A 36‑year‑old woman with recurrent epigastric pain underwent laparotomy due to gastric ulcer perforation 2 days after labor. After surgery, the levels of inflammatory markers remained elevated. Ultrasonography revealed liver tumor and abdominal abscesses, and the patient underwent repeat surgery. Histopathology of the tumor revealed a metastasis of neuroendocrine tumor (NET) G2. Thus, the patient was admitted to the Department of Endocrinology.
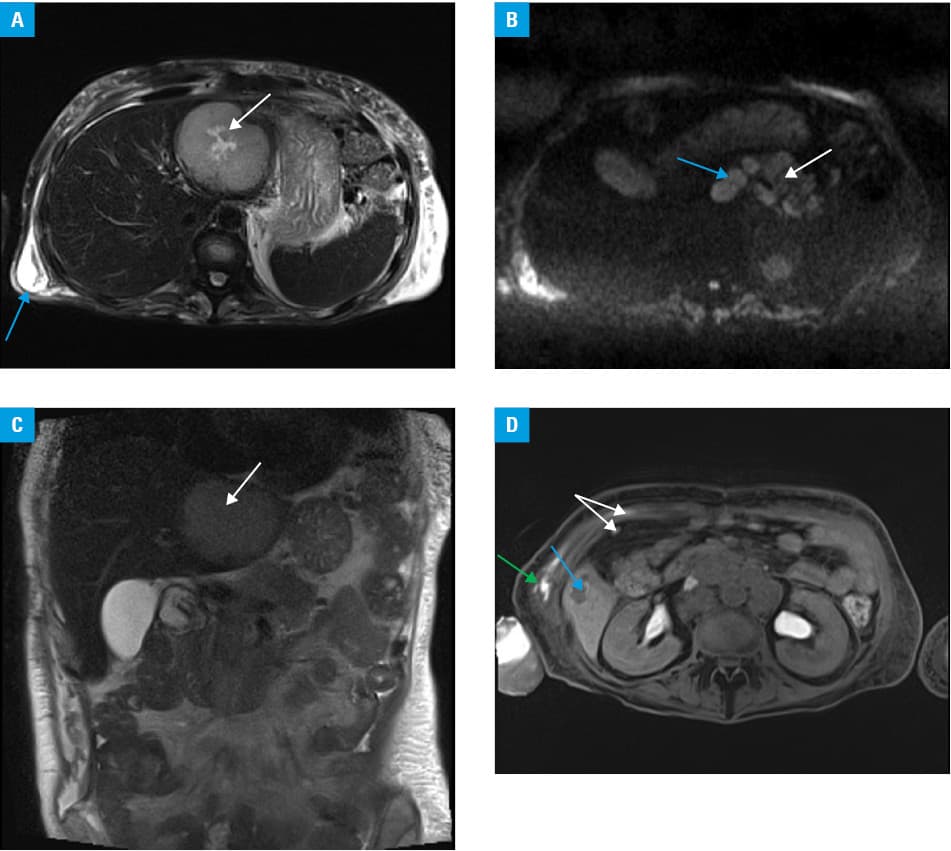
Abdominal computed tomography and magnetic resonance imaging (MRI) of the left liver lobe showed a tumor of 80 × 70 × 75 mm in size with central necrosis and a pancreatic tail tumor of 41 × 54 mm in size; peritoneal and extraperitoneal lymph nodes were enlarged. In the retroperitoneum, abscesses of up to 115 × 60 mm in size were observed (Figure 1). Laboratory tests revealed increased gastrin (2888 pg/ml; 23–115 pg/ml), chromogranin A (699 µg/l; 0–100 µg/l), and serotonin levels (158 ng/ml; 80–450 ng/ml) as well as elevated 24‑hour urinary serotonin excretion (1386 µg/24 h; 50–250 µg/24 h). No additional endocrinopathies were found and gastrinoma was diagnosed. On 18F‑fluorodeoxyglucose positron emission tomography and computed tomography, a slightly increased metabolism in the pancreatic tail tumor, liver metastasis in segment 2, retroperitoneal lymph nodes, and left supraclavicular lymph node were observed. Single‑photon emission computed tomography and computed tomography with 99mTc‑DOTATOC showed somatostatin receptor expression at the same sites and additionally in 2 more liver metastases (segments 4 and 5). The T3N1M1 stage IV NET was diagnosed according to the TNM classification. Because of the clinical status, advanced disease stage, and numerous surgical complications that developed before the diagnosis, the patient was considered ineligible for surgery. Systemic therapy with somatostatin analogues and radionuclide therapy (177Lu‑DOTATATE and 90Y‑DOTATATE, 3.7 GBq) were applied. The patient’s condition stabilized.
Seven months after the diagnosis, the patient developed features of clinical hypercortisolism, hypertension, hypokalemia, and diabetes requiring insulin. Cortisol and adrenocorticotropic hormone (ACTH) levels were increased, without typical circadian rhythms (cortisol, 30 µg/dl and 29.7 µg/dl and ACTH, 161 pg/ml and 170 pg/ml at 8.00 AM and 12.00 PM, respectively), and 24‑hour urinary free cortisol (UFC) excretion was elevated (1626 µg/24 h; reference range <75 µg/24 h). Serum cortisol and UFC levels remained elevated after high‑dose dexamethasone suppression (28.5 µg/dl and 1532 µg/24 h, respectively). The levels of ACTH and cortisol were not affected by the administration of corticotropin‑releasing hormone and desmopressin. Pituitary MRI revealed no adenoma. Ectopic Cushing syndrome was confirmed. After administration of ketoconazole (600 mg/d), the UFC excretion halved but remained elevated (293.7 µg/24 h). It was not possible to increase a ketoconazole dose due to liver dysfunction. At the same time, radiologic disease progression was observed, and second radionuclide therapy was administered (177Lu‑DOTATATE, 7.4 GBq). A month later, 1 year after the diagnosis of gastrinoma, the patient died probably of pulmonary embolism, despite thromboembolic prophylaxis (low‑molecular‑weight heparin).
Gastrinomas are rare functional NETs (0.5–21.5 cases per million persons annually) found mostly in the pancreas or duodenum. They occur sporadically in about 75% to 80% of cases, or in association with multiple endocrine neoplasia type 1. The gastrin secretion stimulates excessive gastric acid production and causes Zollinger–Ellison syndrome.1 Additional ectopic ACTH secretion by a malignant gastrinoma has been rarely described, but according to some authors, it may occur in up to 5% of cases.2 The established diagnosis of the tumor secretion does not exclude the occurrence of a new functional tumor activity, which significantly worsens the prognosis and requires additional treatment (steroidogenesis inhibitors) as well as prevention of opportunistic infections and thromboembolic events.2-5
- Falconi M, Eriksson B, Kaltsas G, et al. ENETS consensus guidelines update for the management of patients with functional pancreatic neuroendocrine tumors and non‑functional pancreatic neuroendocrine tumors. Neuroendocrinology 2016; 103: 153‑171. | Crossref
- Maton PN, Gardner JD, Jensen RT. Cushing’s syndrome in patients with the Zollinger‑Ellison syndrome. N Engl J Med. 1986; 315: 1‑5. | Crossref
- McQuillen DP, Schroy PC, Hesketh PJ, Sugar AM. Pneumocystis carinii pneumonia complicating somatostatin therapy of Cushing’s syndrome in a patient with metastatic pancreatic islet cell carcinoma and Zollinger‑Ellison syndrome. Am J Gastroenterol. 1991; 86: 512‑514.
- Doppman JLK, Nieman LK, Cutler GB Jr, et al. Adrenocorticotropic hormone‑secreting islet cell tumors: are they always malignant? Radiology. 1994; 190: 59‑64. | Crossref
- Said R, O’Reilly EM, Blumgart L, et al. Pancreatic islet cell carcinoma presenting with concurrent Cushing’s and Zollinger‑Ellison syndromes: case series and literature review. Eur J Gastroenterol Hepatol. 2010; 22: 246‑252. | Crossref
ARTICLE INFORMATION