Gastric balloon microbiota: the first investigation of the existence of microbes on the balloon surface



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Gastric balloon microbiota: the first investigation of the existence of microbes on the balloon surface
Introduction
The balloon inserted into the stomach for many weeks seems to be the promised land for bacteria; however, scientific reports describing the phenomenon of colonization of gastric balloon microbiota are not available. Historically, the human stomach has been considered an inhospitable environment for microorganisms because of its acidic conditions and the presence of other antimicrobials.1 However, studies carried out in the mid‑2000s showed that the stomach is rich in various bacterial species. Next generation sequencing analyses demonstrated that as many as 260 phylotypes gathered into 13 phyla are inhabitants of the human gastric mucosa. These predominantly include Proteobacteria (including Helicobacter pylori species and Haemophilus, Actinobacillus, and Neisseria genera), Firmicutes (Streptococcus and Bacillus genera), Bacteroidetes (Prevotella genus), and Actinobacteria (Rothia, Actinomyces and Micrococcus).1
Gastric balloon implantation is a routine procedure performed in overweight and obese patients. The efficacy of the intervention in weight reduction and a relatively low number of complications after surgery have been reported.2 However, few studies aimed to look for a link between gastric microbiota and the efficacy of gastric balloon insertion. To the best of our knowledge, there has been no published report on gastric balloon biofilm microbiota.
For the first time, we have done a preliminary examination of gastric balloon’s microbiota composition in 2 patients after balloon implantation with different tolerance of that treatment.
Patients and methods
Patient A
Patient A, a 51‑year‑old woman, had severe gastric symptoms after balloon implantation (stomach pain, heartburn, nausea) from the very beginning. As a result, she was started on proton pump inhibitors (PPIs; 2 × 40 mg/d throughout the entire treatment period). Due to the above complaints, patient A had the implant removed much earlier, that is, 4 months before the planned time (planned time was 12 months, but the balloon was removed after 8 months). Her weight reduction was not satisfactory (she reduced only 8 kg during therapy), and after the balloon removal, body mass index (BMI) was still too high (initial BMI was 29 kg/m2, and final 26 kg/m2).
Patient B
Patient B, a 28‑year‑old woman, did not experience any adverse effects during therapy, except mild stomach pain. Gastric balloon was used as intended for 6 months. She obtained an almost standard reduction in body weight (18 kg) reaching almost normal BMI (initial BMI was 31.4 kg/m2, and final 25.4 kg/m2). She declared using no drugs throughout the study.
Gastric biopsy samples
The project was approved by the Bioethical Committee of Pomeranian Medical University (no. KB‑0012/29/19). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from both participants included in the study. The patients were qualified for the bariatric procedure during the initial visit, after consultation with the attending doctor. Patients were prepared for the intragastric balloon treatment with the OrberaTM system (Apollo Endosurgery Inc., Austin, Texas, United States) using the standard gastroscopy protocol, after endoscopic analysis of the esophagus and stomach. The endoscopic cytology brush (Cook Medical ECB 5‑180‑2‑S, Jiangsu, China) was used to collect cells from the gastrointestinal wall. The material from the balloon surface was taken and protected against contamination by the gastric, esophageal, and oral cavity wall during the endoscopic device withdrawal maneuver. The material was collected during balloon removal procedures in 2 women at Sonomed Medical Center in Szczecin (Poland). On the day of gastric balloon removal, anthropometric measurements and a standardized food frequency questionnaire were obtained.
Next‑generation sequencing analysis
DNA extraction and sequencing of the V1–V2 regions of the 16S r DNA gene on Illumina MiSeq (Illumina Inc, San Diego, California, United States) were performed in Institute of Clinical Molecular Biology in Kiel University (Germany) using their in‑house protocol. Raw data were processed using the LotuS pipeline (version 1.62, Lotus Software, Massachusetts, United States).3 For taxonomic annotation of operational taxonomic units (OTUs), sequences were aligned against the SILVA4 16S rDNA database using the BLAST+.5 Rarefaction of the OTU abundance table and alpha diversity measures calculations (Chao1 richness estimator, observed species, Shannon and Simpson indices) were done using the RTK program.6 Samples were rarefied down to 13036 reads per sample. Median values of alpha diversity values from 10 rarefaction cycles were taken as final diversity measures. The taxonomic composition of the stomach balloon microbiota swabs was analyzed at the phylum and genus levels.
Results
Gastric balloon biofilm microbiota
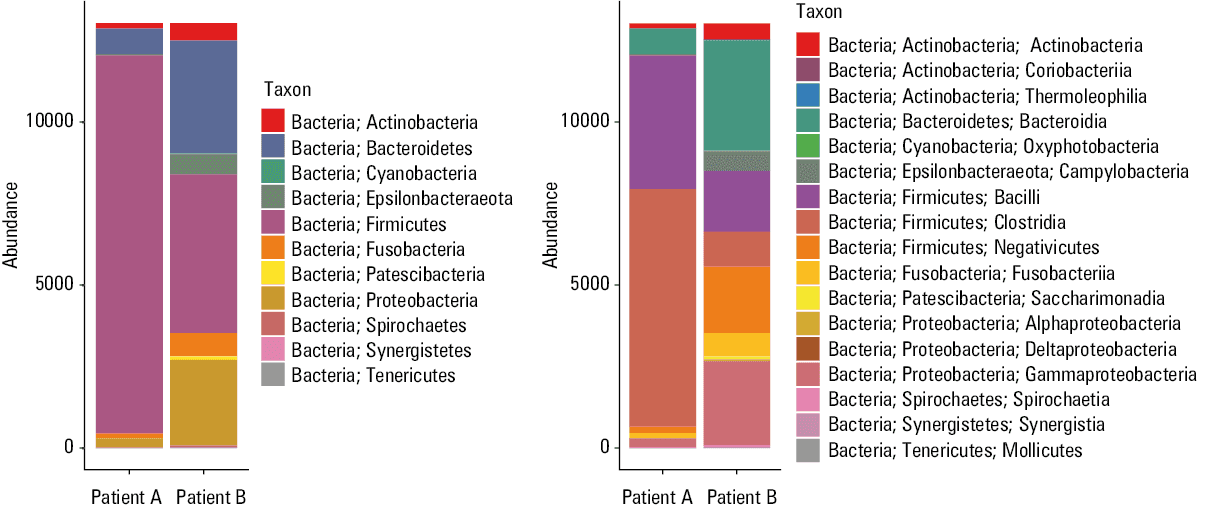
Upon the analysis of the balloon biofilm microbiota from both patients, we observed features common with the gastric mucosa of a healthy person as well as clear differences resulting from the use of PPIs (Patient A). The common phyla of balloon biofilms were similar to that of the healthy human gastric mucosa, and contained: Actinobacteria, Bacteroidetes, Firmicutes, Fusobacteria, Patescibacteria, and Proteobacteria (Figure 1). The gastric balloon microbiota from patient A was less diverse than that in the patient without PPIs, with a marked predominance of Firmicutes and lower abundance of other phyla, for example, Actinobacteria, Bacteroidetes, Epsilonbacteraeota, Fusobacteria, Proteobacteria.
We noticed that as richness and evenness increased, so did the diversity of balloon microbiota species, expressed as OTUs. Balloon microbiota of patient B, as compared with patient A, were characterized by higher richness (OTUs, 144 vs 80, respectively) and evenness (OTUs, 0.72 vs 0.38, respectively). Moreover, alpha diversity indices indicated a higher microbial diversity in patient B. Shannon index was 1.66 vs 3.59, Chao1 88.1 vs 144.3, and Simpson 2.75 vs 19.2 in patients A and B, respectively.
Discussion
In our study, the common bacterial classes of balloon biofilm microbiota were Actinobacteria, Bacteroidia, Campylobacteria, Bacilli, Clostridia, and Negativicutes. In a similar manner, the balloon microbiota of patient A were found to be depleted in taxa such as Bacteroidia and Negativicutes, whereas Bacilli and Clostridia were highly abundant. A previous study among PPIs users7 showed that in the gastric mucosa, the 5 most abundant phyla are: Proteobacteria, Firmicutes, Bacteroidetes, Actinobacteria, and Fusobacteria, with a significant difference between PPI‑users and healthy controls, namely greater abundance of Planococcaceae, Oxalobacteraceae, and Sphingomonadaceae in the PPI group. In contrast, healthy controls showed higher abundance of Caulobacteraceae, and Porphyromonadaceae.
Further, the increase in Clostridia content in patient A seems to confirm the earlier observations showing an increased risk of Clostridium difficile infection after PPIs due to decreased acidity of the gastric lumen.7 It has been shown that microbiota have an important function in the regulation of metabolic pathways related to the metabolism of nutrients in health and disease (eg, type 1 and 2 diabetes).8 It should be emphasized that stomach microbiome composition can also be modified by diet components modulating the secretion of hydrochloric acid—meat and its preservatives as well as vegetable products.1
Conclusions
Significant differences in patient conditions suggest that the balloon microbiota may be an important factor linked with the tolerance and efficacy of the gastric balloon implantation for weight reduction. We would like to emphasize that the balloon microbiome may be possibly influenced by the PPI usage. This indicates that change of the patients’ lifestyle after the bariatric procedure is needed. Additional studies to identify all the factors responsible for balloon tolerance are thus warranted.
- Wu WM, Yang YS, Peng LH. Microbiota in the stomach: new insights. J Dig Dis. 2014; 15: 54‑61. | Crossref
- Alsabah S, Al Haddad E, Ekrouf S, et al. The safety and efficacy of the procedureless intragastric balloon. Surg Obes Relat Dis. 2018; 14: 311‑317. | Crossref
- Hildebrand F, Tadeo R, Voigt AY, et al. LotuS: an efficient and user‑friendly OTU processing pipeline. Microbiome. 2014; 2: 30. | Crossref
- Yilmaz P, Parfrey LW, Yarza P, et al. The SILVA and “All‑species Living Tree Project (LTP)” taxonomic frameworks. Nucleic Acids Res. 2014; 42: D643‑648. | Crossref
- Altschul SF, Gish W, Miller W, et al. Basic local alignment search tool. J Mol Biol. 1990; 215: 403‑410. | Crossref
ARTICLE INFORMATION