The management of patients with atrial fibrillation (AF) has improved in the last decade after the introduction of direct oral anticoagulants (DOACs), which enlarged therapeutic options for thromboprophylaxis in this patient population. Thus, DOACs showed at least similar efficacy to warfarin, with a safer profile regarding major hemorrhages, in particular intracranial bleeding. However, a large proportion of patients with AF is still not receiving an appropriate oral anticoagulation (OAC), with residual thrombotic risk.
In addition, there are some complications not strictly related to AF that are not, or only partially, preventable by OAC, such as cardiovascular death attributed to heart failure and death due to noncardiovascular causes.1 The reported incidence rate of death in patients with AF is up to 5.5% per year,2,3 with approximately 7 in 10 deaths related to cardiovascular causes.
It is therefore evident that to reduce the burden of cardiovascular complications, the management of patients with AF should not be limited to the appropriate prescription of OAC but should include a proactive holistic approach to cardiovascular risk factors and comorbidities. However, a structured clinical approach has been only recently proposed4 and indicated by CHEST guidelines as an appropriate way to manage AF patients.5
This approach, namely the Atrial fibrillation Better Care (ABC) pathway6 (Figure 1), includes 3 components: A stands for avoid stroke with anticoagulation, B, for better symptom management, and C refers to cardiovascular and other comorbidity risk optimization.
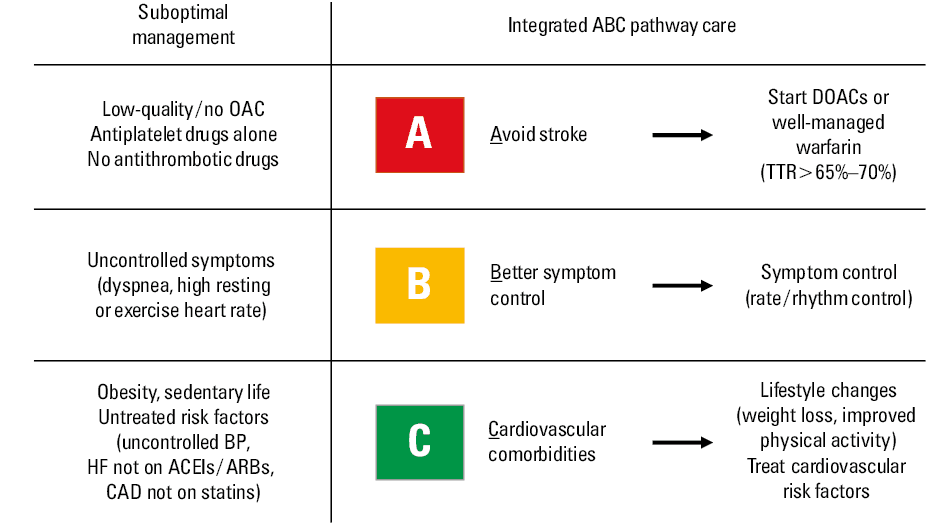
The A component means the optimization of stroke prevention with OAC. In patients treated with warfarin this component consists of maintaining a stable high quality of anticoagulation, as assessed by the time in therapeutic range at values higher than 65% to 70%.7,8 In patients treated with DOACs, the optimization of OAC is represented by the prescription of the appropriate dosage of a DOAC based on patient characteristics. The second component of the ABC pathway, B, implies the need for assessing the presence of symptoms related to AF. The simple European Heart Rhythm Association score may be used for this purpose. The assessment of AF‑related symptoms may help decisions regarding rate and rhythm control. The last component, C, includes a proactive management of associated lifestyle risk factors (ie, unhealthy diet and low physical activity) management and control of cardiometabolic risk factors.
The recently published analysis by Kozieł et al9 on patients included in the BALKAN‑AF survey provides interesting insights on trends in the management of AF patients in the East Europe. As correctly stated by the authors, patients from this region were underrepresented in clinical trials. According to the ABC pathway, less than 50% of patients were optimally treated. Predictors of adherence to the ABC management were: living in the capital city (odds ratio [OR], 1.23; 95% CI, 1.03–1.46; P = 0.02), treatment by cardiologist (OR, 1.34; 95% CI, 1.08–1.66; P = 0.01), arterial hypertension (OR, 2.2; 95% CI, 1.74–2.77; P <0.001), diabetes mellitus (OR, 1.28; 95% CI, 1.05–1.57; P = 0.01), and multimorbidity (≥2 conditions) (OR, 1.85; 95% CI, 1.43–2.38; P <0.001). Conversely, older age (≥80 years) (OR, 0.61; 95% CI, 0.48–0.76; P <0.001) and history of bleeding (OR, 0.5; 95% CI, 0.33–0.75; P = 0.001) were associated with lower adherence to the ABC pathway.9
After analyzing in more detail some aspects of the results from the present study, it becomes evident that the use of OAC is still low; thus even in patients with an indication to OAC (ie, CHA2DS2-VASc ≥2) the authors reported a prevalence of OAC use of 59.9%, with a still high use of antiplatelet drugs and 8.5% of patients not receiving any antithrombotic treatment.9 In the OAC group, at the time of the survey, the use of DOACs was still very low. This low rate of anticoagulation may be due to several reasons, including difficult access to healthcare services in noncapital cities and high cost of DOAC treatment compared with standard warfarin. Furthermore, as also happens in other countries, prescription of DOACs may be reserved to specific specialties (ie, cardiology and internal medicine) or regulated by specific rules, which hinders the increase in DOAC use. However, in keeping with a previous study,10 referral to a cardiology specialist, compared with primary care setting, was associated with an increased rate of OAC prescription. This finding, together with evidence suggesting that the most common reason for not receiving OAC is the physician’s preference, emphasizes the role of medical doctors in the optimization of thromboprophylaxis.11
The study also revealed the suboptimal management of AF in elderly patients, such as those aged 80 years or older.9 This is concerning because elderly patients represent a high‑risk subgroup in whom the risk of stroke and cardiovascular events is particularly evident. In addition, DOACs seem to be effective and safe also in elderly patients, being a suitable therapeutic option for these patients, avoiding the need to assess international normalized ratio.12
The management of comorbidities may be particularly challenging in the AF population, considering that these patients usually have a high number of cardiometabolic diseases, such as metabolic syndrome and heart failure. The BALKAN‑AF study showed a suboptimal management of comorbidities in patients with AF. For instance, more than 30% of patients with heart failure were not receiving a therapy including an ACE inhibitor or angiotensin receptor blocker, and more than 30% of patients with prevalent coronary artery disease not receiving statin therapy.
The implementation of the ABC pathway has prognostic implications. Thus, recent observations from a post‑hoc analysis from the AFFIRM (Atrial Fibrillation Follow‑up Investigation of Rhythm Management) study,13 from the real‑life ATHERO‑AF (Atherosclerosis in Atrial Fibrillation) study cohort14 and from the database of the National Health Insurance Sharing Service in South Korea,15 showed a reduced rate of different complications in patients adherent to the ABC pathway. A clear advantage of this approach relies on including modifiable risk factors, such as anticoagulation quality, blood pressure control, and AF‑related symptoms, which would therefore allow us to modify the individual risk of patients over time.
In conclusion, patients with AF are still not optimally managed; the advantages of appropriate anticoagulation may be lost if other comorbidities are not well addressed leaving patients with a residual cardiovascular risk. A structured integrated management of patients with AF (ie, ABC pathway) should be implemented.
- Gomez‑Outes A, Lagunar‑Ruiz J, Terleira‑Fernandez AI, et al. Causes of death in anticoagulated patients with atrial fibrillation. J Am Coll Cardiol. 2016; 68: 2508‑2521. | Crossref
- Fauchier L, Villejoubert O, Clementy N, et al. Causes of death and influencing factors in patients with atrial fibrillation. Am J Med. 2016; 129: 1278‑1287. | Crossref
- Pastori D, Antonucci E, Violi F, et al. Thrombocytopenia and mortality risk in patients with atrial fibrillation: an analysis from the START registry. J Am Heart Assoc. 2019; 8: e012596.
- Kotecha D, Breithardt G, Camm AJ, et al. Integrating new approaches to atrial fibrillation management: the 6th AFNET/EHRA Consensus Conference. Europace. 2018; 20: 395‑407.
- Lip GYH, Banerjee A, Boriani G, et al. Antithrombotic therapy for atrial fibrillation: CHEST guideline and expert panel report. Chest. 2018; 154: 1121‑1201. | Crossref
ARTICLE INFORMATION