How to diagnose mast cell activation syndrome: practical considerations
Key words: anaphylaxis, epigenetics, mastocytosis, tryptase, urticaria



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
How to diagnose mast cell activation syndrome: practical considerations
Mast cells (MCs) are an important component of the immune system. Their physiological function is involved in multiple areas of human physiology, thus symptoms of their increased activation vary greatly from severe allergic reactions, such as anaphylaxis, to chronic symptoms, such as depression or osteoporosis. Studies on mastocytosis revealed a subgroup of patients presenting symptoms of increased MC degranulation, defined as mast cell activation syndrome (MCAS). This population includes patients with primary MCAS with clonal abnormal MCs, who do not fulfill the criteria for mastocytosis. These symptoms often overlap with comorbidities, which makes the diagnosis and treatment of MCAS difficult. The syndrome is diagnosed on the basis of 3 criteria: 1) the presence of typical symptoms; 2) elevation of serum tryptase levels; and 3) response to anti‑mediator treatment. The diagnosis of MCAS is important especially in patients with anaphylaxis or osteoporosis who require the use of an epinephrine emergency kit and insect venom immunotherapy. In this review, genetic mechanisms and typical symptoms of MCAS as well as its diagnostic criteria and implications were discussed, with a special emphasis on practical guidance with the aim to improve patient care.
Introduction
Mast cells (MCs) constitute an important component of the immune system. They were first described by Paul Ehrlich, a German scientist born in Strzelin in Lower Silesia, who was awarded a Noble Prize for his contribution to immunology in 1908. The physiological function of MCs is related to several areas of human physiology. They are the main effector cells in type I allergic reactions and diseases such as asthma, allergic rhinitis, conjunctivitis, urticaria, and anaphylaxis.1 The binding of allergen to immunoglobulin E (IgE) connected with the FcἐRI receptor on the MC surface leads to the degranulation and release of MC mediators.1
Clinical symptoms caused by local or systemic MC activation are present in the skin (flushing, pruritus, urticaria, and angioedema), respiratory system (nasal congestion, nasal pruritus, wheezing, throat swelling, dyspnea, cough, and stridor), cardiovascular system (hypotension, incontinence, and shock), and gastrointestinal tract (abdominal cramping, abdominal pain, vomiting, and diarrhea).2 Mast cells interact also with the innate and adaptive immune systems in the detection of harmful pathogens such as viruses, bacteria, parasites (mainly helminths), and toxins (eg, Hymenoptera and snakes).2 The cells participate also in wound healing, cancer and tumor progression, and diseases linked to increased fibrosis, such as idiopathic pulmonary fibrosis and multiple sclerosis.2,3 Furthermore, clonal abnormal MCs presenting the KIT mutation (mainly D816V) are found in mastocytosis.4 The disease presents with a wide spectrum of hematologic, allergic, dermatologic, and endocrine symptoms related to abnormal MC infiltration in the bone marrow, skin, and other organs.5
As described above, MC activation is found in a large number of patients. The key element in diagnostic evaluation, especially in the case of anaphylaxis, is to identify individuals with abnormal clonal MCs who may suffer from systemic mastocytosis (SM) or primary mast cell activation syndrome (MCAS). Our patient group involves more than 500 subjects with mastocytosis and MCAS. The present review is based on the European Competence Network on Mastocytosis guidelines and our own experience.
Diagnostic criteria for mast cell activation syndrome
According to the algorithm proposed by Valent et al,2,6 MCAS should be considered when the following 3 criteria are met:
1 Presence of typical and recurrent severe symptoms of excess MC activation (often diagnosed as anaphylaxis affecting at least 2 organs). The typical symptoms include urticaria, flushing, pruritus, wheezing, angioedema, nasal congestion, tachycardia, hypotension, and diarrhea. Headaches, memory loss, and impaired concentration may also be observed, although these symptoms are less specific.
2 Confirmed excess of MC activation in biochemical tests. The preferred marker is tryptase (elevated serum levels by 20% above the upper limit of the normal range or by at least 20% above baseline plus 2 ng/ml within 4 hours after a symptomatic period). Other metabolites include serum and urinary histamine and urine prostaglandin D2, leukotrienes C4 and E4, and 11β-prostaglandin F2α. Prostaglandin D2 in 24‑hour urine collection is considered the most specific marker of excess MC activation, but its availability is highly limited.
3 Positive response to symptom treatment as in mastocytosis. By consensus, this criterion should be fulfilled by antihistamine agents; however, response to other drugs, such as leukotriene receptor blockers, systemic glucocorticoids, and sodium cromoglycate, may also be useful, although they are considered less specific and thus more efficient in other diseases than MCAS. The withdrawal of symptoms should be complete or at least major, as self‑reported by patients.7
In the case of nonsevere, transient symptoms (criterion 1 not fulfilled) and positive criteria 2 and 3, systemic or local (if the range of skin symptoms is limited) mast cell activation (MCA) is diagnosed with a similar clinical approach to that in MCAS.2 In other cases, if the patient does not respond to standard MCAS treatment and requires repeated epinephrine administration, MCA might be diagnosed provided that typical symptoms (criterion 1) and elevated levels of MC‑derived mediator (criterion 2) are present and the criteria for primary MCAS are met (see below).6
Once the diagnosis is confirmed, MCAS is classified according to an underlying cause. Primary MCAS involves monoclonal MC proliferation, similar to SM but not fulfilling its criteria. In this type of MCAS, CD25+ mastocytes, the KIT D816V mutation, or both are observed in bone marrow biopsy. The diagnosis of mastocytosis is superior to that of MCAS, which means that if at any point the criteria for mastocytosis are fulfilled, MCAS is no longer considered. Secondary MCAS is defined as MC activation due to comorbidities.8 The most typical cause is type 1 hypersensitivity according to the Gell and Coombs classification, which leads to persistent MC activation through allergen‑specific IgE.9 Hymenoptera venom, food, and drug intolerance or allergies are currently discussed as the most important causes of secondary MCAS. Although receptors for IgE (FcεRI) are considered the strongest MC activator, many different receptors are present on cell surface.10 Bacterial components might activate MC directly with toll‑like receptors 2, 3, 4, and 6 as well as fMLP receptor or through complement activation.11 Excess of hormones may also induce secondary MCAS through estrogen, progesterone, corticotropin‑releasing hormone, and α-melanocyte–stimulating hormone receptors. The chronic use of certain drugs such as opioids, muscle relaxants, intravenous contrast media, or adenosine may also activate MCs. If the primary and secondary causes are excluded, idiopathic MCAS may be diagnosed.9
Importantly, some patients may be diagnosed with primary and secondary MCAS, as is the case in patients with mastocytosis and insect venom allergy (IVA) who require specific lifelong immunotherapy.12,13 It is recommended that these patients are provided with lifelong immunotherapy, in addition to antimediator treatment and an emergency kit including at least 2 epinephrine autoinjectors.14
When to consider mast cell activation syndrome?
The incidence of recurrent anaphylactic reactions is typical of patients with MCAS.15 If those reactions are associated with hypotension with cardiovascular collapse without skin lesions such as urticaria or angioedema, the probability of MCAS diagnosis is even higher.16,17 In the case of acute symptoms, such as anaphylaxis, it is imperative to stabilize the patient’s condition before starting any diagnostic procedures.
The diagnostic workup in MCAS usually starts from the examination of symptoms (such as anaphylaxis and pruritus); therefore, the diagnostic algorithm should overlap that for anaphylaxis (Figure 1). So far, no diagnostic indications other than those for SM have been proposed for MCAS.2 However, if SM is suspected, primary MCAS should always be considered. According to these algorithms, MCAS should be suspected in the following scenarios:
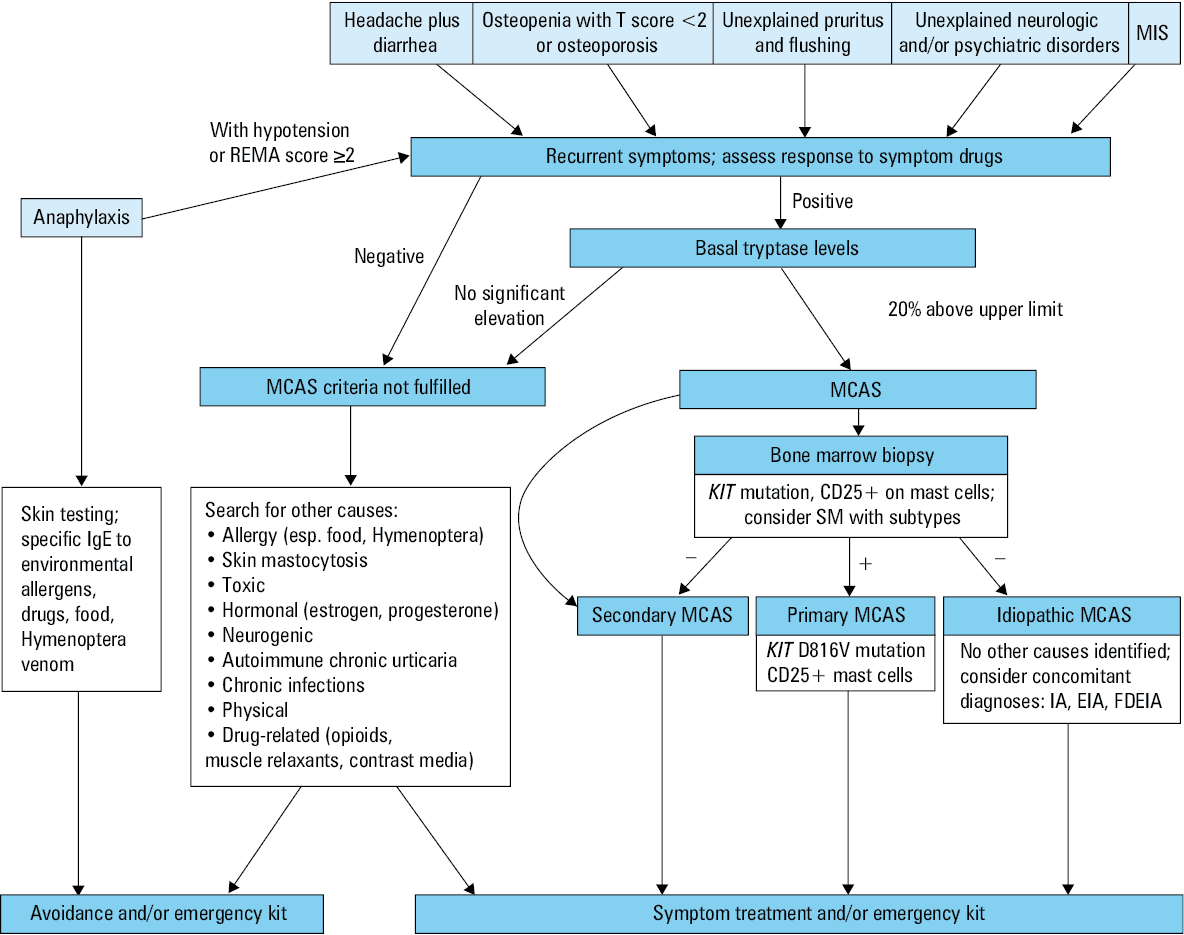
1 In all patients who have experienced anaphylaxis with hypotension, and particularly in those with Hymenoptera venom allergy (HVA) and idiopathic anaphylaxis.
2 In the case of severe osteopenia (T score <2) or osteoporosis in men and in premenopausal women.
3 In patients with recurrent headaches and diarrhea, especially after exclusion of all gastrointestinal disorders and food allergies or intolerance with no lesions on endoscopy.
4 In patients with unexplained pruritus and flushing; in this group, cutaneous mastocytosis (CM) and chronic urticaria should be considered, although these conditions may also coexist with MCAS.
5 In the case of unexplained neurologic and psychiatric disorders with negative screening for any neurologic and endocrine disease.
6 In patients with confirmed mastocytosis in the skin (MIS).
7 In patients who experienced anaphylaxis, with the REMA (Red Española de Mastocitosis) score of at least 2. The points are scored for male sex, lack of skin manifestation, fainting, and high tryptase levels. This score is generally used to decide on patient eligibility for bone marrow biopsy.18
The diagnostic algorithm, initially proposed by Valent et al,2,19 is presented in Figure 1. After the diagnosis of MCAS, consider bone marrow biopsy.
Symptoms of the activation and release of mediators from MCs (MCA) may result from the immune response or a specific IgE‑independent mechanism of hypersensitivity.9 The severity of MCA depends on the trigger, the type of reaction including an IgE‑mediated mechanism, and other chronic disorders.
Anaphylactic reactions occur in 0.05% to 2% of the general population, with more episodes observed in patients with mastocytosis: from 22% to 49% in adults and between 6% and 9% in children.13,20 Hymenoptera stings are considered a major cause of anaphylaxis in mastocytosis.4,13,20,21 The incidence of MCAS in patients with HVA was reported to range from 1% to 7.9%.12,20 In the majority of these patients, anaphylactic reactions occur typically without skin involvement such as rash, blistering, or angioedema, but cardiovascular symptoms, such as hypotension, resulting in the loss of consciousness are predominantly observed. Therefore, anaphylactic reactions without skin involvement could be a potential risk factor for MCAS.8,16 Patients with HVA with a cardiovascular manifestation of anaphylaxis as well as those with HVA and increased basal serum tryptase levels should be screened for mastocytosis with bone marrow trephine biopsy.12,20 It is suggested that these patients may have a very low MC burden; therefore, bone marrow examination should be performed in the Reference Center of Excellence for Mastocytosis where appropriate and highly sensitive techniques are used.20
The main diagnostic procedures in patients with a suspected MC disorder include skin examination, measurement of basal serum tryptase levels, and studies for the presence of KIT gene mutations, notably a D816V analysis.
How to exclude mastocytosis in the skin? When to perform skin biopsy?
The term “mastocytosis in the skin” refers to heterogeneous skin lesions that are typical for various forms of CM.7 It is a provisional diagnosis that can be used until SM‑related criteria are checked and the final diagnosis of CM or SM is established. By definition, CM is associated with no involvement of internal organs.7,22 Adults present with SM with or without skin involvement.19,22,23 The most common clinical presentation of MIS in adults is a maculopapular form (MPCM), previously termed “urticaria pigmentosa.”22,23 It has been estimated that approximately 95% of patients with indolent systemic mastocytosis present with MPCM, while around 50% of patients with advanced forms of SM exhibit skin lesions.19,22,24 Therefore, MIS is considered a significant diagnostic indicator of mastocytosis. To exclude MIS, all patients with MC mediator–related symptoms have to be examined by dermatologists and undergo a skin biopsy if CM is suspected.
Maculopapular CM is characterized by small, round, brown, or red monomorphic lesions that usually intensify upon rubbing, exposure to heat, or emotional stress.22 Mechanical irritation of CM manifestations may provoke skin MC degranulation with redness and urticaria on the skin surface. This reaction, called the Darier sign, is highly specific to CM.22,25 In contrast to the Darier sign, dermographism is induced by stroking the nonlesional skin surface. Small monomorphic lesions correspond to a monomorphic variant of MPCM, which is the most typical variant for adult‑onset mastocytosis. Less frequently, adult patients show larger brown or red lesions of different size and shape typical for a polymorphic variant of MPCM.22 Skin lesions may vary in number, shape, elevation, and pigmentation. Patients may have only a few lesions, usually localized on the thigh and trunk. Skin lesions may be visible also at other body sites as disseminated macules, papules, plaques, or nodules. In some patients, skin lesions tend to show confluence or they are accompanied by telangiectasias.22 Rarely, adult patients suffer from diffuse CM (DCM), the most severe form of CM, due to MC infiltration involving almost the entire skin.26,27 It usually occurs at birth or in early infancy and presents with generalized erythema and blistering. In adults, a generalized thickening of the skin with the leather‑grain appearance and the pronounced Darier sign are prominent features of DCM.26 Patients with MIS may experience MC mediator–related symptoms, both systemic and skin specific, such as flushing and pruritus (blistering occurs only in children).7,22
The diagnosis of MIS is established by examining the skin and performing a skin biopsy.22 The number of MCs is increased 4- to 8‑fold in the lesional skin of CM patients (around 40 MCs/mm2).7,22,28 It is recommended to use an antibody against tryptase as a standard immunohistochemical marker or anti‑KIT (CD117) to visualize skin infiltrate by MCs.5,18,24 In uncertain cases, if histologic examination is not conclusive, the presence of the KIT D816V mutation at codon 816 in lesional skin confirms the diagnosis of MIS.7,22
Tryptase and other mediators
The most important first‑line examination in patients with suspected mastocytosis or primary MCAS is the measurement of tryptase levels in peripheral blood.19 In the absence of urticaria pigmentosa, the patient with the tryptase level below 15 ng/ml and no increase during the suspected reaction should be followed. The tryptase level above 25 ng/ml is an indication for bone marrow studies including histopathology, cytology, flow cytometry, and detection of the KIT mutation.19 Patients with the level between 15 and 25 ng/ml and a REMA score of 2 or higher or with the KIT D816V mutation detected in peripheral blood should also undergo bone marrow studies.18
The elevated tryptase level may be related to other comorbidities, including hematologic, nonhematologic reactive, and other disorders.2 Hematologic diseases include chronic leukemia (myeloid, eosinophilic, basophilic), acute basophilic or myeloid leukemia, myelodysplastic syndrome, myeloproliferative neoplasm especially with mutated PDGFR or FGFR genes, and myelomastocytic leukemia.2,29 Nonhematologic reactive conditions with elevated tryptase levels are allergic disorders, mainly exacerbated chronic urticaria, chronic inflammatory diseases, and chronic helminth infection. Other conditions include end‑stage kidney disease and hereditary alpha tryptasemia. Elevated tryptase level can be rarely found in healthy individuals or as a false positive result due to heterophilic antibodies.2 Additional mediators, such as histamine in plasma or urine, histamine metabolites in urine, or prostaglandin metabolites in 24‑hour urine collection, may also be used as indicators of MCA.30 The positive result should be based on an event‑related increase in at least 2 of these mediators or, preferably, at least 50% higher values after the reaction in comparison with the baseline value.2
Importance of gene studies in mast cell activation syndrome
Of the 3 MCAS variants, only the primary one has a clonal somatic genetic aberration. No specific mutations have been found in patients with secondary or idiopathic MCAS. The crucial element in the pathogenesis of primary MCAS is the presence of the somatic activating KIT D816V mutation in exon 17 in peripheral blood or bone marrow MCs.2,6,31 This mutation is observed in more than 80% of adults with SM. Among pediatric patients, mainly with CM, 25% of cases have no mutation, 35% have the KIT D816V (D816I or D816Y) mutation, and 40% have other mutations in genes encoding consituants of the stem cell factor receptor.32
Other genetic changes observed in patients with mastocytosis
The presence of activating KIT mutations is not the only factor determining the variety of clinical manifestations in MC disorders. Other mutations or gene polymorphisms are vital for the regulation of MC proliferation or activation and affect the clinical outcome.33
The severity of anaphylactic reactions might be increased by an activated cascade of intracellular tyrosine kinases: Kit, Lyn, Syk, and Fyn in pathological MCs.4,34 On the other hand, the presence of KIT D816V gene mutations does not significantly affect the course of anaphylactic reactions.
Recent research on the association of gene polymorphism and clinical disease outcome has shown that clinical manifestations of mastocytosis are related to the 1112C/T polymorphism of interleukin (IL)-13 promoter and Q576R polymorphism of the IL‑4 receptor α-chain.35,36 The –1112C/T polymorphism of the IL13 gene increases the risk of SM. Lange et al37 revealed a potential role of polymorphic variants of the IL31 gene in the pathogenesis of mastocytosis. It was shown that the IL31 IVS2+12AA genotype and IVS2+12A allele were far more common in patients with mastocytosis than in controls and were associated with a higher risk of SM. Moreover, the presence of the –2057AA genotype increased the risk of SM in adults.37
Rausz et al33 investigated the IL6R Asp358Ala polymorphism and reported that carriers of the AA genotype had a 2.5‑fold lower risk of mastocytosis than those with the AC or CC genotypes (odds ratio, 0.40; 95% CI, 0.2–0.8; P = 0.008). Górska et al38 revealed an increased expression of the TRAF4 gene in patients with mastocytosis and food hypersensitivity as well as a decreased expression of the B3GAT1 gene in patients with mastocytosis and IVA. Niedoszytko et al39 studied whole‑genome expression and showed that the genetic pathways that lead to cancer development are associated with the risk of anaphylaxis on exposure to insect venom. Patients who did not respond to insect sting presented more abnormalities in gene expression typical for neoplastic diseases.39 Higher expression of TRAF4 due to T‑helper cell type 2 allergic inflammation is in line with another study highlighting the role of the IL13 gene polymorphism in the pathogenesis of mastocytosis and frequent food‑related hypersensitivity reactions in this group of patients.35
Mutations in epigenetic regulator genes in mastocytosis
Abnormalities in the regulation of epigenetic mechanisms of gene expression may affect the pathogenesis of mastocytosis through specific microRNA expression, loss of suppressor gene function, activation of specific oncogenes (tyrosine kinases, signal transduction proteins), impaired replication and DNA repair processes, and apoptosis as well as by causing instability of the MC genome.40-42 Aberrant expression of microRNAs is detected in MCs with the KIT mutation. Lee et al41 indicated that cells with KIT mutations have lower expression of miR -539 and miR 381. These microRNAs are involved in the inhibition of microphthalmia‑associated transcription factor expression (a regulator of MCs and melanocyte development) as well as melanin and tryptase synthesis (Figure 2).40-42
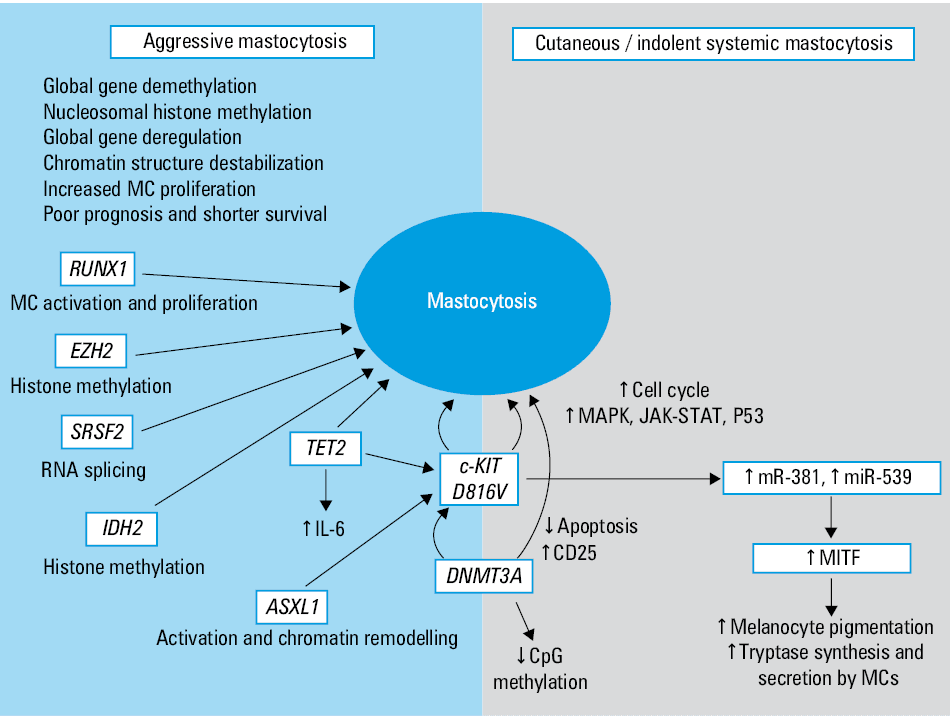
Recent studies using sequencing of multiple genes in search for typical mutations observed in myeloid malignancies have also reported a list of somatic mutations frequently found in patients with mastocytosis.43-47 These included genes encoding factors regulating splicing process, signaling transmission, and epigenetic regulations. Mutations in genes encoding factors involved in the epigenetic process are frequently observed in a clinically advanced form of mastocytosis and are associated with poor prognosis and shorter life expectancy. The most frequently mutated genes are TET‑2 (demethylation of DNA), DNMT3A (methylation of CpG islands), ASXL1 (chromatin silencing and remodeling), and IDH2 (regulation of histone methylation). The main genetic mutations and epigenetic changes observed in mastocytosis are shown in Figure 2.43-47
Management of patients with mast cell activation syndrome and Hymenoptera venom allergy
The aim of chronic treatment is to prevent symptoms by prophylactic use of antimediator drugs.5 The first‑line choice is histamine receptor blockers 1 and 2. Patients with gastrointestinal symptoms may benefit from additional treatment with proton pump inhibitors. Some patients also benefit from administration of cromones, low‑dose glucocorticoids, and, in the case of psychological disorders, antidepressants.5,48-50
It is important to prevent any future allergic or hypersensitivity reactions by proper diagnosis and management, including the equipment of epinephrine autoinjector and specific venom immunotherapy in confirmed venom allergy. According to the guidelines, all patients with anaphylaxis after an insect sting in medical history should be screened for IVA and referred for immunotherapy.51 Insect venom allergy is diagnosed on the basis of anaphylactic symptoms as well as by identifying the stinging insect and confirming the specific IgE mechanism of the systemic reaction. According to the recommendations, skin tests and detection of serum‑specific IgE to insect venom should be performed at least 2 weeks after the allergic reaction.52 If the diagnosis is not confirmed, the same procedures should be repeated in a few weeks. In these patients, a higher risk of MCAS was reported.53 On the other hand, in patients with mastocytosis and a history of anaphylaxis after a sting, it is difficult to confirm the diagnosis on the basis of standard procedures.54 Negative skin test results and undetectable sIgE may be observed in these cases, presumably because of the absorption of sIgE on the surface of MCs.13 In these patients, the detection of sIgE against recombinant allergens or molecular diagnostic approaches such as basophil activation test may improve diagnostic accuracy and enable a diagnosis of IVA.
The recommended therapy in patients with IVA is the same regardless of the presence of MCAS. Apart from antihistamine treatment, all patients without contraindications are referred for immunotherapy and should be equipped with an emergency kit including epinephrine autoinjector. Importantly, according to the current guidelines, venom immunotherapy should be lifelong as the only disease‑modifying treatment in patients with mastocytosis or MCAS. Based on evidence from a large database, it is suggested that the induction of venom immunotherapy with modified, less aggressive, build‑up phase protocol due to some side effects should be performed, which tended to be insignificantly higher during observed rush‑modified course.14 In another study, no adverse reaction was observed during the maintenance treatment and none of the patients discontinued insect venom immunotherapy due to side effects.55 The frequency of adverse events in patients with MCAS is approximately 18.9% (range, 0%–46%) and is similar to that observed in the general population.12,13 However, patients with MC disorders are still at risk of anaphylaxis and a systemic reaction after an insect sting with venom other than that used for immunotherapy.56 Therefore, all patients with MC disorders should be equipped with epinephrine autoinjectors even though they had received maintenance venom immunotherapy.56
- Elieh Ali Komi D, Wohrl S, Bielory L. Mast cell biology at molecular level: a comprehensive review. Clin Rev Allergy Immunol. 2019. . | Crossref
- Valent P, Akin C, Bonadonna P, et al. Proposed diagnostic algorithm for patients with suspected mast cell activation syndrome. J Allergy Clin Immunol Pract. 2019; 7: 1125‑1133.e1. | Crossref
- Shimbori C, Upagupta C, Bellaye P‑S, et al. Mechanical stress‑induced mast cell degranulation activates TGF‑beta1 signalling pathway in pulmonary fibrosis. Thorax. 2019; 74: 455‑465. | Crossref
- Gorska A, Niedoszytko M, Lange M, et al. Risk factors for anaphylaxis in patients with mastocytosis. Pol Arch Med Wewn. 2015; 125: 46‑53. | Crossref
- Valent P, Akin C, Gleixner K V, et al. Multidisciplinary challenges in mastocytosis and how to address with personalized medicine approaches. Int J Mol Sci. 2019; 20: 2976. | Crossref
ARTICLE INFORMATION