Etiology and bacterial susceptibility to antibiotics in patients with recurrent lower urinary tract infections
Key words: antibiotic susceptibility, first-line urinary tract infection treatment, lower urinary tract infections



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Etiology and bacterial susceptibility to antibiotics in patients with recurrent lower urinary tract infections
Introduction: Recurrent urinary tract infections (UTIs) are a frequent health problem and a common reason for treatment resistance.
Objectives: The purpose of the study was to evaluate the etiology of community‑acquired lower recurrent UTI and bacterial antibiotic susceptibility.
Patients and methods: A total of 796 microbiological urine cultures from 332 patients (280 women and 52 men) treated in a single nephrology outpatient department in central Poland in years 2016 to 2018 were analyzed. The most frequent species responsible for recurrent lower UTI were identified and the susceptibility of all the microbes to specific antibiotics was assessed. The patients’ kidney function and inflammation parameters were evaluated.
Results: The median (interquartile range [IQR]) age of the patients was 65 (59–77) years (women, 69 [57–78] years; men, 67 [62–77] years), median (IQR) glomerular filtration rate was 56.6 (40.2–81.3) ml/min/1.73 m2 with median (IQR) C‑reactive protein concentration of 3.2 (1.5–7.0) mg/l. There were 43 bacterial species identified: 24 gram‑positive and 19 gram‑negative. The analyzed urine cultures contained 977 microbial samples (563 gram‑negative bacteria, 408 gram‑positive, 6 fungi). The most common bacteria was Escherichia coli (39.6%) which showed 100% susceptibility to carbapenems, 98.9% to amikacin, 96.5% to piperacillin/tazobactam, and 94.3% to gentamicin. With regard to oral antibiotics, its highest susceptibility was to fosfomycin 95.5%, nitrofurantoin 85.5%, and cefuroxime 82.3%. In 39.9% of cases, E. coli was resistant to fluoroquinolones and in 46.6% to trimethoprim/sulfamethoxazole.Conclusions: The most frequently occurring bacteria causing recurrent lower UTI are characterized by significant resistance to the antimicrobial therapy recommended as the first‑line treatment: fluoroquinolones and trimethoprim/sulfamethoxazole. It seems that the first choice in the treatment of lower UTIs should be: fosfomycin, nitrofurantoin, or cefuroxime.
What's new?
Our study showed that fosfomycin, nitrofurantoin, and cefuroxime should be recommended as the first‑line therapy in community‑acquired lower urinary tract infection (UTI) including recurrent UTI. Bacteria that are the most common causes of lower UTIs are characterized by significant resistance to the most commonly used antimicrobial therapy recommended as the first‑line treatment (ciprofloxacin and trimethoprim/sulfamethoxazole). Based on our findings, it seems reasonable to conduct local analyses of changing etiology and antibiotic susceptibility of microorganisms causing UTIs and to accordingly modify the treatment recommendations.
Introduction
Urinary tract infections (UTIs) are the most common reason for workplace absenteeism and attending general practitioner (GP) appointments.1 There is little statistical data available regarding the frequency of UTIs; however, it is estimated that they are responsible for about 20% of hospital acquired infections and 40% to 50% infections acquired outside the hospital setting.2 Moreover, 20% to 40% of patients with lower UTI experience recurrent infection.3
The etiology of UTIs is predominantly bacterial. They are caused most frequently by Escherichia coli, 70% to 95% of cases, less often by Staphylococcus saprophyticus 5% to 10% of cases, Proteus mirabilis, Klebsiella species (spp.), Enterococcus spp. in 5% or less of cases, and occasionally Staphylococcus aureus.4
The appearance of symptoms of lower UTI such as dysuria, frequent urination, pain in the suprapubic region, or urinary incontinence is a common reason for antimicrobial empiric therapy, which due to various etiology factors of UTIs and constantly increasing resistance of microorganisms, is ineffective in some patients.5,6 In case of an uncomplicated UTI, the following are recommended as the first‑line treatment: nitrofurantoin (it is unavailable in Poland; another available substance is furazidinum), trimethoprim/sulfamethoxazole (cotrimoxazole), trimethoprim, or fosfomycin. Alternatively, if contraindications to the above substances are reported, treatment with an antibiotic belonging to the group of fluoroquinolones is recommended.4
According to the guidelines, in an uncomplicated UTI, it is not necessary to perform microbiological urine examination, therefore information about the etiology, especially about antibiotic susceptibility of bacteria prevalent in specific populations, is relevant in order to choose an antibiotic with the highest probability of effectiveness in the empiric treatment,7 in view of the treatment having become increasingly hindered by growing antibiotic resistance. Resistance to trimethoprim has been reported as higher than 20%. Also resistance to cotrimoxazole is widespread, particularly in developing countries, where it has been reported to be as high as 64%. Identification of resistant urinary isolates is often associated with previous exposure to antibiotics.8
Although the GP’s office is usually the first point of contact for the patients with lower UTI, the majority of microbiological urine examinations are carried out in the nephrology outpatient department, where the patients are referred to for the diagnosis of recurrent UTIs and complicated infections.
The aim of this study was to analyze microbiological urine assessments carried out in patients referred for diagnosis and treatment to a nephrology outpatient department in central Poland from 2016 to 2018, mostly due to recurrent lower UTI, with particular emphasis on the bacteria antibiotic susceptibility.
Patients and methods
Retrospective analysis included all microbiological urine examinations done over 3 years, from 2016 to 2018, in adult Caucasian patients, diagnosed/treated mostly because of recurrent UTIs in one nephrology outpatient department of a university hospital in central Poland. All the samples came from the outpatients presenting with clinical symptoms of lower UTIs. The analysis did not include urine cultures (UCs) from patients with estimated glomerular filtration rate (eGFR) of less than 15 ml/min/1.73 m2, C‑reactive protein (CRP) value higher than 20 mg/l, and those with a Foley‑type catheter. The type of microorganisms and their antibiotic susceptibility were analyzed. As a part of standard diagnostic process of recurrent UTI,s all the patients once underwent an ultrasound examination in the radiology department at the hospital, with the use of the same equipment, but carried out by different radiologists. On the basis of available medical documentation, including anthropometric data, patient’s history and the results of ultrasound examination of the urinary system, UTI was classified as uncomplicated or complicated. Complicated UTI was defined as UTI in a person with urinary tract defect, reflux nephropathy, stasis within the pelvicalyceal system, nephrolithiasis, congenital nephropathy (polycystic kidney disease), or with functional changes in the form of neurogenic bladder. We also took into consideration concomitant disorders such as diabetes mellitus or treatment with immunosuppressive therapy. Information about the serum level of creatinine and CRP values obtained at the same appointment as UCs was taken from the patients’ medical history. The results of UCs were also obtained from medical records. Kidney function was assessed by calculating eGFR using the CKD‑EPI (Chronic Kidney Disease Epidemiology Collaboration) formula.9
The microbiological urine tests were done in the local hospital microbiological laboratory. The inoculations were performed according to the EUCAST (European Committee on Antimicrobial Susceptibility Testing) guidelines.10 Tested specimens were inoculated onto the Columbia agar with 5% sheep blood (bioMérieux, Marcy l’Etoile, France), which supports growth of a variety of bacteria, the MacConkey agar with crystal violet (bioMérieux, Marcy l’Etoile, France), which allows growth of only gram‑negative bacteria, and the Sabouraud gentamicin chloramphenicol 2 agar (bioMérieux, Marcy l’Etoile, France), which allows growth of fungi. The inoculations on the Columbia agar and the MacConkey agar were incubated (CO2‑Incubator, model INC153med, Memmert GmbH, Heilbronn, Germany) at 35 °C for up to 48 hours, whereas the inoculations on the Sabouraud agar were incubated at 35 °C for up to 7 days. Bacterial and yeast species identification was performed using the VITEK®2 Compact (bioMérieux Inc., Hazelwood, Missouri, United States). The following reference strains were tested for quality control: S. aureus the American Type Culture Collection (ATCC) strain 25923, Enterococcus faecalis ATCC 29212, E. coli ATCC 25922 and 35218, Klebsiella pneumoniae ATCC 700603, Pseudomonas aeruginosa ATCC 27853, Candida albicans ATCC 90028, and Candida parapsilosis ATCC 22019. Susceptibility testing was performed using the VITEK®2 Compact with Vitek card YS08 for yeast and Vitek 2 AST‑PG43 and Vitek 2 AST‑N330 for bacteria. The disk diffusion method was used to determine drug susceptibility to antibiotics not included in Vitek cards, for example, fosfomycin, tetracycline, ofloxacin, levofloxacin. Susceptibility to a range of antibiotics was evaluated by the disk diffusion method on the Mueller‑Hinton agar (Bio‑Rad, Marnes‑la‑Coquette, France) for gram‑negative rods, staphylococci, and enterococci, and Mueller‑Hinton agar supplemented with 5% defibrinated horse blood and 20 mg/l NAD (Bio‑Rad, Marnes‑la‑Coquette, France) for streptococci. Minimum inhibitory concentrations were determined by the VITEK®2 Compact and, in addition, by antibiotic gradient strips, Etest (bioMérieux, Marcy l’Etoile, France). In addition, M.I.C.E strips (Oxoid Limited, Hampshire, United Kingdom) were used for extended‑spectrum β-lactamase (ESBL)-producing strains.
For this type of a retrospective study, formal patient consent and the approval of an institutional review board were not required.
Statistical analysis
Nominal data are presented as numbers with percentages; numerical data are presented as medians with interquartile range. Lack of normality was assessed based on visual inspection of histograms. All calculations were done using the Microsoft Excel software.
Results
A total of 796 UCs from 332 patients (280 women and 52 men) were analyzed. Seventy‑five patients had diabetes mellitus, 9 were diagnosed with autoimmune diseases (6 had systemic lupus erythematosus, 3 had rheumatoid arthritis) and were treated with immunosuppressive therapy. Abdominal ultrasound detected nephrolithiasis without any signs of stasis in 41 of the patients; 21 patients were diagnosed with chronic obstructive nephropathy and 10 patients with polycystic kidney disease. Complicated UTIs were diagnosed altogether in 72 patients (21.7%). In other patients, imaging did not show significant deviations from normal, except for single simple cysts. The characteristics of the study group along with the number of UCs and the number of isolated bacteria are presented in Table 1.
Whole group | Women | Men | |
Data are presented as number (percentage) unless otherwise indicated.
Abbreviations: CRP, C‑reactive protein; eGFR, estimated glomerular filtration rate; IQR, interquartile range; UC, urine culture; UTI, urinary tract infection | |||
Patients | 332 (100) | 280 (84.3) | 52 (15.7) |
Age, y, median (IQR) | 65 (59–77) | 69 (57–78) | 67 (62–77) |
Patients with diabetes | 75 (22.6) | 64 (22.9) | 11 (21.2) |
Patients with complicated UTI | 72 (21.7) | 55 (19.6) | 17 (32.7) |
UCs | 796 (100) | 688 (86.4) | 108 (13.6) |
UCs per patient, n, median (IQR) | 1 (1–3) | 1 (1–3) | 1 (1–2.5) |
eGFR, ml/min/1.73m2, median (IQR) | 56.6 (40.2–81.3) | 56.5 (40.1–82.2) | 57.7 (40.2–75.5) |
CRP, mg/l, median (IQR) | 3.2 (1.5–7) | 3.3 (1.4–7) | 3 (1.8–7.1) |
Identified bacterial samples, n | 97 | 845 | 126 |
Gram‑negative bacterial samples, n | 563 | 502 | 61 |
Gram‑positive bacterial samples, n | 408 | 343 | 65 |
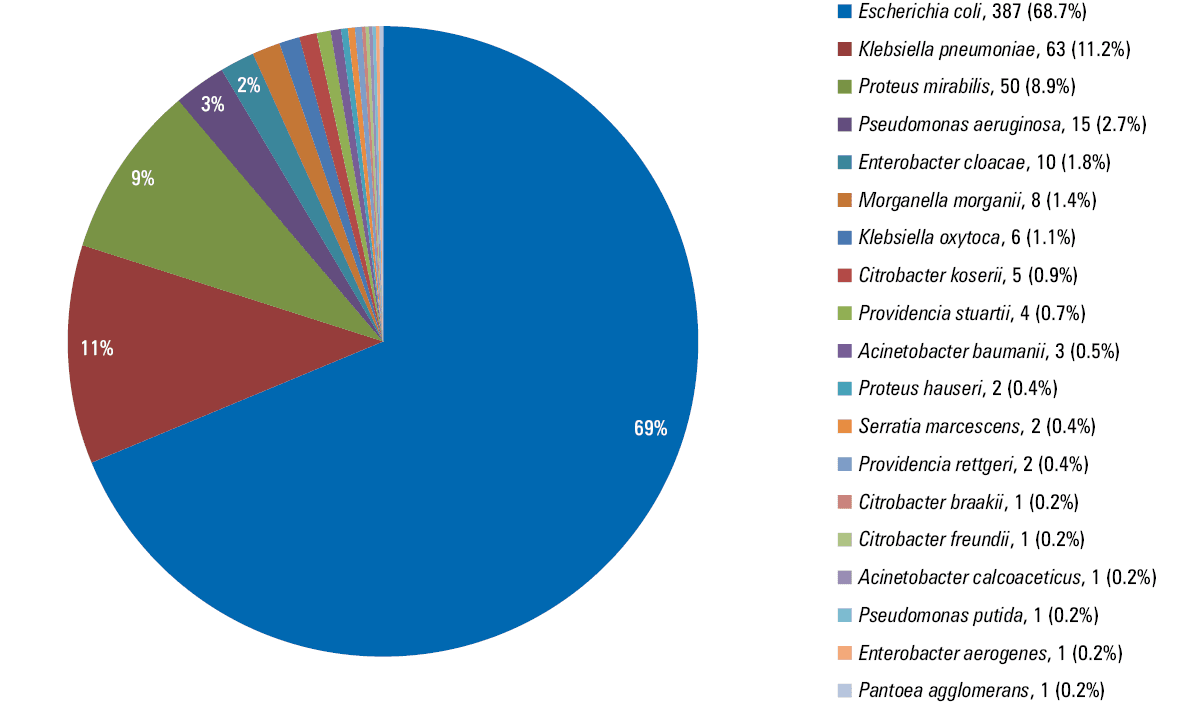
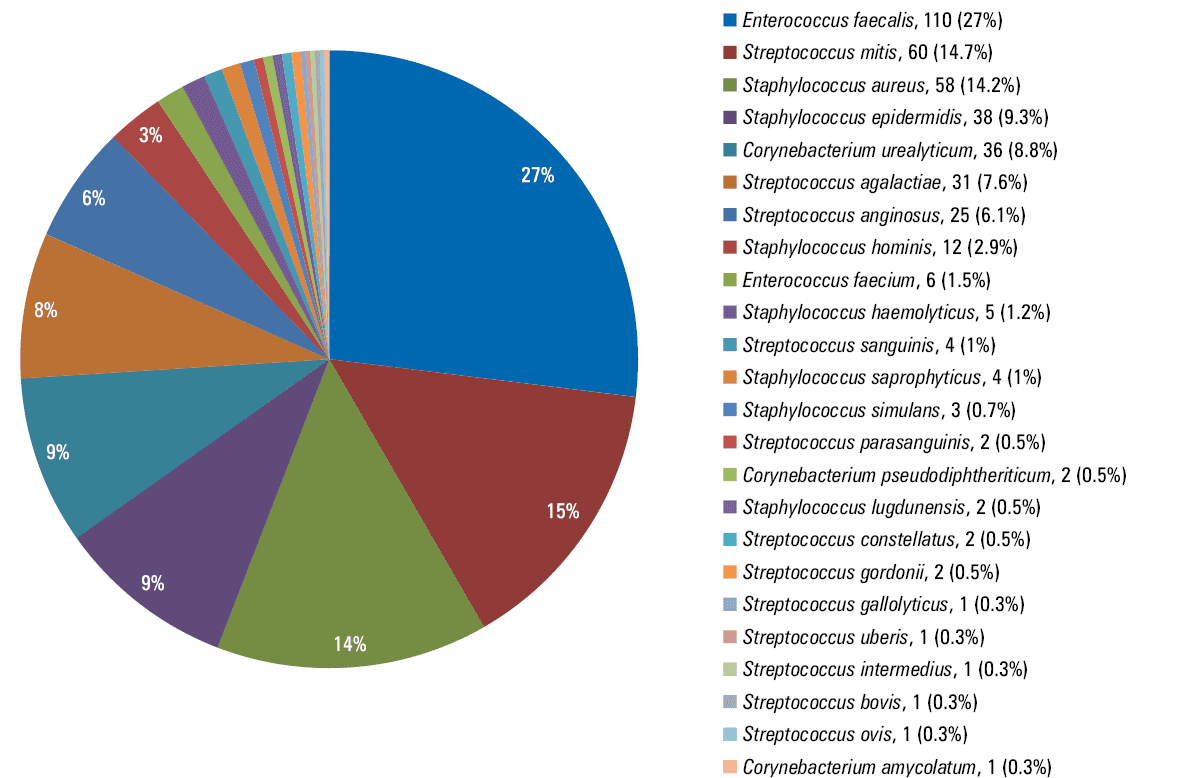
According to all identified microorganisms in the analyzed UCs, infections in the study group were caused most often by bacteria (99.2%) and seldom by fungi (0.4%) or mixed flora (0.4%). Among the bacteria, 58% were gram‑negative and 42% were gram‑positive. The most frequently identified gram‑negative bacteria were: E. coli (39.6% of all microorganisms), K. pneumoniae (6.4%), and P. mirabilis (5.1%). The most frequent gram‑positive bacteria were: E. faecalis (11.3%), Streptococcus mitis (6.1%), and S. aureus (5.9%). The etiology of UTIs in the whole study group and separately in women and in men are illustrated in Table 2.
Bacteria | Samples in whole group | Samples in women | Samples in men |
Data are presented as number (percentage). Percentage was calculated in respect to the number of microbial samples. | |||
Escherichia coli | 387 (39.6) | 359 (42.4) | 28 (21.5) |
Enterococcus faecalis | 110 (11.3) | 94 (11.1) | 16 (12.3) |
Klebsiella pneumoniae | 63 (6.4) | 51 (6) | 12 (9.2) |
Streptococcus mitis | 60 (6.1) | 54 (6.4) | 6 (4.6) |
Staphylococcus aureus | 58 (5.9) | 46 (5.4) | 12 (9.2) |
Proteus mirabilis | 50 (5.1) | 50 (5.9) | 0 |
All identified bacteria in the assessed UCs and the percentage distribution of individual species are depicted in Figures 1 and 2.
Among the identified bacteria, the number of microorganisms belonging to particularly resistant strains was calculated: ESBL‑producing E. coli constituted 9% of all cases of a given species, and respectively: ESBL‑producing K. pneumoniae 30.2%, ESBL‑producing P. mirabilis 6%, high‑level aminoglycoside resistance E. faecalis 28.2%, methicyllin‑resistant S. aureus 24.1%.
The most common bacteria found in UCs from patients with complicated UTI were E. coli (33.6%), E. faecalis (11.4%), and S. aureus (10%).
There were 202 patients (60.8%) aged 65 years and older. Among those, the etiology of recurrent UTIs was similar to that of the entire group; the most frequent microorganisms were E. coli (44.2%), E. faecalis (10.5%), and K. pneumoniae (8.1%).
E. coli, the most frequent gram‑negative bacteria in the study group, presented 100% susceptibility to intravenous antibiotics such as carbapenems, that is, imipenem and meropenem, 98.9% to amikacin, 96.5% to piperacillin with tazobactam, 94.3% to gentamicin. With regard to oral antimicrobial drugs, its highest susceptibility was to fosfomycin 95.5%, nitrofurantoin 85.5%, and cefuroxime 82.3%. In 39.9% of cases, E. coli was resistant to fluoroquinolones and in 46.6% to cotrimoxazole. The most frequently occurring gram‑positive bacteria, E. faecalis, was susceptible to imipenem, linezolid, and vancomycin in 100%, and with regard to oral medications, to ampicillin and amoxicillin in 100%, to nitrofurantoin in 97.3%, and to amoxicillin with clavulanic acid in 80%. E. faecalis was resistant to ciprofloxacin in 93.2%, to cotrimoxazole in 98.9%, and to cefuroxime and gentamicin in 100%.
Antibiotic susceptibility of the most frequent gram‑negative and gram‑positive bacteria causing UTIs is presented in detail in Tables 3 and 4.
Data are presented as percentage unless otherwise indicated.
Abbreviations: ESBL, extended‑spectrum β-lactamases | |||||||||||||||
Bacteria | Total, n | Amikacin | Gentamicin | Amoxicillin/clavulanic acid | Ampicillin | Piperacillin /tazobactam | Cefuroxime | Cefepime | Ciprofloxacin | Fosfomycin | Nitrofurantoin | Imipenem | Meropenem | Cotrimoxazole | |
Escherichia coli | Total | 387 | 98.9 | 94.3 | 70.5 | 44.7 | 96.5 | 82.3 | 90.7 | 60.1 | 95.5 | 85.5 | 100 | 100 | 53.4 |
Non–ESBL producing | 352 | 99.1 | 96.6 | 75.3 | 49.7 | 98.1 | 90.5 | 99.6 | 65.2 | 97.1 | 86.4 | 100 | 100 | 55.5 | |
ESBL producing | 35 | 97.1 | 70.6 | 22.9 | 0 | 82.4 | 0 | 17.9 | 8.6 | 80 | 77.1 | 100 | 100 | 32.4 | |
Klebsiella pneumoniae | Total | 63 | 95.2 | 90.5 | 54 | 0 | 67.2 | 59.7 | 72.2 | 45.2 | 23.8 | 2.3 | 100 | 100 | 50.8 |
Non–ESBL producing | 44 | 97.7 | 95.5 | 75 | 0 | 81 | 86.1 | 100 | 65.1 | 26.2 | 0 | 100 | 100 | 68.2 | |
ESBL producing | 19 | 89.5 | 79 | 5.3 | 0 | 36.9 | 0 | 0 | 0 | 17.7 | 10 | 100 | 100 | 10.5 | |
Proteus mirabilis | Total | 50 | 100 | 67.4 | 88 | 46.9 | 100 | 94 | 92.3 | 50 | 35.9 | 0 | 100 | 100 | 36 |
Non–ESBL producing | 47 | 100 | 72.1 | 93.6 | 51.7 | 100 | 100 | 100 | 53.2 | 36.8 | 0 | 100 | 100 | 38.3 | |
Bacteria | Total, n | Amikacin | Gentamicin | Amoxicillin | Amoxicillin/clavulanic acid | Ampicillin | Piperacillin/tazobactam | Cefuroxime | Ciprofloxacin | Levofloxacin | Nitrofurantoin | Cotrimoxazole | Imipenem | Linezolid | Vancomycin | ||
Data are presented as percentage unless otherwise indicated.
Abbreviations: HLAR, high‑level aminoglycoside resistance; NE, not estimated; MRSA, methicillin‑resistant Staphylococcus aureus; MSSA, methicillin‑sensitive Staphylococcus aureus | |||||||||||||||||
Enterococcus faecalis | Total | 110 | 4.2 | 0 | 100 | 80 | 100 | 100 | 0 | 6.8 | 64.3 | 97.3 | 1.1 | 100 | 100 | 100 | |
Without HLAR | 79 | 5.9 | 0 | 100 | 80 | 100 | 100 | 0 | 8.2 | 77.8 | 100 | 0 | 100 | 100 | 100 | ||
With HLAR | 31 | 0 | 0 | 100 | NE | 100 | 100 | 0 | 3.7 | 40 | 90.3 | 4 | 100 | 100 | 100 | ||
Streptococcus mitis | 60 | NE | 0 | 100 | NE | 96.8 | NE | 98.3 | 0 | 61.7 | 0 | 0 | NE | 100 | 100 | ||
Staphylococcus aureus | Total | 58 | 80 | 82.1 | NE | 75 | NE | NE | 76 | 68.4 | 65.9 | 0 | 58.2 | NE | 100 | 100 | |
MSSA | 44 | 91.3 | 90.7 | NE | 100 | NE | NE | 100 | 86.1 | 81.3 | 0 | 69.1 | NE | 100 | 100 | ||
MRSA | 14 | 42.9 | 53.9 | NE | 0 | NE | NE | 0 | 14.3 | 11.1 | 0 | 23.1 | NE | 100 | 100 | ||
Susceptibility of the most commonly identified bacteria (all cases from each species, including particularly resistant strains) to the most frequently used antibiotics, including those recommended as the first‑line treatment in UTI2 is summarized in Table 5.
Bacteria | Distribution, n (%)a | Amoxicillin | Amoxicillin/clavulanic acid | Cefuroxime | Ciprofloxacin | Fosfomycin | Nitrofurntoin | Cotrimoxazole |
Data are presented as percentage unless otherwise indicated.
a The number of identified samples and their percentage distribution
Abbreviations: see Table 4 | ||||||||
Escherichia coli | 387 (39.6) | NE | 70.5 | 82.3 | 60.1 | 95.5 | 85.5 | 53.4 |
Enterococcus faecalis | 110 (11.3) | 100 | 80 | 0 | 6.8 | NE | 97.3 | 1.1 |
Klebsiella pneumoniae | 63 (6.4) | NE | 54 | 59.7 | 45.2 | 23.7 | 2.3 | 50.8 |
Streptococcus mitis | 60 (6.1) | 100 | NE | 98.3 | 0 | NE | 0 | 0 |
Staphylococcus aureus | 58 (5.9) | NE | 75 | 75.9 | 68.4 | NE | 0 | 58.2 |
Proteus mirabilis | 50 (5.1) | NE | 88 | 94 | 50 | 35.9 | 0 | 36 |
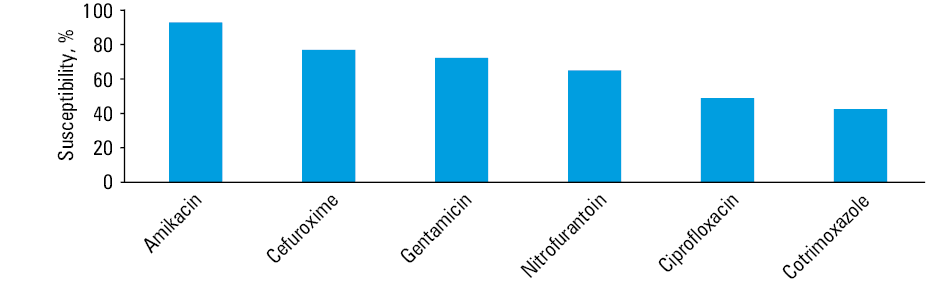
The susceptibility of the most frequent bacteria in the study group (E. coli, K. pneumoniae, P. mirabilis, E. faecalis, S. mitis, S. aureus), constituting 74.5% of all identified microorganisms, is presented in Figure 3.
Discussion
Our research confirmed that lower UTIs are diagnosed much more frequently in women than in men (84.3% women, 15.7% men), and in the elderly.11
The most common pathogen identified in the study population was E. coli, constituting 39.6% of all found bmicroorganisms, which is less common than reported in other studies; however, the analyzed UCs were taken mainly from patients with recurrent UTI. Stefaniuk et al,12 in a multicenter analysis conducted in the Polish population in 2013, found that E. coli was responsible for 71.4% of all UTIs. In a California study, where the etiology of UTIs from 2008 to 2017 was analyzed, E. coli was the cause of UTIs acquired outside hospital in 70%,13 and in a study from Russia, 49.1%.14 Other identified bacteria in our population were E. faecalis (11.3%), K. pneumoniae (6.4%), S. mitis (6.1%), S. aureus (5.9%), and P. mirabilis (5.1%), which are also mentioned in other reports as common causes of UTIs,15-17 but with variable frequency. The percentage distribution of the most frequent microorganisms causing UTIs differs depending on the study population; however, in all studies, a significant numerical superiority of gram‑negative over gram‑positive species is emphasized.12,16
According to the guidelines, in case of an uncomplicated UTI, chemotherapeutics are recommended as the first‑line treatment. These are, for example, nitrofurantoin, cotrimoxazole, trimethoprim, fosfomycin or alternatively fluoroquinolones.4 Our analysis showed that bacteria that are the most common etiological factors of recurrent UTI demonstrate significant resistance to the abovementioned substances, which is also confirmed in other European analyses, for example, in one conducted in Spain,18 and another in Switzerland.19 In our study, E. coli was characterized by as much as 39.9% resistance to ciprofloxacin and 46.6% to trimethoprim/sulfamethoxazole. Both these chemotherapeutics are among substances most frequently prescribed by GPs in the treatment of UTI, including recurrent UTI, not only in Poland.20 A Polish study published in 2016 presents the susceptibility of E. coli to ciprofloxacin in 65.8% and to trimethoprim/sulfamethoxazole in 65.1% of cases.12 In Spain, in years 2003 to 2004, it was shown to be as much as 81.4% and 74.1%21 and in the earlier mentioned studies 73.8%, 76.1%18 and 88.9%, 85.7%,19 respectively. Our results confirm a constantly growing resistance of bacteria to the frequently used chemotherapeutics. Perhaps the higher percentage of resistance to fluoroquinolones noted in our population is due to the fact that the antibiotic susceptibility was assessed several years later than in the cited studies, and most of our population had specifically recurrent UTI, having probably already undergone a course of antibiotic therapy in the past.12,21 Of note, ciprofloxacin, trimethoprim/sulfamethoxazole, amoxicillin, amoxicillin with clavulanic acid and cefuroxime are on the list of the most frequently used antibacterial medications due to different indications including community‑acquired respiratory tract infections in 2014 in Poland.22 It may partly account for such a high resistance of bacteria to this chemotherapeutics causing UTI in our population. Noteworthy in our studied group is high susceptibility of E. coli to fosfomycin 95.5% and nitrofurantoin 85.5%, which is also highlighted in other publications.6,23,24
Such high susceptibility of E. coli to nitrofurantoin in Poland may be due to the fact that the substance is not available and another substance, furazidinum, having similar properties and belonging to the group of nitrofurans, is in common use. However, a study performed in Switzerland in years 2009 to 2015 also revealed significant effectiveness of nitrofurantoin in the treatment of lower UTI, including recurrent UTI, although this substance is available and often prescribed by GPs.25
Despite high susceptibility of E. coli to nitrofurantoin and fosfomycin, these substances present low efficacy against other pathogens, especially gram‑positive bacteria, which cause UTIs (they were the cause of UTIs in our population in 42% of cases). In our study, most frequent gram‑positive bacteria (S. mitis, S. aureus, with exception of E. faecalis, which showed 97.3% susceptibility) were resistant to nitrofurantoin in every case, while resistance to fosfomycin was not estimated at all. Cefuroxime, an antibiotic available in oral form, proved to be highly effective both against gram‑negative and gram‑positive bacteria. However, it is not on the list of substances recommended as the first‑line treatment in uncomplicated UTI. Its effectiveness against 6 of the most frequent bacterial species (constituting 74.5% of all identified bacteria) was estimated as 77%. E. coli showed 82.3% susceptibility to cefuroxime in our analysis and 90.1% in another study.12
After analyzing all our microbiological UCs, high susceptibility of microorganisms to intravenous antibiotics was observed. E. coli showed 100% susceptibility to carbapenems (imipenem and meropenem), 98.9% to amikacin, 96.5% to piperacillin with tazobactam and 94.3% to gentamicin, and E. faecalis showed 100% susceptibility to ampicillin, imipenem, linezolid, and vancomycin. However, it is likely that such high susceptibility of bacteria causing recurrent lower UTI may be due to the fact that in such infections intravenous antibiotic therapy is practically not used and reserved for more severe systemic infections, and oral treatment is preferred. The high susceptibility of pathogens to aminoglycosides should be emphasized. It may result from the fact that due to their nephrotoxicity, it is currently a very rarely recommended class of drugs.
Another issue mentioned in many studies26-29 is a growing prevalence of pathogens belonging to particularly resistant strains, which renders effective antibiotic therapy of UTI very difficult. As suggested in a study published in 2019, potential risk factors of infection with ESBL‑producing strains may be: antibiotic therapy or previous hospitalization during the last 3 months, history of recurrent UTIs, or abnormalities in the structure and functioning of the kidneys.30 In the analyzed UCs, ESBL‑producing E. coli represented 9% of all cases of a given species, ESBL‑producing K. pneumoniae 30.2%, ESBL‑producing P. mirabilis 6%. ESBL‑producing E. coli showed lower susceptibility to nitrofurantoin (77.1%) and fosfomycin (80%) compared with non–ESBL‑producing (86.4% and 97.1%, respectively). ESBL‑producing K. pneumoniae was sensitive to nitrofurantoin only in 10% of cases and to fosfomycin in 17.7%. That is not compatible with the results from a study from England in years 2015 to 2017, where over 95% of ESBL‑producing Enterobacteriaceae were susceptible to nitrofurantoin and fosfomycin.26 In another study published in 2019, no significant difference was observed in the treatment of UTI caused by ESBL‑producing pathogens with antibiotics from the carbapenem group or other groups;27 however, in our analysis, those microorganisms showed 100% susceptibility especially to carbapenems (imipenem and meropenem). These bacteria were susceptible to an old antibiotic, amikacin (ESBL‑producing E coli, 97.1%; ESBL‑producing K. pneumoniae, 89.5%), less often they were sensitive to oral preparations, amoxicillin with clavulanic acid (22.9% and 5.3%, respectively), cotrimoxazole (32.4% and 10.5%, respectively) and demonstrated no susceptibility to cefuroxime.
The kidney function in our patients was normal with median (IQR) eGFR of 56.6 (40.2–81.3) ml/min/1.73 m2 and with median CRP value of 3.2 (1.5–7.0) mg/l, slightly exceeding the reference range (<5 mg/l).
Our study has some limitations. First of all, this is a retrospective study and the assessment was carried out based on medical documentation, including the patient’s medical history, laboratory results with UCs, results of imaging examinations, on the basis of which UTIs were qualified as complicated/uncomplicated. We cannot give reliable treatment results since the patients were treated by different nephrologists, and outpatients follow‑up visits were performed at different time schedules, and sometimes patients were recommended to attend a follow‑up at a GP.
In conclusion, the analysis showed that bacteria that are the most common causes of recurrent lower UTIs are characterized by significant resistance to the antimicrobial therapy most commonly used and recommended as the first‑line treatment: fluoroquinolones and trimethoprim/sulfamethoxazole. It seems that the first choice in treatment of lower UTIs should be: fosfomycin, nitrofurantoin, or cefuroxime. It is advisable to conduct local analyses of changing etiology and antibiotic susceptibility of microorganisms causing UTIs and to accordingly modify the recommendations regarding the implementation of empiric treatment depending on the results obtained in a given population.
- Mulder M, Baan E, Verbon A, et al. Trends of prescribing antimicrobial drugs for urinary tract infections in primary care in the Netherlands: a population‑based cohort study. BMJ Open. 2019; 9: e027221. | Crossref
- Kiliś-Pstrusińska K. Urinary tract infections . Praktyka Lekarska: Zeszyty Specjalistyczne. 2012; 72: 5‑13.
- Hooton TM, Stamm WE. Diagnosis and treatment of uncomplicated urinary tract infection. Infect Dis Clin North Am. 1997; 11: 551‑581. | Crossref
- Duława J, Drabczyk R. Urinary tract infections . In Gajewski P, Szczeklik A, eds. Interna Szczeklika ‑ Internal Medicine Textbook 2018 . Medycyna Praktyczna; 2018: 1611‑1622.
- Wagenlehner FM, Naber KG. Treatment of bacterial urinary tract infections: presence and future. Eur Urol. 2006; 49: 235‑244. | Crossref
ARTICLE INFORMATION