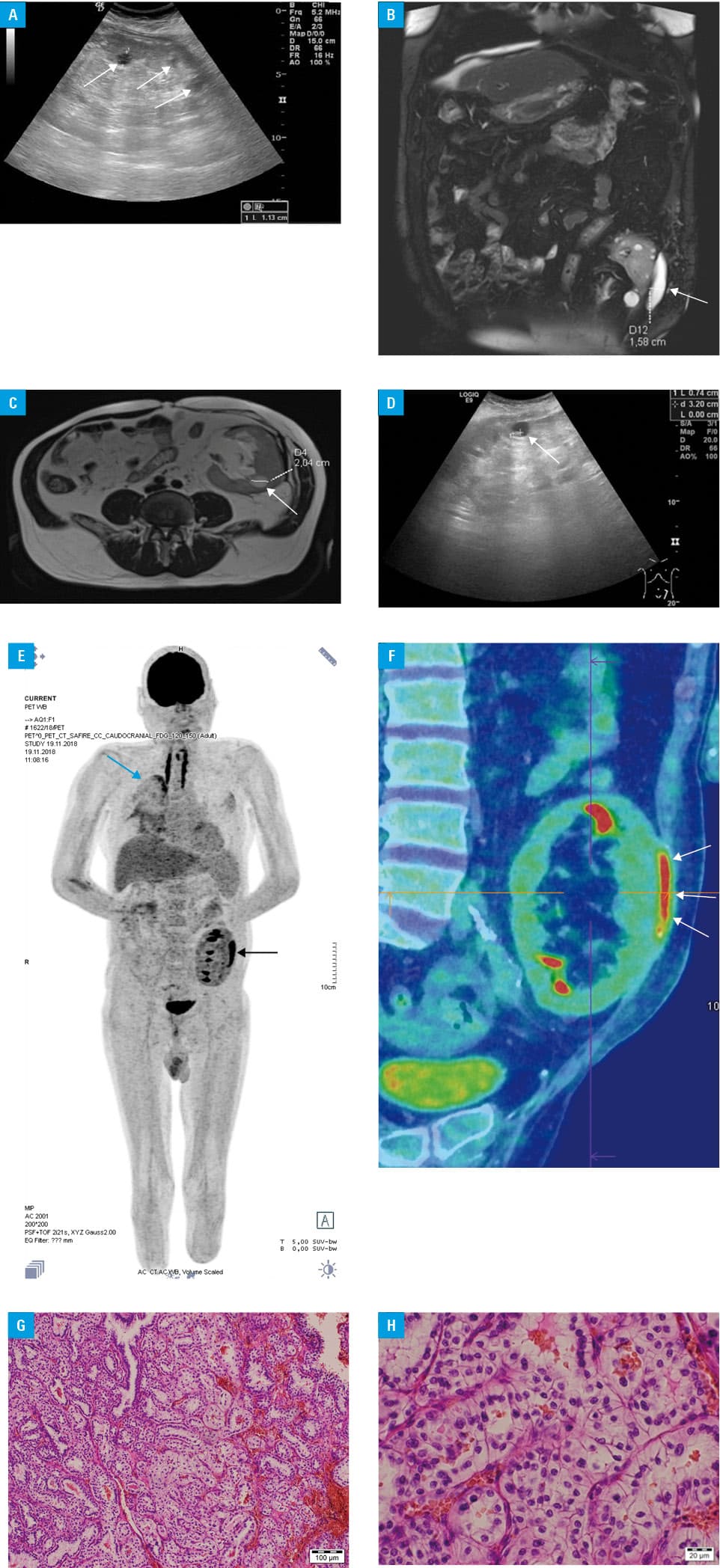
In the presented case, a rare form of renal cancer in the transplanted kidney was shown. Contrary to other organ recipients, cancer in patients after kidney transplant occur almost exclusively in native kidneys.5 Our report highlights the need for paying special attention to kidney transplant recipients with nonspecific symptoms and radiological abnormalities.
- Voora S, Adey DB. Management of kidney transplant recipients by general nephrologists: core curriculum 2019. Am J Kidney Dis. 2019; 73: 866‑879. | Crossref
- Fishman JA. Infection in organ transplantation. Am J Transplant. 2017; 17: 856‑879. | Crossref
- Yang D, Thamcharoen N, Cardarelli F. Management of immunosuppression in kidney transplant recipients who develop malignancy. J Clin Med. 2019; 8. | Crossref
- Sprangers B, Nair V, Launay‑Vacher V, et al. Risk factors associated with post‑kidney transplant malignancies: an article from the Cancer‑Kidney International Network. Clin Kidney J. 2018; 11: 315‑329. | Crossref
- Pilmore H, Dent H, Chang S, et al. Reduction in cardiovascular death after kidney transplantation. Transplantation. 2010; 89: 851‑857. | Crossref
ARTICLE INFORMATION