A 63‑year‑old man presented with cough, dyspnea, and fever (38ºC). His respiratory rate was 20 breaths/min and arterial oxygen saturation was 91% on room air. Past medical history included diabetes mellitus, hyperlipidemia, and hepatitis B infection. He was admitted to the intensive care unit but not intubated.
Chest X‑ray performed on admission showed mild nonspecific increased bronchovascular markings with no consolidation (Figure 1A).
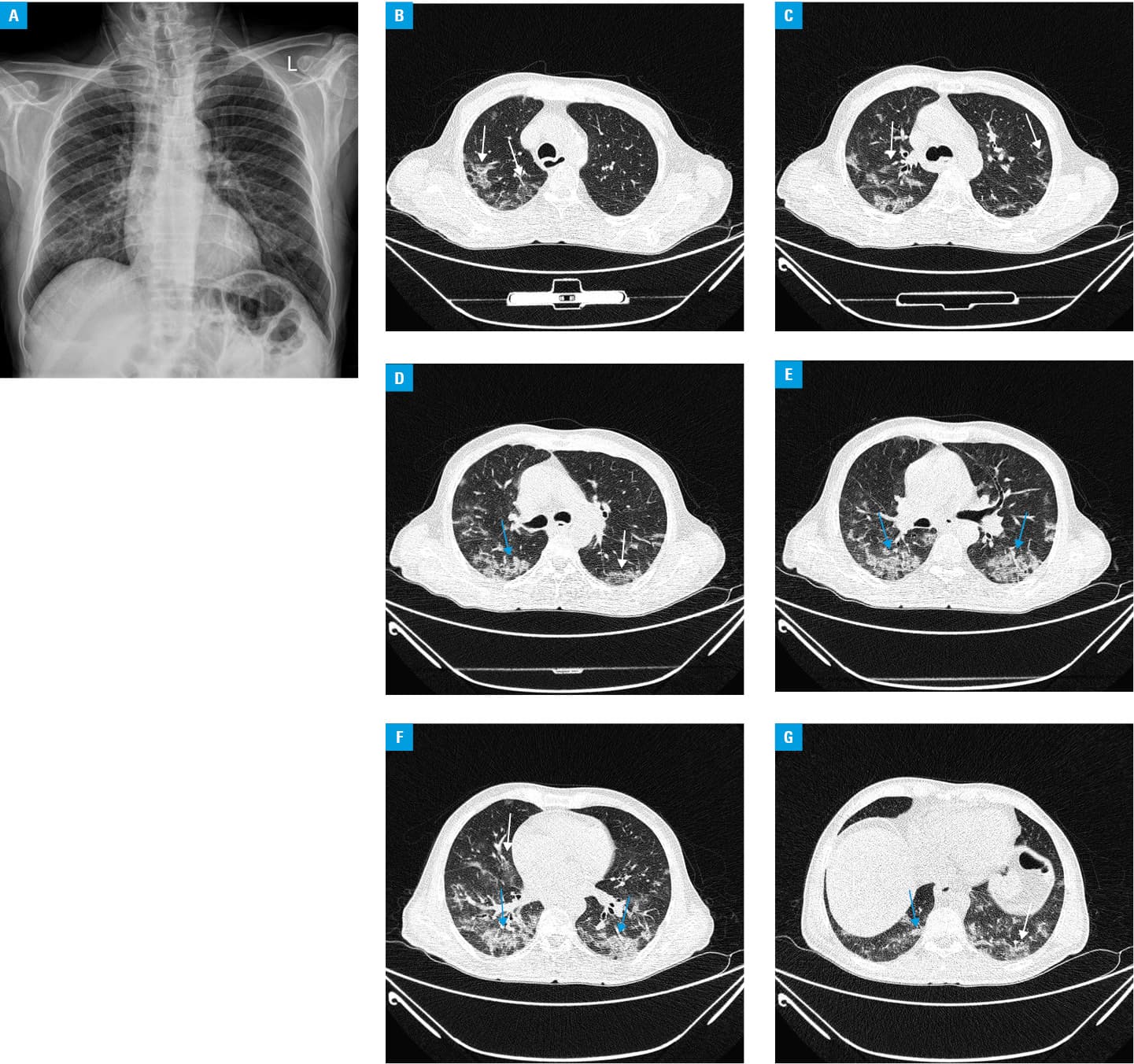
Because the patient’s oxygen saturation was decreasing, computed tomography (CT) was performed (Figure 1B-1G). The lung parenchyma was inhomogeneous with bilateral patchy ground glass opacities along with areas of consolidations. The abnormalities had a peripheral distribution and were more extensive in the lower lobes. There was no pleural effusion or lymphadenopathy.
The diagnosis of coronavirus disease 2019 (COVID‑19) pulmonary infection was established. The patient was treated with oseltamivir, ritonavir, hydroxychloroquine, and vancomycin.
The hospitalization lasted 15 days and the patient was discharged in stable condition with oxygen saturation of 95%.
The important common features of COVID‑19‑induced pulmonary lesions on CT of the thorax include, in the early till late stages, the following 3 key abnormalities1: 1) ground glass opacities with peripheral distribution, 2) consolidations with peripheral distribution, 3) multifocal/multilobar involvement.
Late findings of COVID‑19 include: 1) linear opacities, 2) crazy‑paving (used to describe ground‑glass opacities with superimposed interlobular and intralobular septal thickening), 3) reverse halo.
Additional inconsistent findings in COVID‑19 infections are2: 1) tree‑in‑bud nodularity, 2) centrilobular distribution, 3) predominantly peribronchovascular pattern of distribution, 4) predominantly nodular pattern, 5) cavitation, 6) lymphadenopathy, 7) pleural effusion.
Patients who are at a higher risk for severe illness caused by COVID19 are older adults (>65 years), patients with underlying HIV, asthma, and possibly pregnant women.3
The most important criteria for COVID‑19 severity are respiratory distress (respiratory rates ≥30, arterial oxygen saturation <93% at rest, ratio of partial pressure arterial oxygen to fraction of inspired oxygen [PaO2/FiO2] ≤300 mm Hg), and rapid (within 24–48 hours) progression (>50%) of CT findings. Disease progression can lead to respiratory failure, shock, and extra pulmonary organ failure.4
To summarize, CT of the thorax is sensitive enough to detect the viral infection (COVID‑19) but should not be used as a screening tool in asymptomatic patients. Computed tomography is important to differentiate and rule out other chest findings which may mimic COVID‑19 and plays a vital role in the monitoring of disease progression.
- Mahdavi A, Khalili N, Davarpanah AH, et al. Radiologic management of COVID‑19: preliminary experience of the Iranian Society of Radiology COVID‑19 consultant group (ISRCC). Iran J Radiol. 2020 Mar 7. . | Crossref
- Kanne JP, Little BP, Chung JH, et al. Essentials for radiologists on COVID‑19: an update‑radiology scientific expert panel. Radiology. 2020: 200527. .
- Centers for disease control and prevention. People Who Are at Higher Risk for Severe Illness. https://www.cdc.gov/coronavirus/2019‑ncov/specific‑groups/people‑at‑higher‑risk.html. Accessed March 23, 2020.
- Zu ZY, Jiang MD, Xu PP, et al. Coronavirus Disease 2019 (COVID‑19): a prospective from China. Radiology. 2020 Feb 21. .
ARTICLE INFORMATION