Characteristics of salivary inflammation in obesity
Key words: inflammatory cytokines, obesity, saliva



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Characteristics of salivary inflammation in obesity
Introduction: The discovery of the secretory function of adipose tissue has led to a new direction in research on obesity‑related health problems. Adipokines are present not only in blood but also in saliva. Numerous studies have indicated that obesity affects salivary concentrations of adipokines.
Objectives: The aim of this study was to evaluate the levels of selected inflammatory markers in saliva and to determine their discriminatory value in obese individuals.
Patients and methods: The study included 125 patients (82 women and 43 men), aged from 20 to 65 years. There were 59 patients with obesity (body mass index [BMI] >30 kg/m2) and 66 controls with normal body weight (BMI <25 kg/m2). Mixed saliva samples were collected from all participants to determine the concentrations of the following inflammatory markers: tumor necrosis factor-α receptors 1 and 2, pentraxin 3, interleukin 15, monocyte chemoattractant protein 1, soluble intercellular adhesion molecule 1, and soluble CD40 ligand (sCD40L).
Results: Compared with controls, individuals with obesity had significantly higher levels of all inflammatory markers except sCD40L levels, which were lower. The salivary marker sCD40L seems to have the best discriminatory value in obesity regardless of sex, with the optimal cutoff point of 3.28 pg/ml and the area under the curve of 0.8.
Conclusions: Obesity may be associated with altered levels of selected inflammatory markers in saliva. The discriminatory values determined in this study may facilitate the diagnosis of metabolic diseases.
What's new?
It is known that obesity is an inflammatory disease and that it is possible to determine the levels of proinflammatory cytokines in saliva. We found differences between the concentrations of selected salivary cytokines in individuals with obesity and normal weight. The salivary marker soluble CD40 ligand has the best discriminatory value for obesity. Our research can help determine the appropriate reference values for selected inflammatory cytokines in saliva, thus improving the diagnosis of inflammatory diseases.
Introduction
Adipose tissue plays an important role in storage of excessive nutrients and regulating energy balance. Due to limited ability of adipocytes for fat deposition, overnutrition generates the production of oxygen free radicals resulting in oxidative stress and, consequently, inflammation. In obesity, low‑grade inflammatory status is primarily caused by the activity of adipocytes and immune cells secreting various proinflammatory molecules, such as tumor necrosis factor-α receptors 1 (TNF-α-R1) and 2 (TNF-α-R2), pentraxin 3 (PTX3), interleukin 15 (IL‑15), monocyte chemoattractant protein 1 (MCP‑1), soluble intercellular adhesion molecule 1 (sICAM‑1), or soluble CD40 ligand (sCD40L). All these signaling molecules are responsible for such processes as chronic systemic inflammation, adipogenesis, atherosclerosis, or insulin resistance, as well as their severe consequences like cardiovascular disease, diabetes, metabolic disorders, carcinogenesis, and severe asthma.1-5
New molecular technologies within the last decade have focused on analyses of salivary proteome and transcriptome. Saliva has been studied as an alternative biological fluid in the noninvasive diagnostics of several systemic diseases, such as endocrine, cardiovascular, autoimmune, or infectious diseases.6,7 Saliva is generally composed of water (about 99%), proteins (eg, enzymes and immunoglobulins), and electrolytes (eg, sodium and calcium). All these substances are delivered to saliva mainly by salivary glands, gingival crevices, and upper respiratory mucosa. The majority of blood components pass to saliva via intracellular mechanisms, such as passive or active transport or ultrafiltration between cell junctions, by analogy to renal production of urine. In patients with obesity, correlations have been reported between the concentrations of several markers in blood and saliva (eg, inflammatory cytokines, adipokines, or cortisol).8,9 Saliva collection is less stressful for patients, is easy to perform, and requires no qualified personnel. These findings indicate that salivary biomarkers have a valuable potential for developing new noninvasive diagnostic techniques.
We aimed to evaluate the salivary levels of selected inflammatory markers and to determine their discriminatory values in people with obesity. Saliva was chosen as an alternative biological fluid to blood.
Patients and methods
Patients
The study included 125 patients (82 women and 43 men) aged from 20 to 65 years. There were 59 patients with obesity (body mass index [BMI] >30 kg/m2) recruited from the Department of Internal and Metabolic Diseases, Poznan University of Medical Sciences (Poznań, Poland). The control group included 66 patients with normal body weight (BMI <25 kg/m2) from the Department of Conservative Dentistry and Periodontology, Poznan University of Medical Sciences. The exclusion criteria were as follows: diabetes, change in body weight (±3 kg) within the last 3 months, history of surgical treatment for obesity, and pregnancy or use of contraceptive agents.
The study was approved by the Bioethical Commission at the Poznan University of Medical Sciences (No. 189/14). Every patient was informed about the aim and type of research to be carried out, and signed informed consent forms were obtained from all patients. All procedures involving human participants were in accordance with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Saliva collection
Unstimulated mixed saliva was used for laboratory studies. Saliva was collected at a specific time of the day, that is, between 10 AM and 1 PM. All samples were collected at least 2 hours after a meal. For proper saliva flow into calibrated tubes on ice, patients were seated in an upright position with their trunks bent forward and were asked to hold swallowing. The tubes containing saliva were kept on ice at all times during the experiment. The unstimulated saliva was collected for a total of 20 minutes and the secreted amount was calculated in ml/min. Immediately after calculation, the saliva was centrifuged for 10 minutes at 2000 rpm using the MPW‑223e centrifuge (MPW Med. Instruments, Warsaw, Poland), aliquoted into tubes, and frozen at a temperature of –80 °C until it was used for the measurement of inflammatory markers. No protease inhibitors were used.
Biochemical and immunological analyses
The pH of saliva after collection was measured using the CG840 pH meter (Schott, Mainz, Germany). To estimate the salivary concentrations of selected inflammatory markers such as TNF-α-R1, TNF-α-R2, PTX3, IL‑15, MCP‑1, sICAM‑1, and sCD40L, an enzyme‑linked immunosorbent assay was used (DuoSet Immunoassay Development kit; R&D Systems, Minneapolis, Minnesota, United States). The spectrophotometric readout of the results was executed using the VERSA microplate reader (Molecular Devices LLC, San Jose, California, United States).
Statistical analysis
The Shapiro–Wilk test was used to verify the normal distribution of the results, and nonparametric methods were used for analyses of results that were not normally distributed. The Mann‑Whitney test was used to compare variables between the study and control groups. The Spearman rank test was used to measure the degree of association between variables. Also, receiver operating characteristic curves were analyzed for tested salivary markers. The significance level was estimated at an α level of 0.05. The analyses were performed using the Statistica 13.1 software (StatSoft, Kraków, Poland).
Results
The characteristics of patients, including the detailed demographic and physical parameters, are shown in Table 1.
Variable | Study group (n = 59) | Control group (n = 66) | All patients (n = 125) | |
Quantitative variables are expressed as median (Q1–Q3) and categorical variables as number (percentage).
Abbreviations: BMI, body mass index; WHR, waist‑to‑hip ratio | ||||
Sex | Female | 46 (78) | 36 (54.5) | 82 (65.6) |
Male | 13 (22) | 30 (45.5) | 43 (34.4) | |
Age, y | 34 (27–40) | 30 (24–36) | 32 (25–37) | |
BMI, kg/m2 | 37.1 (32.7–41.4) | 21.8 (19.4–23.9) | 28.0 (21.7–36) | |
WHR | 0.92 (0.85–0.96) | 0.80 (0.75–0.89) | 0.86 (0.77–0.92) | |
Unstimulated saliva, ml/min | 0.30 (0.23–0.38) | 0.38 (0.25–0.63) | 0.33 (0.25–0.5) | |
Salivary pH | 7.0 (6.8–7.2) | 7.0 (6.7–7.3) | 7.0 (6.7–7.3) | |
The amount of unstimulated saliva secreted by patients with obesity was lower when compared with normal‑weight individuals. However, salivary pH was not lower in the group with obesity.
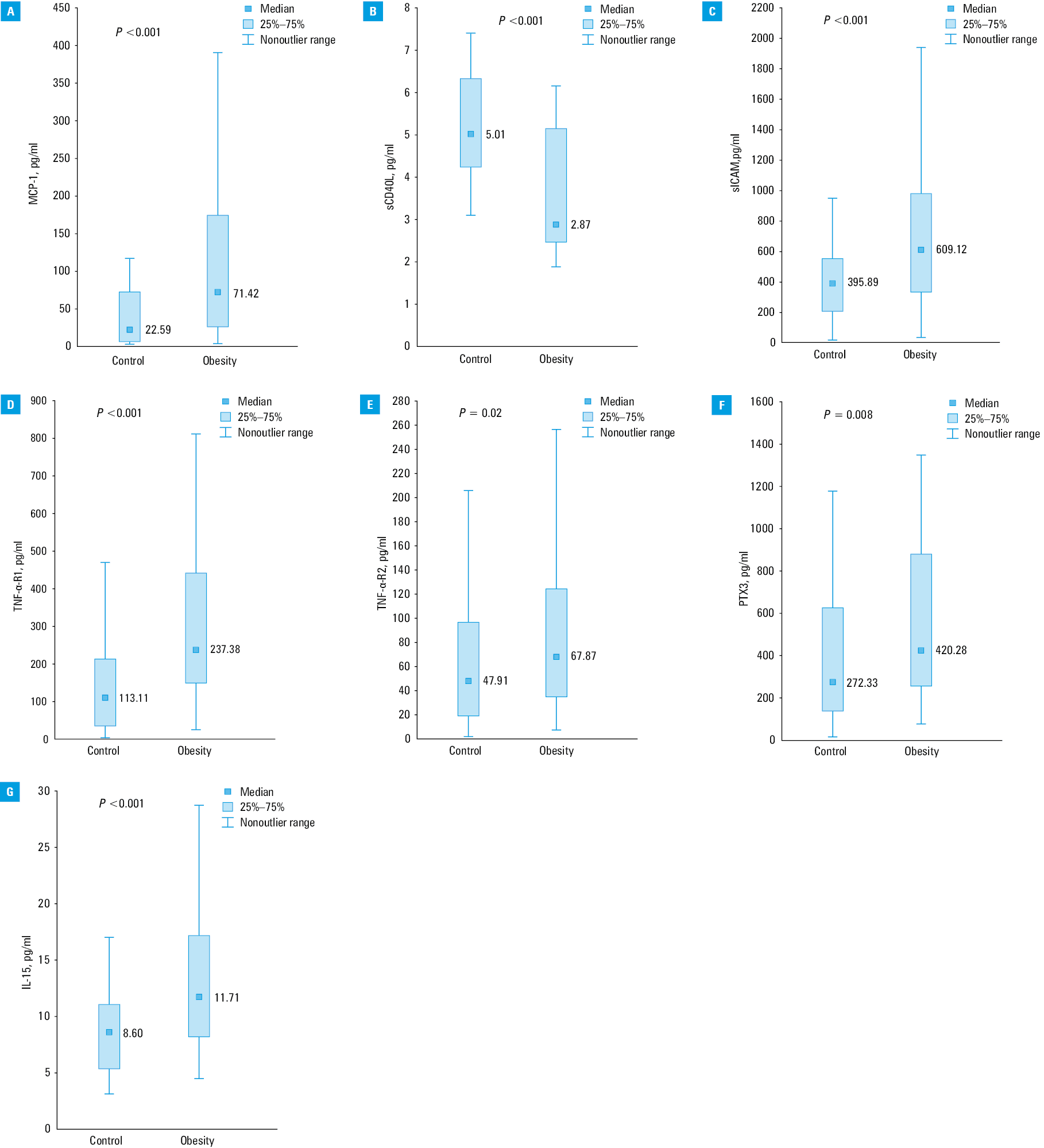
There were significant differences in the concentrations of all inflammatory markers in saliva between patients with obesity and controls (Figure 1A–1G). Significant correlations were noted between different inflammatory markers of both groups. The correlation coefficients are presented in Table 2.
Variable | TNF-α-R1 | TNF-α-R2 | IL‑15 | sCD40L | sICAM‑1 | PTX3 |
a P <0.05
Abbreviations: see Figure 1 | ||||||
MCP‑1 | 0.327a | 0.504a | 0.112 | –0.021 | 0.512a | 0.337a |
TNF-α-R1 | – | 0.547a | –0.011 | –0.006 | 0.457a | 0.391a |
TNF-α-R2 | – | – | –0.048 | 0.199a | 0.679a | 0.634a |
IL‑15 | – | – | – | –0.243a | –0.008 | 0.076 |
sCD40L | – | – | – | – | 0.031 | 0.019 |
sICAM‑1 | – | – | – | – | – | 0.437a |
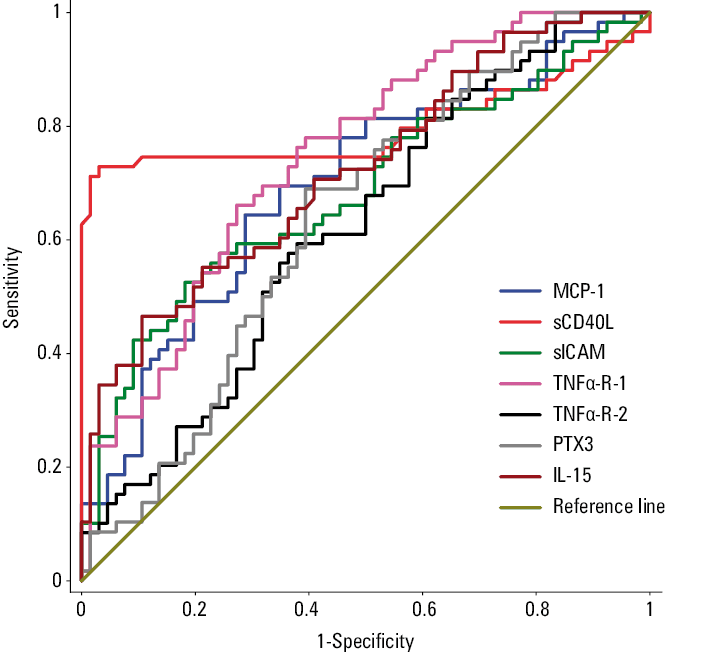
Also, the analysis of the receiver operating characteristic curves by sex was performed to assess the ability of salivary markers to discriminate obesity and determine their potentially optimal cutoff points. The results are shown in Table 3 and Figure 2. All markers had a discriminatory value for obesity, but the best value was noted for sCD40L. Importantly, unlike other markers, lower levels of this ligand were related to a higher risk of obesity.
Variable | Women | Men | Overall | ||||
AUC | P value | AUC | P value | AUC | P value | Optimal cutoff point, pg/ml | |
A P value of less than 0.05 was considered significant.
Abbreviations: AUC, area under the curve; others, see Figure 1 | |||||||
MCP‑1 | 0.658 | 0.009 | 0.8 | <0.001 | 0.696 | <0.001 | 56.12 |
sCD40L | 0.801 | <0.001 | 0.8 | 0.004 | 0.8 | <0.001 | 3.28 |
sICAM‑1 | 0.702 | <0.001 | 0.687 | 0.03 | 0.685 | <0.001 | 606.09 |
TNF-α-R1 | 0.778 | <0.001 | 0.697 | 0.02 | 0.747 | <0.001 | 182.8 |
TNF-α-R2 | 0.624 | 0.047 | 0.595 | 0.28 | 0.62 | 0.02 | 56.39 |
PTX‑3 | 0.628 | 0.049 | 0.641 | 0.11 | 0.637 | 0.006 | 319.44 |
IL‑15 | 0.623 | 0.047 | 0.831 | <0.001 | 0.721 | <0.001 | 13.03 |
Discussion
Individuals with obesity showed higher concentrations of all studied cytokines in saliva, except sCD40L. The present study shows that there are significant differences between components and properties of saliva originating from patients with obesity and individuals with normal body weight.
Previous studies have shown that individuals with obesity have moderate persistent underlying inflammation in the parotid glands coupled with inflammatory mediators secreted by adipose tissue and acting along the hypothalamic–pituitary–adrenal axis, which might contribute to the reduced activity of the salivary glands.10Although the amount of saliva was lower, we did not observe any difference in pH of saliva between study groups.
Our results demonstrate that the concentrations of cytokines produced in the cells of adipose tissue can be estimated not only in blood but also in saliva. A recognized marker of inflammation is MCP‑1. Blood MCP‑1 concentrations have been used in the diagnosis and prognostication of several diseases, such as nephritis, rheumatoid arthritis, and cardiovascular disorders.11,12 Currently, an increased number of investigators analyze the concentrations of cytokines in saliva, in addition to blood. In a very interesting report, Khan13 estimated 57 cytokines, chemokines, growth factors, and acute‑phase proteins of 20 healthy volunteers and compared their concentrations in serum, urine, and saliva. He reported a mean salivary MCP‑1 concentration of 105.0 pg/ml, which is 2‑fold higher than the mean concentration obtained in our control group.
More recently, Goodson et al14studied 10- to 12‑year‑old children with obesity and confirmed that the analysis of saliva can be successfully used to detect metabolic abnormalities induced by excessive body weight, especially in young patients in whom blood sampling may be difficult. The salivary biomarkers of obesity and metabolic disturbances analyzed by Goodson et al14 included the monocyte chemotactic factor, MCP‑1. Its mean concentration in children with obesity was 174.1 pg/ml, similar to the level seen in our study. Currently ongoing investigations have continued to use salivary MCP‑1 in the evaluation of tissue damage and prognosis of head and neck tumors.15
Another cytokine investigated in this study was the CD40/CD40L complex, which is involved in the inflammatory cascade in several autoimmune diseases, including systemic lupus and rheumatoid arthritis.16 The results of several studies have shown that the CD40/CD40L complex, estimated either in blood or serum, is a useful biomarker for the diagnosis of Sjögren syndrome.17 It was also shown that the CD40/CD40L complex participates in the process of programmed cell death or apoptosis in patients with Sjögren syndrome. We found that sCD40L had the best discriminatory value for obesity, regardless of sex. It had the highest area under the curve values among the tested markers. As sCD40L is a destimulant, based on a determined optimal cutoff point, its median salivary concentrations below 3.28 pg/ml can be considered as a potential prognostic marker of obesity. In contrast, all other parameters are stimulants and their cutoff threshold is a measurement above which the probability of obesity potentially increases.
The concentration of sICAM‑1 in saliva is significantly higher in individuals with obesity when compared with individuals with normal weight (609.12 pg/ml vs 395.89 pg/ml). This difference may point to an increased risk for leukocyte (particularly monocyte) adhesion to the vascular endothelium, which, consequently, leads to the formation of foam cells in arteriosclerotic plaques.18 According to previous studies, increased blood concentrations of sICAM‑1 may be observed in asthma, allergic or autoimmune inflammation of the skin, and malignant disease. Another study has reported high levels of sICAM‑1 in the saliva of individuals diagnosed with periodontal disease.19
In our study, a significant difference was detected in median salivary TNF-α-R1 concentrations in individuals with obesity (237.38 pg/ml) when compared with healthy individuals (113.11 pg/ml). This may indicate an increase in TNF-α concentrations and could explain the persistent moderate inflammation and a tendency for cell apoptosis in obese patients. The level of salivary TNF-α-R2 in individuals with obesity (67.87 pg/ml) was also higher than that in the control group (47.91 pg/ml). The available studies assessing TNF-α-R2 levels in saliva pertained to the diagnosis and prognosis of Lichen planus invasions.20 Ghallab et al,21 examining patients with Lichen planus invasions, analyzed the alterations in salivary TNF-α-R2 concentrations after prednisone treatment. Before the application of prednisone, the average salivary concentration of TNF-α-R2 was 350 pg/ml, and this level decreased to 14 pg/ml following treatment. The mean salivary TNF-α-R2 concentration in healthy individuals was only 45 pg/ml.
We also assessed changes in PTX3 levels, a known serum biomarker used for the evaluation of cardiovascular complications and for the evaluation of cardiovascular complications and the severity of atherosclerotic vascular disease.22 Recent studies have shown that, in addition to the known uses of PTX3, its estimation in the saliva is helpful in early diagnosis and estimation of prognosis related to periodontal diseases.23 Our study showed a higher median concentration of PTX3 in individuals with obesity (420.28 pg/ml) when compared with normal‑weight individuals (272.33 pg/ml).
We also noted a significant difference in the levels of another important inflammatory cytokine, IL‑15, between study groups. In the group with obesity, the median concentration was 11.71 pg/ml, as compared with 8.6 pg/ml in the control group. Phalane et al24 reported the mean salivary IL‑15 level of 0.6 pg/ml in patients with tuberculosis, while IL‑15 was undetected in serum. In addition, Khan13 stated that the concentration of IL‑15 could not be estimated in blood, urine, or saliva.
Conclusions
The results of our study add to the current knowledge on the link between inflammation and obesity. This may allow a better monitoring of patients with obesity and also facilitate a more accurate estimation of prognosis. Our study has revealed several positive correlations inflammatory markers and excessive body weight. Hopefully, this will aid the implementation of appropriate steps to screen individuals at risk for obesity, leading to the development of proper preventive guidelines.
The saliva of patients with obesity contained higher concentrations of all the measured inflammatory markers except for sCD40L levels. Salivary biomarkers have the potential to facilitated the diagnosis of other systemic diseases, including many of those which are a consequence of obesity. Our study could help elucidate the pathomechanism of obesity. Establishing reference values for the proinflammatory cytokines in saliva would allow a better monitoring of general health in patients with obesity. Further research is necessary to implement systemic solutions for patients with obesity.
- Pîrsean C, Neguț C, Stefan‑van Staden R‑I, et al. The salivary levels of leptin and interleukin‑6 as potential inflammatory markers in children obesity. PloS One. 2019; 14: e0210288. | Crossref
- Maliszewska K, Adamska‑Patruno E, Krętowski A. The interplay between muscle mass decline, obesity, and type 2 diabetes. Pol Arch Intern Med. 2019; 129: 809‑816. | Crossref
- Miethe S, Guarino M, Alhamdan F, et al. Effects of obesity on asthma: immunometabolic links. Pol Arch Intern Med. 2018; 128: 469‑477. | Crossref
- Nunes LAS, Mussavira S, Bindhu OS. Clinical and diagnostic utility of saliva as a non‑invasive diagnostic fluid: a systematic review. Biochem Medica. 2015; 25: 177‑192. | Crossref
- Desai GS, Mathews ST. Saliva as a non‑invasive diagnostic tool for inflammation and insulin‑resistance. World J Diabetes. 2014; 5: 730‑738. | Crossref
ARTICLE INFORMATION