Impact of disseminated tumor cells in the bone marrow on survival and disease progression in patients with left-sided colorectal cancer
Key words: circulating tumor cells, distant metastases, left-sided colon cancer, overall survival, prognostic biomarker



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Impact of disseminated tumor cells in the bone marrow on survival and disease progression in patients with left-sided colorectal cancer
Introduction: Disseminated tumor cells (DTCs) are a subset of circulating tumor cells that migrate to the bone marrow. Colorectal cancer is a heterogeneous disease depending on the site of the primary tumor.
Objectives: We aimed to assess the association between the presence of DTCs in the bone marrow and tumor characteristics as well as long‑term treatment outcomes in patients with left‑sided colorectal cancer.
Patients and methods: This prospective study included 91 patients with left‑sided colorectal cancer (37 with colon cancer and 54 with rectal cancer) treated between 2007 and 2012 in a single tertiary center. Fifteen patients had stage I cancer; 26, stage II; 26, stage III; and 24, stage IV. Overall survival and cancer relapse rates were compared between patients with different cancer stages and DTC status.
Results: Bone marrow DTCs were identified in 42 patients (46.1%). The prevalence of DTCs was not related to tumor infiltration depth, nodal involvement, distant metastasis, tumor stage, or primary tumor site. The 5‑year overall survival rates were 59.5% and 53% in the DTC‑positive and DTC‑negative groups, respectively (P = 0.19). There was a notable trend favoring survival in patients with DTCs with stage II and III disease (both separately and when combined). The number of metachronous distant metastases was significantly lower in DTC‑positive patients.
Conclusions: The presence of DTCs in the bone marrow is not associated with primary tumor characteristics and seems to reduce metastasis formation in left‑sided colorectal cancer. There is also a trend for improved overall survival in DTC‑positive patients. These results are intriguing and warrant further confirmation.
What's new?
Our study showed a significantly lower number of metachronous distant metastases in patients with left‑sided colorectal carcinoma and disseminated tumor cells (DTCs) in the bone marrow than in those without DTCs. The presence of DTCs in the bone marrow was not a negative predictive factor of distant metastases or a negative prognostic factor in our study group. This supports the concept that there are substantial differences between the characteristics of colorectal cancer depending on affected sites. This issue should be addressed in future studies in order to develop a tailored approach for patients with this malignancy.
Introduction
The significance of disseminated tumor cells (DTCs) in the bone marrow of patients with colorectal cancer is unclear. The presence of DTCs in the bone marrow is identified in 17% to 64% of this population (median, 29%).1 These cells are a subset of circulating tumor cells that migrate to the bone marrow and can form micrometastases. This phenomenon is mostly described in patients with breast cancer. Although DTCs in the bone marrow are present in a substantial percentage of cancer patients without distant or nodal metastases, most of them will not develop distant metastases. Additionally, cancer cells in the bone marrow may be dormant for several years before re‑entering the circulation; however, such situations are very uncommon in colorectal cancer. Two meta‑analyses of studies on the prognostic significance of circulating cancer cells in colorectal cancer indicated that the presence of DTCs in the peripheral blood is a negative prognostic factor.2,3
At present, there is insufficient evidence to confirm that the presence of DTCs in the bone marrow of patients with colorectal cancer affects the prognosis.4-7 Such studies, especially those on nondisseminated colorectal cancer, require a large number of patients and a long follow‑up, because the median survival in patients with colorectal cancer undergoing radical surgery is longer than 5 years. In addition, colorectal cancer is a heterogenous disease depending on the site affected by the primary tumor. What follows, right- and left‑sided cancers may differ in terms of biological characteristics and prognosis.8-11 Therefore, in this study, we focused on malignancies arising from the left colon and rectum, with an emphasis on locally advanced cancer. In particular, we aimed to assess the relationship between the presence of DTCs in the bone marrow and tumor characteristics, cancer progression, and survival in patients with left‑sided colorectal cancer.
Patients and methods
The study included 91 patients with colorectal cancer treated at a single institution between 2007 and 2012. Only patients with tumors located in the rectum or left colon were included. The term “left colon” was defined as a section of the colon distal to the left one‑third of the transverse colon. The inclusion criteria were age over 18, histologically confirmed cancer, and elective surgical procedure. Patients with synchronous right‑sided colon cancer or those with a history of other neoplastic diseases were excluded. None of the patients with colon cancer received preoperative chemotherapy, while 5 patients with rectal cancer received preoperative radiotherapy and 2—preoperative chemoradiotherapy. The group included 42 women and 49 men (mean [SD] age, 64.7 [10.2] years). The distribution of cancer stage according to the TNM classification was as follows: T1, 2 patients; T2, 16; T3, 60; T4, 13; N0, 42; N1, 20; N2, 25; Nx, 4; M0, 67; and M1, 24. The clinical and pathological characteristics of patients are summarized in Table 1.
Parameter | Patients, n (%) |
Abbreviations: AJCC, American Joint Committee on Cancer; UICC, Union for International Cancer Control | |
Tumor location | |
Left colon | 37 (41) |
Rectum | 54 (59) |
Primary tumor | |
T1 | 2 (2) |
T2 | 16 (18) |
T3 | 60 (66) |
T4 | 13 (14) |
Lymph nodes | |
N0 | 42 (46) |
N1 | 20 (22) |
N2 | 25 (27.5) |
Nx | 4 (4.5) |
Metastases | |
M0 | 67 (73.6) |
M1 | 24 (26.4) |
UICC/AJCC stage | |
I | 15 (16.4) |
II | 26 (28.6) |
III | 26 (28.6) |
IV | 24 (26.4) |
Grade | |
1 | 26 (28.55) |
2 | 45 (49.45) |
3 | 13 (14.3) |
Not assessed | 7 (7.7) |
Resection margins | |
R0 | 63 (69.2) |
R1 | 5 (5.5) |
R2 | 23 (25.3) |
A bone marrow biopsy of the posterior superior iliac spine was performed on the day of surgery after the induction of general anesthesia. A 5‑ml sample of the bone marrow was collected into plastic EDTA tubes.
Pelleted cells from bone marrow samples were incubated with an excessive amount of lysing solution (BD Biosciences, San Jose, California, United States) for 10minutes, repeated 3 to 4 times to remove erythrocytes. The remaining cells were washed in phosphate‑buffered saline (PBS) and adjusted to the concentration of 1 × 107cellsml−1 in PBS. Subsequently, the cells were stained with monoclonal mouse antihuman CD45 (phycoerythrin‑labeled) antibodies (DAKO, Glostrup, Denmark) and sorted into CD45+ and CD45− populations using flow cytometry (FACS Vantage SE, BD Biosciences, Bedford, Massachusetts, United States) equipped with the TurboSort option (BD Biosciences) and Aerosol Protection System (Flexoduct International ApS, Greve, Denmark). The Innova Enterprise II ion laser (Coherent, Santa Clara, California, United States) operating at 488nm was used as a light source. Sorting was performed using a 70‑mm nozzle tip with a drop drive frequency of 65kHz, 1.5‑drop envelopes and a “normal” sorting mode. Sorted CD45− cells were collected into polystyrene Falcon 2057 tubes (BD Biosciences) precoated with fetal calf serum and maintained in a refrigerated bath recirculator (Neslab Instruments, Portsmouth, New Hampshire, United States). About 1 × 106 of CD45– cells (1 × 106cellsml−1) were used to prepare slides. The slides were dried, fixed with a mixture of ethanol and acetone (1:1 vv−1), and then stained for 30minutes with A45‑B/B3 monoclonal antibodies (5µgml−1) (Micromet GmbH, Munich, Germany), which recognize common epitopes of cytokeratins (CKs) including CK8, CK18, and CK19. Subsequently, the slides were washed and stained for 30 minutes with goat anti‑mouse IgG‑FITC‑labeled antibodies (DAKO). After washing with PBS, the slides were assayed within 2 days. The CK+ cells were identified by 2 independent investigators under a BX60 fluorescent microscope (Olympus, Tokyo, Japan) and documented with a DP10 camera (Olympus). At least 300 cells were examined per slide. The samples were regarded as positive when at least 3 CK+ cells were found per slide. Accordingly, patients were classified into CK+ and CK− groups. All CK+ cells were cytologically malignant cells as seen under the microscope. We could not distinguish between different CKs. However, the antibody (A45‑B/B3) was commonly used in research on DTCs in the bone marrow, so the comparison with other studies is possible. The cytokeratins CK8, CK18, and CK19 are the epitopes of normal colonic mucosa, colonic adenoma, and adenocarcinoma. Therefore, the staining of the tumor for these epitopes is not routinely used and was not performed in our patients.
The surgical procedures were carried out according to oncology guidelines. Due to the changes in the TNM staging system during the study period, all the specimens were re‑staged according to the seventh edition. The clinical and pathological data were recorded. Patients received postoperative chemotherapy if indicated, regardless of their DTC status. All patients were followed for at least 5 years or until death, and the dates of death were verified with the census registry office.
All patients provided written informed consent to participate in the study. The study was approved by the Jagiellonian University Ethical Committee (KBET no. 86/B/2007 and KBET no. 122.6120.128.2015) and was registered at ClinicalTrials.gov (registration number, NCT03640572).
Statistical analysis
The statistical analysis was conducted using the Statistica 13 software (Dell, Inc., Tulsa, Oklahoma, United States). The distribution of variables was checked using the Kolmogorov–Smirnov test. Categorical variables were compared with the χ2 test with Yates correction. Survival analysis was performed according to the Kaplan–Meier method and log‑rank test. A P value of less than 0.05 was considered significant.
Results
In our study, CK+ cells were identified in the bone marrow of 42 patients (46.1%): 16 patients with left‑colon cancer (43.2%) and 26 with rectal cancer (48.1%), without a significant difference (Table 2). The prevalence of DTCs was not related to the depth of infiltration (T feature) and was similar in patients with T1‑2 and T4 cancer. There was no significant difference between the prevalence of DTCs in patients with and without distant metastasis. These patients also showed similar rates of DTC detection in the bone marrow. The prevalence of DTCs in the bone marrow of patients with TNM stages I–IV was similar, with a slightly lower prevalence in patients with stage IV cancer. The presence of DTCs in the bone marrow was not related to either the tumor grade or radicality of resection.
Parameter | Left colon (16/37) | Rectum (26/54) | Both sites (42/91) |
Data are presented as the number of disseminated tumor cell–positive patients/the total number of patients with cancer of particular stage, grade, or resection margins (percentage).
Abbreviations: see Table 1 | |||
Tumor | |||
T1–T2 | 0/3 | 10/15 (66.6) | 10/18 (55) |
T3 | 13/29 (44.8) | 12/31 (38.7) | 25/60 (41.7) |
T4 | 3/5 (60) | 4/8 (50) | 7/13 (53.8) |
Lymph nodes | |||
N– | 5/15 (33.3) | 14/27 (51.9) | 19/42 (45.2) |
N+ | 10/21 (47.6) | 9/24 (37.5) | 19/45 (42.2) |
Nx | 1/1 (100) | 3/3 (100) | 4/4 (100) |
Metastases | |||
M0 | 11/28 (39.2) | 21/39 (53.8) | 32/67 (47.7) |
M1 | 5/9 (55.5) | 5/15 (33.3) | 10/24 (41.6) |
Grade | |||
G1–G2 | 12/29 (41.3) | 21/42 (50) | 33/71 (46.5) |
G3 | 3/6 (50) | 0/7 | 3/13 (23) |
Not assessed | 1/2 (50) | 5/5 (100) | 6/7 (85.7) |
UICC/AJCC stage | |||
I | 0/3 | 7/12 (58.3) | 7/15 (46.6) |
II | 5/12 (41.7) | 7/14 (50) | 12/26 (46.2) |
III | 6/13 (46.2) | 7/13 (53.8) | 13/26 (50) |
IV | 5/9 (55.5) | 5/15 (33.3) | 10/24 (41.6) |
Resection margins | |||
R0 | 10/28 (35.7) | 20/35 (57.1) | 30/63 (47.6) |
R1 | 1/1 (100) | 0/4 | 1/5 (20) |
R2 | 5/8 (62.5) | 6/15 (40) | 11/23 (47.8) |
The number of patients who received preoperative treatment was low. Nonetheless, 5 patients with rectal cancer received preoperative radiotherapy, and 3 of them had DTCs in the bone marrow. Moreover, 2 patients with rectal cancer received preoperative chemoradiotherapy, and 5 weeks after treatment completion, both of them were found to harbor DTCs in their bone marrow.
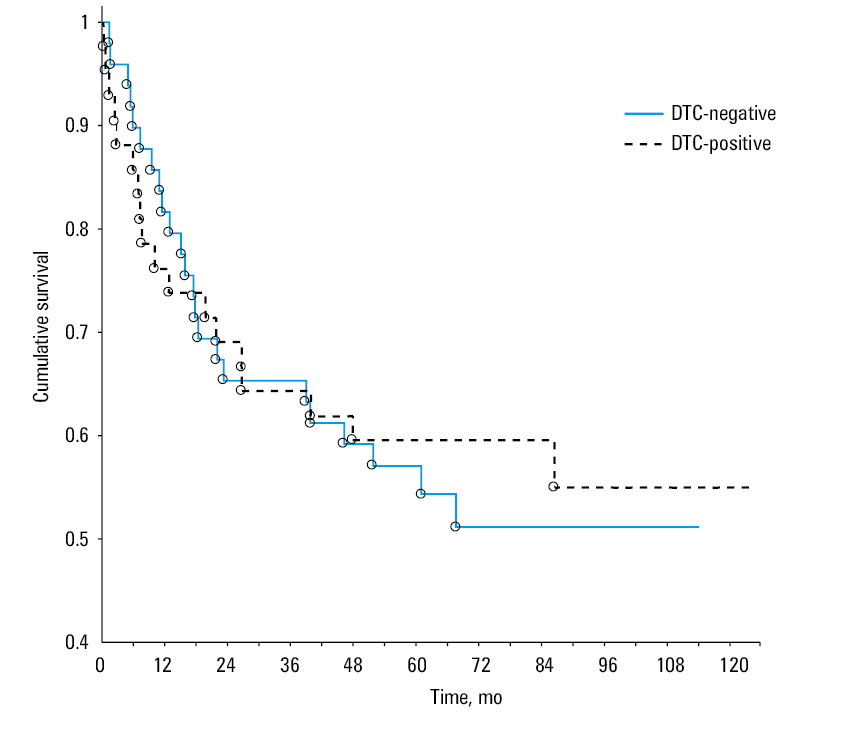
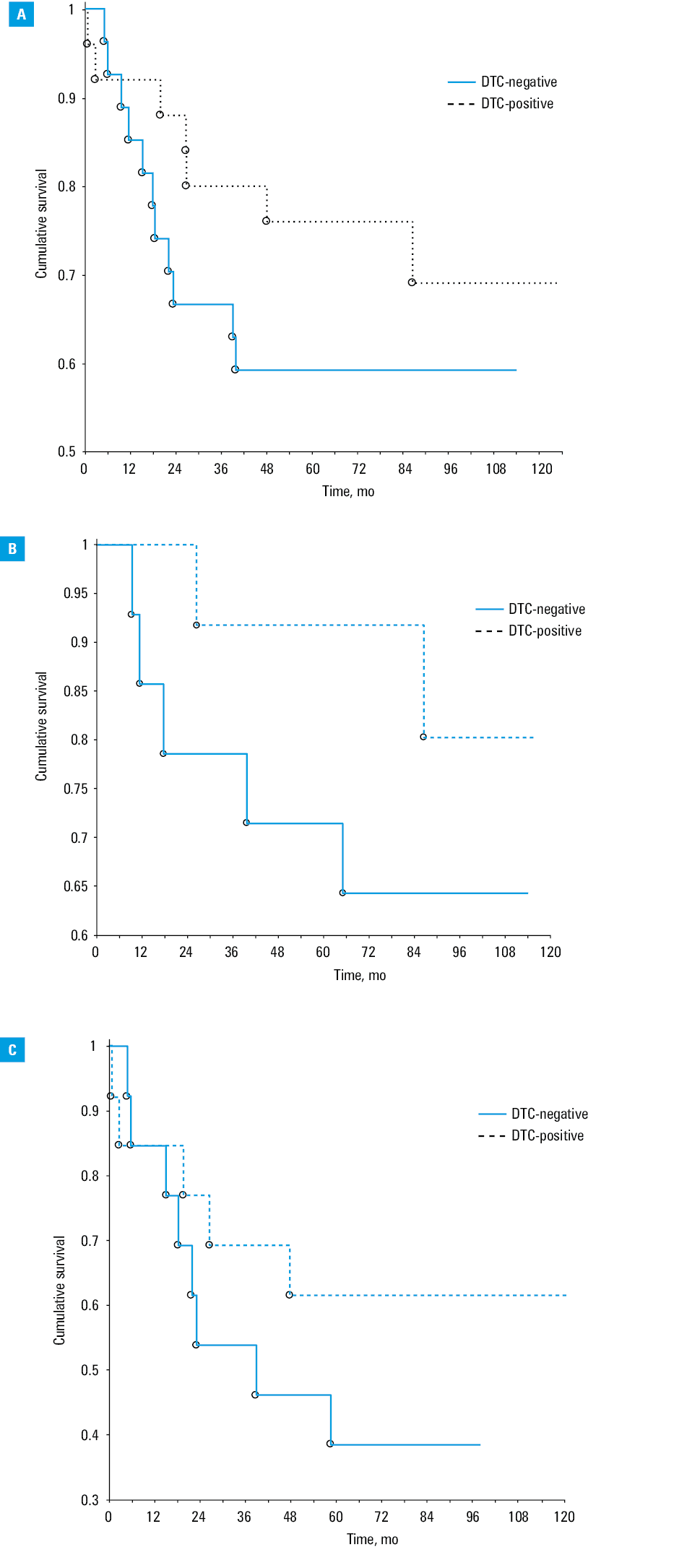
All patients were followed for at least 5 years. The 5‑year survival rate for DTC‑positive patients was 59.5%, while for DTC‑negative ones, it was 53%. The difference between groups was not significant (Figure 1). As DTC could theoretically lead to distant metastasis and cancer progression, a further analysis of patients with stage II and III disease was performed. Stage IV patients were excluded, because they already had disseminated disease, while stage I patients were excluded due to a very low probability of tumor progression. In the group of patients with stages II and III, the 5‑year survival rates were 59.2% and 76% for DTC‑negative and DTC‑positive patients, respectively (Figure 2A). Even though the difference was almost 17% in favor of DTC‑positive patients, it was not significant. The number of patients in stages II and III in the DTC‑negative group was 14 and 13, respectively, and in the DTC‑positive group, 12 and 13, respectively. The mean age of DTC‑negative patients was 63 years, while in the DTC‑positive group, it was 65.3 years. A trend towards better survival in DTC‑positive patients was also observed when we analyzed patients with stages II and III cancer separately; however, the number of patients was too small to obtain significant results (Figure 2B and 2C).
Disease recurrence was assessed in stages II and III. Metastatic disease was diagnosed in 13 patients (25%). The sites of metastasis differed, with the prevalence of liver metastasis (7 of the 13 patients). In the DTC‑negative group, 10 cases of metastasis were observed, while in the DTC‑positive group, only 3 cases (P = 0.038).
Discussion
This study was started in 2007 and we decided to use methodology already established for gastric cancer in patients with colorectal cancer.12 The preliminary results were not published earlier, as such a study requires long‑term follow‑up. As of now, all participants have been followed for at least 5 years. Our population was more homogenous than those in other studies, because we recruited only patients with left‑sided colon and rectal cancer. Most studies included patients with both left- and right‑sided colorectal cancer or only those with rectal cancer. Right‑sided colon cancer has different clinical and molecular characteristics than left‑sided colon and rectal cancer; therefore, it should be analyzed separately in clinical and scientific studies.13
In our study, DTCs in the bone marrow were diagnosed in 46.1% of patients. Other studies reported an incidence between 10% and 63.6% of cases,7,14 although the majority of studies reported a range between 25% and 40%. With the high number of epitopes of the tumor cells used and different methods of detection (immunocytochemistry, immunomagnetic assay, or reverse‑transcription polymerase chain reaction), there is no standard method for identifying DTCs in the bone marrow.15 The rate of detection differs depending on the technique used, even within a single study.16,17 The method that we used in this study is based on fluorescence‑activated cell sorting and the detection of cells expressing the common epitope of CK8, CK18, and CK19 within the sorted population. Therefore, this approach may be more sensitive than other simpler methods, because the cell population is enriched with the initial sorting.
In our study, the incidence of DTCs in the bone marrow was not related to the depth of tumor infiltration, nodal involvement, or distant metastasis. A similar finding was described in a German study of patients with colon cancer.16 However, in that study, over 40% of patients had tumors in the right‑sided colon. Our results were corroborated also by other studies in diverse groups of patients with colorectal cancer,4,7 while some other investigations provided contradictory results.18,19 There is also a common opinion that the tumor grade does not influence the rate of DTCs in the bone marrow.4,16
We observed no difference in the prevalence of DTCs between patients with left colon and those with rectal cancer. This is in line with other studies.4,20 For patients with colon cancer, neoadjuvant therapy is the exception and not the standard treatment, but patients with rectal cancer may receive preoperative radiotherapy or chemoradiotherapy according to indications. In our study, only 7 patients with rectal cancer underwent preoperative treatment. While this number is low, this method was not used routinely in the initial study period. It was not expected that the short‑course radiotherapy would affect DTCs; however, 5 weeks of chemoradiotherapy could potentially eradicate such cells. The study on DTCs in rectal cancer showed that they are identified less frequently in patients who responded to preoperative chemoradiotherapy.21 Moreover, in a study on gastric cancer, chemotherapy was reported to significantly reduce the prevalence of DTCs in the bone marrow.22 We observed only 2 patients who received preoperative chemoradiotherapy. After this therapy, both of them were DTC positive. Although this observation has no statistical power, it shows that the preoperative treatment did not bias the results in patients with rectal cancer.
The overall survival at 5 years was similar between the DTC‑positive and DTC‑negative groups. Both groups also had comparable cancer stages according to the TNM classification. This finding alone is not surprising, as previous studies demonstrated that the presence of DTCs in the bone marrow may not be a negative prognostic factor in patients with colorectal cancer. This is also in line with conclusions from a meta‑analysis published in 2010.23 However, the authors emphasized that the methods of DTC detection were inhomogenous. Therefore, new studies with new populations of patients diagnosed using a specific method are still needed. For further analysis in our study, we excluded patients with the most advanced disease stage, namely, stage IV. The prognostic significance of bone marrow DTCs was described in stage IV colorectal cancer, but only in patients after a curative resection of liver metastasis.24 On the other hand, other investigators demonstrated that this phenomenon may be related to the method of detection.17 We were unable to identify a study that would show the prognostic significance of DTCs in patients with stage IV colorectal cancer who did not undergo a radical resection of metastasis. In our study, only 1 patient with stage IV cancer had a simultaneous liver resection for metastasis. Also, stage I patients were excluded due to a very low probability of cancer progression with definitive treatment. Other studies, especially those with small sample sizes, included stage I patients,5 but larger studies investigated mainly those with stage II and III disease.4 When patients with stages II and III were analyzed together, the 5‑year survival rate in our study was similar between patients with and without DTCs. These results are in contrast to a recent publication from Switzerland, where bone marrow cells were identified with the same type of pan‑CK antibody, with a detection rate similar to that in our study, in patients with stages I–III. The authors found that the presence of DTCs in the bone marrow was a negative prognostic factor for survival.25 However, in contrast to our study, they excluded patients with rectal cancer and only about 40% of patients had left‑sided cancer. Moreover, their findings were not corroborated by some other studies.7,20
In our study, the survival plots showed a trend favoring patients with DTCs in the bone marrow, but the results were not significant. Therefore, we attempted to assess the incidence of distant metastasis during the 5‑year follow‑up. Theoretically, tumor cells located in the bone marrow could be the source of distant metastasis. What follows is that there should be a correlation between DTCs and metachronous metastasis. Such associations have been observed in breast,26 prostate,27 and esophageal cancer.28 Surprisingly, in our study, there was a significantly lower number of metachronous distant metastases in patients with DTCs than in those without. The reason for this finding may be the low number of patients; however, this number is not significantly lower than in the majority of similar studies of patients with the same TNM stages. This observation may indicate that the presence of DTCs might have prevented the progression and metastasis formation. There are hypotheses explaining why DTCs do not influence cancer progression,29 but they do not focus on the beneficial effect of this phenomenon. Bone marrow is a specific site with a number of hematopoietic and immunocompetent cells and also stem cells. DTCs are present during the generation and maturation of various immunocompetent cells. It was demonstrated that the generation of monocytes from hematopoietic CD34+ stem cells from the bone marrow of patients with colon cancer is possible, and these cells act as antigen‑presenting cells. They may present tumor‑specific antigens to cytotoxic T lymphocytes.30 Moreover, it was shown that after in vivo exposure to blood‑derived cell- and tumor‑associated antigens, bone marrow dendritic cells were capable of inducing systemic protective T cell–mediated antitumor immunity upon adoptive transfer.31 In contrast to the bone marrow, responses of lymph nodes to blood‑circulating antigen were only weak. There is evidence that bone marrow–derived dendritic cells differ from peripheral blood–derived dendritic cells, but the significance of this difference is unclear.32Bone marrow also seems to be a preferential site for migration and/or selective retainment of memory T cells and becomes enriched with antigen‑specific memory T lymphocytes in response to viral infection or tumor development.33,34 This mechanism may underlie the finding observed in our study. Surrounded by immune cells, DTCs may be the source of tumor‑related antigens and generate an immune reaction against these antigens. Therefore, DTCs may act as a kind of cancer vaccination.Previous studies have shown that blood circulating breast cancer cells may settle in the bone marrow and spleen. At these sites, antigen‑presenting cells may pick up, process, and cross‑present tumor‑associated antigens to prime naive T lymphocytes. This may lead to generation and maturation of specific effector and also memory T cells. Particular clones of so activated cytotoxic T lymphocytes, upon contact with tumor cells, may exhibit cytotoxic activity or even control dormant cancer foci.35 It was also proposed that small amounts of persisting tumor‑associated antigens produced by dormant tumor cells from the bone marrow may contribute to the maintenance of tumor‑specific and long‑term memory mediated by appropriate subsets of memory T lymphocytes.36The presence of DTCs in the bone marrow is not associated with primary tumor characteristics and seems to reduce metastasis formation in left‑sided colorectal cancer. There is a trend for improved overall survival in DTC‑positive patients.
- Akagi Y, Kinugasa T, Adachi Y, Shirouzu K. Prognostic significance of isolated tumor cells in patients with colorectal cancer in recent 10‑year studies. Mol Clin Oncol. 2013; 1: 582‑592. | Crossref
- Yang C, Zou K, Zheng L, Xiong B. Prognostic and clinicopathological significance of circulating tumor cells detected by RT‑PCR in non‑metastatic colorectal cancer: a meta‑analysis and systematic review. BMC Cancer. 2017; 17: 725. | Crossref
- Groot Koerkamp B, Rahbari NN, Büchler MW, et al. Circulating tumor cells and prognosis of patients with resectable colorectal liver metastases or widespread metastatic colorectal cancer: a meta‑analysis. Ann Surg Oncol. 2013; 20: 2156‑2165. | Crossref
- Flatmark K, Borgen E, Nesland JM, et al. Disseminated tumor cells as a prognostic biomarker in colorectal cancer. Br J Cancer. 2011; 104: 1434‑1439. | Crossref
- O’Connor OJ, Cahill RA, Kirwan WO, Redmond HP. The impact of bone marrow micrometastases on metastatic disease‑free survival in patients with colorectal carcinoma. Colorectal Dis. 2005; 7: 406‑409. | Crossref
ARTICLE INFORMATION