Prevalence of atherosclerotic stenosis of the carotid and cerebral arteries in patients with stable or unstable coronary artery disease
Key words: atherosclerosis, carotid, cerebral, coronary artery disease



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Prevalence of atherosclerotic stenosis of the carotid and cerebral arteries in patients with stable or unstable coronary artery disease
Introduction: Carotid artery atherosclerosis is a recognized predictor of cardiovascular events. The coexistence of coronary atherosclerosis and cerebrovascular disease is associated with unfavorable clinical outcomes.
Objectives: The aim of this study was to determine the prevalence of hemodynamically and clinically significant carotid and/or cerebral artery stenosis in patients with stable and unstable coronary artery disease (CAD).
Patients and methods: Cardiac and neurological examinations together with coronary angiography and carotid ultrasound were performed in 241 patients, and transcranial Doppler imaging of cerebral arteries in 114. The prevalence of hemodynamically significant internal carotid artery (ICA) stenosis, intracranial artery stenosis, and clinical signs of central nervous system ischemia were compared between patients with stable and unstable CAD.
Results: There was no significant difference in the prevalence of ICA stenosis (15.3% vs 19%) and intracranial artery stenosis (18% vs 16%) between patients with stable and unstable CAD. Risk factors for cerebral artery stenosis included ICA stenosis (odds ratio [OR], 13.21; 95% CI, 5.93–41.89) and advanced CAD (OR, 2.38; 95% CI, 1.13–4.09), and for ischemic events within the central nervous system, ICA stenosis (OR, 1.74; 95% CI, 1.01–3.16) and intracranial artery stenosis (OR, 3.01; 95% CI, 1.66–5.57).
Conclusions: No differences in the prevalence of atherosclerosis of the carotid and cerebral arteries were found between patients with stable and unstable CAD in this study. Advanced CAD is one of the risk factors for hemodynamically significant cerebral artery stenosis.
What's new?
In this study, the coexistence of carotid or intracranial atherosclerosis with coronary artery disease (CAD) was confirmed in more than 16% of patients. We did not find any significant difference in the prevalence of internal carotid artery and intracranial arterial stenoses between patients with stable CAD and those with the unstable disease. Advanced CAD was a risk factor for the hemodynamically significant stenosis of cerebral arteries. Our findings support a multivessel approach in patients with a single clinical manifestation of atherosclerosis. Knowledge of the site and severity of atherosclerotic lesions is of importance to clinicians who qualify patients for interventional treatment of various vascular areas, as patients with multivessel disease gain fewer benefits. Our findings confirmed that extensive diagnostic procedures performed in patients with advanced CAD, including the examination of intracranial arteries, can help identify those at risk of central nervous system ischemia.
Introduction
Atherosclerosis is a systemic arterial disease; however, the mechanisms underlying the formation, development, and destabilization of concomitant lesions observed in arteries of various calibers and varying reactivity parameters remain unclear.1-3
The involvement of arteries from different vascular areas indicates a significant burden of the atherosclerotic process, even if patients have never experienced any clinical symptoms of atherosclerosis. The coexistence of atherosclerosis in the coronary arteries, carotid arteries, and other vascular territories has been proven in clinical studies, large international registries, and postmortem studies.4-8
Polyvascular atherosclerosis in patients with single or multifocal clinical manifestations is associated with unfavorable clinical outcomes.4-6,9
Atherosclerotic lesions in the carotid arteries and the thickness of the intima‑media complex are recognized predictors of cardiovascular events in patients with symptomatic or asymptomatic ischemic heart disease and of complications during coronary angiography and coronary artery bypass graft (CABG) surgery.3,10-13
Significant coronary artery disease (CAD) coexisting with carotid stenosis in patients undergoing interventional treatment of carotid artery stenosis (stenting or endarterectomy) is associated with the risk of periprocedural cardiac complications (myocardial infarct).14,15
Available data emphasizing the clinical relevance of coronary atherosclerosis, particularly of the asymptomatic disease, in the evaluation of the prevalence of cerebral artery atherosclerosis and the risk for cerebral events are still scarce, which prompted us to investigate this area.16-18
Vascular ultrasound examination with Doppler color flow imaging is a modality routinely used to assess morphological changes in the carotid arteries and blood flow disturbances caused by atherosclerosis. Ultrasound examination of the intracranial arteries can also be used as an additional method to evaluate the risk of cardiovascular events in patients with atherosclerosis.19,20
The aim of this study was to determine the prevalence of hemodynamically significant stenosis of the carotid and/or cerebral arteries in patients with stable and unstable CAD.
An additional aim was to determine the prevalence of symptomatic carotid and cerebral artery stenosis coexisting with CAD.
Patients and methods
The study involved 241 patients with CAD who were hospitalized in the 3rd Department of Cardiology at Medical University of Silesia, Katowice, Poland.
In all patients, a medical history was taken and a physical examination was performed, including cardiac and neurological examinations, electrocardiography, echocardiography, coronary angiography, carotid artery ultrasound, and laboratory tests routinely carried out in patients admitted to the Department of Cardiology in order to diagnose CAD. In 114 patients, an additional ultrasound examination of the intracranial arteries with transcranial color Doppler (TCD) imaging was performed in the Department of Neurology at Medical University of Silesia, Katowice, Poland. The patients who underwent TCD imaging were selected randomly due to the availability of an ultrasound device in the Department of Neurology during their hospitalization. Primarily, there were 126 patients selected; however, in the end, 114 patients were included into our study due to lack of an appropriate acoustic window for the TCD examination in 12 patients.
Existing diseases and conditions commonly considered actual and possible risk factors for stroke were determined based on recent medical records and results of in‑hospital tests.
Heart failure, CAD, and myocardial infarction were defined based on the previously described and established recommendations,21,22 whereas stroke and transient ischemic attack (TIA) were defined according to the current American Stroke Association guidelines.23 All patients were evaluated for risk factors for atherosclerosis, which included arterial hypertension, diabetes, obesity, lipid disorders, and nicotinism.
Unstable CAD was defined as a coronary vascular disease causing acute coronary syndrome. The status of cardiac ischemia which did not lead to acute coronary syndrome was classified as stable CAD. An increase and/or decrease in cardiac troponin levels, with at least 1 value above the 99th percentile of the upper reference limit, was a parameter used to confirm acute coronary syndrome.
The abovementioned conditions were confirmed by a neurologist, a cardiologist, or an internist.
The exclusion criteria were as follows: nonatherosclerotic stenosis, potential causes of cerebral embolism other than atherosclerotic lesions in the carotid artery (atrial fibrillation, mitral and/or aortic valve stenosis, mechanical heart valve, persistent foramen ovale or another defect, interatrial septal aneurysm, cardiac myxoma, or a thrombus in the left ventricle or atrium), carotid artery dissection or intraluminal thrombosis visible on ultrasound and brain damage other than of vascular origin (detected on computed tomography or magnetic resonance imaging of the head), central nervous system (CNS) ischemic symptoms in the area of the posterior cerebral circulation.
All patients underwent coronary angiography according to the standard protocol.24 Based on coronary angiography results, patients with advanced coronary lesions were identified. These were patients who had atherosclerotic lesions causing stenosis greater than 50% in more than 2 sites and those with mild atherosclerotic lesions causing stenosis greater than 50%, found in 1 site or 2 sites.
Duplex Doppler ultrasound of the carotid and vertebral arteries was performed with the 7.5‑MHz linear array probe (Elegra, Siemens, Erlangen, Germany) and the degree of stenosis and atherosclerotic plaque morphology was assessed. Carotid stenosis was graded based on morphological data (B‑mode images, color flow imaging), velocity measurements (in the stenotic and poststenotic segments), and collateral flow evaluated according to the combined criteria for internal carotid stenosis grading published by von Reutern et al.25
For the purpose of this study, internal carotid artery (ICA) stenosis greater than 50% was considered significant. The velocity criteria for significant ICA stenosis (>50%) were as follows: peak systolic velocity greater than or equal to 120 cm/s, end diastolic velocity greater than or equal to 40 cm/s, the ratio of peak systolic velocity of ICA to peak systolic velocity of the common carotid artery greater than or equal to 2.
In all patients, carotid duplex Doppler ultrasound was performed by an experienced cardiologist (MK) and a neurologist (PP), who agreed on the degree of stenosis.
The intracranial arteries were examined by assessing the following hemodynamic parameters with TCD imaging: mean blood flow velocity in the arteries (periorbital arteries, middle cerebral arteries, anterior cerebral arteries, posterior cerebral arteries, vertebral arteries, and the basilar artery). The Pioneer 2002 TC device (EME, Überlingen, Germany), equipped with a 2‑MHz pulse‑wave Doppler ultrasound probe, was used.
The first part of the study aimed to evaluate mean blood flow velocity expressed in centimeters per second and the Gosling pulsatility index in the vertebral arteries, the basilar artery, the middle, anterior, and posterior cerebral arteries (at the depth of 56 mm, 70 mm, and 35 mm, respectively). Subjects were examined in a supine position, except for the assessment of the arteries of the vertebral‑basilar system, which was performed in a sitting position. The middle cerebral artery (MCA) stenosis greater than 50% was diagnosed based on the following criteria: mean velocity greater than 80 cm/s, systolic velocity greater than 160 cm/s, the ratio of mean velocity in the prestenotic site to mean velocity in the stenotic site of 1 to 2 or more, a segmental increase in mean velocity by 80 cm/s, the difference between mean velocity in the corresponding segment of the MCA on the opposite side greater than 30 cm/s, and the ratio of mean velocity in the MCA to mean velocity in ICA on the stenotic side greater than or equal to 2. The anterior cerebral artery stenosis greater than 50% was diagnosed based on the following criteria: a local increase in mean velocity with associated turbulence and Doppler spectrum broadening, systolic velocity greater than 120 cm/s, and a segmental increase in mean velocity by 80 cm/s. The posterior cerebral artery stenosis greater than 50% was diagnosed based on the following criteria: a local segmental increase in mean velocity by 30% in relation to the proximal and distal segments with associated turbulence and Doppler spectrum broadening, a segmental increase in mean velocity by 50 cm/s in relation to the adjacent vessel segments.26
Transcranial color Doppler imaging was performed by an experienced neurosonology specialist (PP, accredited with the International Certification in Neurosonology).
The prevalence of hemodynamically significant ICA stenosis, the presence of significant intracranial aortic stenosis, and clinical signs of CNS ischemia (TIA, stroke) were compared between patients with stable CAD and those with unstable CAD.
Statistical analysis
Statistical analysis was performed using the tests listed below. Basic statistical parameters were calculated for interval‑scale variables (mean [SD], median [interquartile range]). These variables were tested for normality using the Shapiro–Wilk test. Numbers and percentages were given for nominal variables. Mean and median values of interval‑scale variables were compared using the t test (for variables with normal distribution) or the Mann–Whitney test (for variables with distribution other than normal). Study groups were compared for nominal variables using the χ2 test or the Fisher test, depending on the group size. In order to identify risk factors for ICA stenosis, intracranial artery stenosis, and CNS ischemic events, univariable logistic regression analysis was applied. It included risk factors for atherosclerosis (age, sex, arterial hypertension, diabetes mellitus, lipid disorders, body mass index >25 kg/m2, nicotine abuse, and heart failure) and the presence and advancement of atherosclerotic lesions in the coronary vessels. Based on the presence of ICA and/or intracranial artery stenosis, a univariable analysis model was developed to assess the cumulative risk of CNS ischemic events in patients with comorbid ICA stenosis and intracranial arterial atherosclerosis. Odds ratios (ORs) with 95% CIs were calculated for the pre‑identified independent factors. A P value less than 0.05 was considered significant. Analyses were performed using the Statistica software, version 13.3 (Tibco Software, Inc., Palo Alto, California, United States).
The study was approved by the Bioethics Committee of the Medical University of Silesia (NN‑6501‑90/I/15). All patients were informed about the aim and course of the study and provided informed consent.
Results
The clinical characteristics of the study patients are presented in Table 1.
Parameter | Overall (n = 241) | Stable CAD (n = 183) | Unstable CAD (n = 58) | P valuea | ||
Data are presented as number (percentage) unless otherwise indicated.
a Comparison between patients with stable CAD and those with unstable CAD
Abbreviations: BMI, body mass index; CAD, coronary artery disease; LVEF, left ventricular ejection fraction; TIA, transient ischemic attack | ||||||
Age, y | Mean (SD) | 68.6 (8.8) | 68.9 (8.8) | 67.9 (9.1) | 0.47 | |
Median (range) | 69 (41–89) | 69 (41–89) | 67 (46–85) | |||
Female sex | 69 (28.6) | 51 (27.9) | 18 (31) | 0.64 | ||
Arterial hypertension | 200 (83) | 152 (83.1) | 48 (82.8) | 0.95 | ||
Diabetes mellitus | 83 (34.4) | 65 (35.5) | 18 (31) | 0.53 | ||
BMI | Mean (SD) | 28 (2.7) | 27.9 (2.7) | 28.9 (2.6) | 0.28 | |
Median (range) | 27.5 (22.7–39.3) | 27.5 (22.7–39.3) | 27.9 (22.9–35.9) | |||
Lipid disorders | 172 (71.4) | 134 (73.2) | 38 (65.5) | 0.26 | ||
History of stroke/TIA | 25 (10.4) | 18 (9.8) | 7 (12.1) | 0.63 | ||
Nicotinism | 123 (51) | 94 (51.4) | 29 (50) | 0.85 | ||
LVEF >50% | 173 (71.8) | 129 (70.5) | 44 (75.9) | 0.43 | ||
Stable CAD was diagnosed in 183 patients (75.9%), and unstable CAD in 58 (24.1%). Advanced coronary atherosclerotic lesions (stenosis >50% in more than 2 sites) were found in 26 patients (10.8%), single coronary artery stenosis greater than 50% in 103 (42.7%), and coronary artery stenosis in 2 sites in 112 (46.5%).
Internal carotid artery stenosis was diagnosed in 39 patients (16.2%). Symptoms of CNS ischemia were reported in the medical history of 25 patients (10.4%).
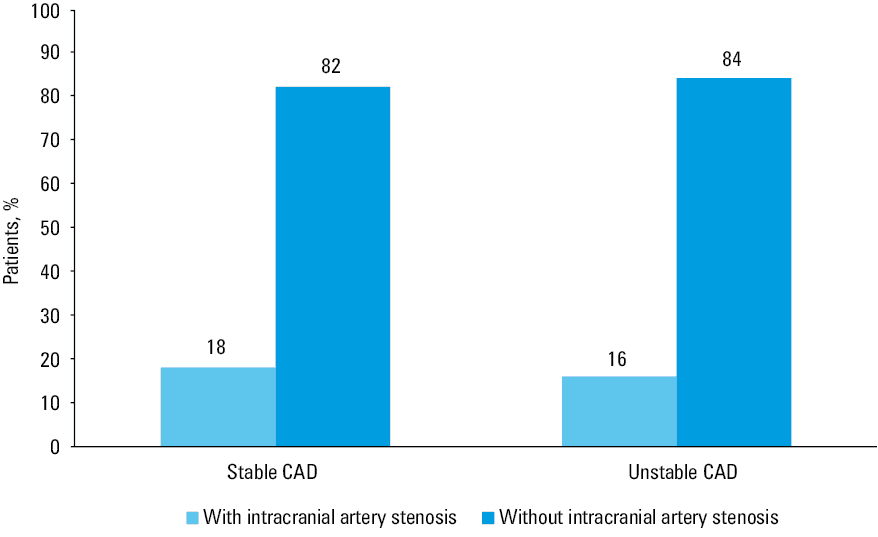
There was no significant difference in the prevalence of ICA stenosis greater than 50% between patients with stable CAD and those with unstable CAD. Internal carotid artery stenosis greater than 50% was found in 28 patients (15.3%) with stable CAD and in 11 (19%) with unstable CAD (P = 0.51). In logistic regression analysis, none of the analyzed factors turned out to be a risk factor for ICA stenosis.
Atherosclerotic stenoses of the intracranial arteries were diagnosed in 20 patients (17.6%). Of 114 patients included into the study, 89 (78%) were diagnosed with stable CAD, and 25 (22%) with unstable CAD. There was no difference in the prevalence of atherosclerotic intracranial artery stenosis between patients with stable CAD and those with unstable CAD. Intracranial artery atherosclerosis was found in 16 patients (18%) with stable CAD and in 4 (16%) with unstable CAD (P = 0.54) (Figure 1).
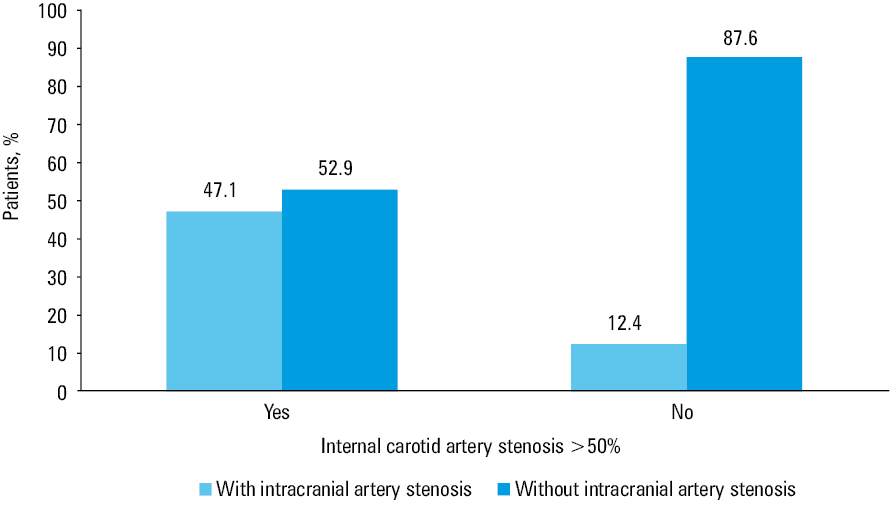
Atherosclerosis of the intracranial arteries was more frequent in patients with ICA stenosis greater than 50% (8 patients [47.1%]) than in those without ICA stenosis (12 patients [12.4%]); P = 0.005 (Figure 2). In logistic regression analysis, the following risk factors for intracranial atherosclerosis were identified: ICA stenosis (OR, 13.21; 95% CI, 5.93–41.89; P = 0.009) and advanced CAD (OR, 2.38; 95% CI, 1.13–4.09; P = 0.007) (Table 2).
Parameter | OR | 95% CI | P value |
Abbreviations: ICA, internal carotid artery; OR, odds ratio; others, see Table 1 | |||
Age | 1.04 | 0.96–1.07 | 0.21 |
Female sex | 0.85 | 0.36–1.57 | 0.81 |
BMI >25 kg/m2 | 1.13 | 0.85–2.61 | 0.15 |
Arterial hypertension | 0.38 | 0.03–1.77 | 0.36 |
Diabetes mellitus | 1.81 | 0.56–5.87 | 0.26 |
Nicotinism | 1.87 | 0.96–3.72 | 0.26 |
Lipid disorders | 0.97 | 0.55–1.76 | 0.17 |
Heart failure | 1.27 | 0.42–3.84 | 0.66 |
Unstable CAD | 0.75 | 0.37–1.42 | 0.95 |
Advanced CAD | 2.38 | 1.13–4.09 | 0.007 |
ICA stenosis >50% | 13.21 | 5.93–41.89 | 0.009 |
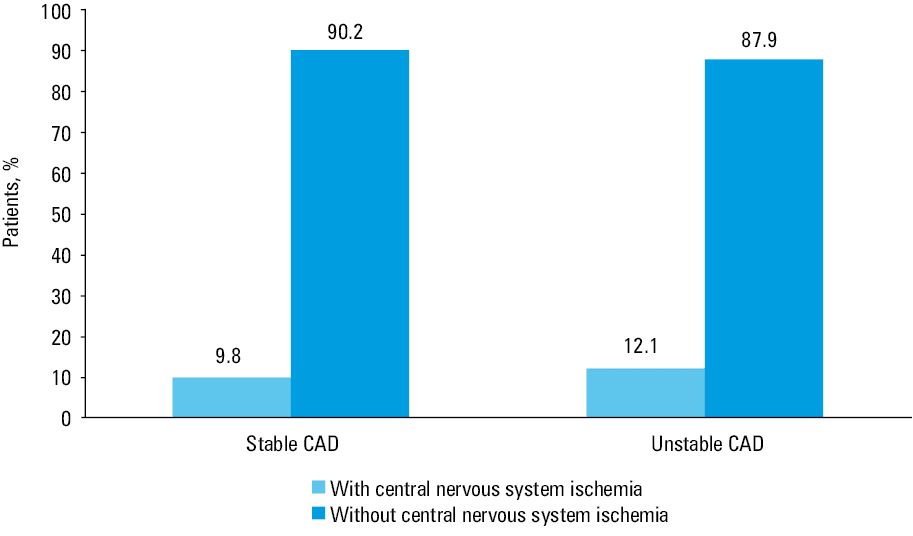
Symptoms of previous CNS ischemia were found in 18 patients (9.8%) with stable CAD and in 7 (12.1%) with unstable CAD (P = 0.63) (Figure 3). In all patients, symptoms of CNS ischemia due to large‑vessel atherosclerosis were seen in the area of the anterior cerebral circulation (anterior cerebral artery, MCA, ICA).
Logistic regression analysis showed that the factors associated with an increased risk of CNS ischemic events were as follows: ICA stenosis greater than 50% on 1 side or both sides (OR, 1.74; 95% CI, 1.01–3.16; P = 0.03), intracranial artery stenosis (OR, 3.01; 95% CI, 1.66–5.57; P = 0.03) (Table 3). The risk of CNS ischemic events in patients with comorbid ICA stenosis and intracranial artery atherosclerosis was particularly high (cumulative OR, 37.94; 95% CI, 29.82–48.29; P <0.001).
Parameter | OR | 95% CI | P value |
Age | 1.05 | 0.94–1.09 | 0.28 |
Female sex | 0.52 | 0.27–1.95 | 0.71 |
BMI >25 m/kg2 | 1.06 | 0.62–1.98 | 0.71 |
Arterial hypertension | 0.25 | 0.02–1.67 | 0.17 |
Diabetes mellitus | 0.49 | 0.13–1.97 | 0.56 |
Nicotinism | 0.4 | 0.20–1.13 | 0.34 |
Lipid disorders | 1.51 | 0.78–2.85 | 0.92 |
Heart failure | 1.22 | 0.71–2.16 | 0.96 |
Unstable CAD | 0.51 | 0.21–1.23 | 0.85 |
Advanced CAD | 1.04 | 0.29–3.73 | 0.94 |
ICA stenosis >50% | 1.74 | 1.01–3.16 | 0.03 |
Intracranial artery stenosis | 3.01 | 1.66–5.57 | 0.03 |
Discussion
The principal findings of this study, regarding the prevalence of significant stenosis of the carotid and cerebral arteries in patients with CAD, were as follows: 1) patients with stable CAD and those with unstable CAD do not differ in the prevalence of ICA and cerebral artery stenosis; and 2) advanced CAD is one of the risk factors for atherosclerosis of the cerebral arteries.
Atherosclerosis is a systemic disease. Therefore, the probability of comorbid arterial stenoses in diverse vascular territories is high. However, the level of such coexistence differs among studies. Polyvascular atherosclerosis was found in 15% to 46% of patients in various studies, and in more than 16% in our study. Such a difference can be explained by different study methods used by other authors.4,6,8,27-29 Different degrees of stenosis advancement in particular arteries can be observed in every patient. Multifocal localization of atherosclerosis is associated with unfavorable long‑term outcomes, and the cardiovascular risk is independently related to the number of arterial territories affected by significant atherosclerosis.4,6,8,9,18 The clinical manifestations of atherosclerosis in 1 vascular bed is often associated with symptoms of plaque destabilization in another vascular region, as factors predisposing to plaque ruptures can be present both locally and systemically.3,5
Available studies suggest that 24% of patients with CAD have atherosclerotic lesions in at least 1 additional site within the carotid, renal, and/or lower limb arteries, and the severity of stenotic lesions in the coronary arteries is associated with a greater number of lesions and greater severity of lesions in another area.30
Although the coexistence of carotid or intracranial atherosclerosis and CAD was confirmed in more than 16% of patients, we did not find a significant difference in the prevalence of ICA and intracranial artery stenoses between patients with stable CAD and those with unstable CAD.
Symptoms of CAD do not depend solely on the severity of atherosclerotic lesions in the coronary vessels. The clinical presentation of CAD depends on the site of particular lesions in the coronary vessels, the development of collateral circulation, atheromatous plaque morphology, the pattern and speed of its progression, its destabilization risk, comorbidities affecting pain perception, and the therapy applied. Patients with unstable CAD could be a heterogeneous group including patients with a single critical atherosclerotic lesion or those with advanced multivessel disease.
In our study group, advanced atherosclerosis of the coronary arteries was a risk factor for atherosclerosis of the intracranial arteries. This finding was similar to that reported by other authors.31
Our study confirmed that there is an increased risk of atherosclerotic lesions of the intracranial arteries in patients with ICA stenosis and a distinct cumulative risk of CNS ischemic events in patients with both these pathologies. The presence of such tandem stenoses is relevant not only because it influences the disease risk but also in terms of selecting the most suitable interventional treatment method.
From a clinical point of view, it is of key importance to determine the risk of CNS ischemic events in patients with advanced CAD and carotid artery stenosis before CABG, as different treatment strategies can be applied (simultaneous or staged carotid endarterectomy/CABG or carotid artery stenting/CABG).32 The risk of CNS ischemic events depends not only on the degree of ICA stenosis and the presence of bilateral ICA stenosis but also, as found in our study, on the presence of intracranial artery stenosis.
On the other hand, asymptomatic CAD coexisting with carotid stenosis is a risk factor for myocardial infarction during, and even after, interventional treatment of the carotid arteries. Therefore, we must look for asymptomatic CAD in patients with carotid stenosis.14,15 Musiałek et al14 proposed a novel carotid revascularization decision‑making model with coronary angiography before stenting to prevent coronary complications in the perioperative period. The findings of our study support such a multivessel approach in patients with 1 clinical manifestation of atherosclerosis. It would be reasonable to broaden the scope of diagnostic procedures in patients with CAD in order to assess the condition of the carotid and cerebral arteries, which would optimize the therapeutic strategy and help prevent stroke. To know the site and severity of atherosclerotic lesions is of importance to clinicians who qualify patients for interventional treatment of various vascular areas, as patients with multivessel disease gain fewer benefits.33
In clinical practice, our findings confirmed that extensive diagnostic work‑up performed in patients with advanced CAD, including the examination of the intracranial arteries, can help identify patients at risk of CNS ischemia.
Limitations
Our study had the following limitations: 1) lack of TCD imaging results in the entire study group (the examination was performed in almost a half of the patients); including only subjects who underwent TCD imaging would affect the sample size and lower the quality of performed search for associations; 2) different numbers of patients with stable and unstable CAD (a smaller number of those with unstable CAD)—it also limited the difference in the number of TCD examinations in both groups. It did not affect the results, as the percentage of patients with unstable CAD was similar, that is 24%, in the entire group and 22% in patients who underwent TCD imaging. The percentage of patients undergoing TCD imaging was proportional in those with stable and unstable CAD (48% vs 43%); 3) only stroke and TIA were treated as symptoms of CNS ischemia. We did not investigate other possible manifestations of CNS ischemia (eg, impairment of cognitive functions) and “silent” ischemic events revealed in neuroimaging studies. In accordance with the assumption and purpose of the study, we analyzed acute symptomatic incidents caused by atherosclerosis during the preceding 6 months (based on the definition adopted in guidelines by researchers and experts). It is impossible to assess the onset of silent strokes; 4) lack of subanalysis of patients divided according to the site of atherosclerotic lesions in the coronary vessels and the number of affected coronary vessels. It did not affect the results of the study, although such an analysis would increase its value; 5) lack of multivariable logistic regression analysis to identify potential independent risk factors for intracranial artery stenosis and CNS ischemia syndrome. Undoubtedly, this analysis would enhance the value of our study.
Conclusions
No differences between the prevalence of atherosclerosis of the carotid and cerebral arteries between patients with stable and unstable CAD were found in this study.
A total of 16% to 20% of study patients with unstable CAD had atherosclerotic stenosis of the carotid or cerebral arteries. However, in the majority of patients, stenosis was asymptomatic.
Advanced CAD is one of the risk factors for hemodynamically significant cerebral artery stenosis.
- Gepner AD, Young R, Delaney JA, et al. Comparison of coronary artery calcium presence, carotid plaque presence, and carotid intima‑media thickness for cardiovascular disease prediction in the Multi‑Ethnic Study of Atherosclerosis. Circ Cardiovasc Imaging. 2015; 8: e002262. | Crossref
- Sigala F, Oikonomou E, Antonopoulos AS, et al. Coronary versus carotid artery plaques. Similarities and differences regarding biomarkers morphology and prognosis. Curr Opin Pharmacol. 2018; 39: 9‑18. | Crossref
- Schneider A, Gawęcka J, Minczykowski A, et al. Arterial structure and function in patients with acute coronary syndrome after 1‑year treatment. Pol Arch Intern Med. 2017: 127: 184‑189. | Crossref
- Bhatt D, Steg P, Ohman E, et al. International prevalence, recognition and treatment of cardiovascular risk factors in outpatients with atherothrombosis. JAMA. 2006; 295: 180‑189. | Crossref
- Musialek P, Tracz W, Tekieli L, et al. Multimarker approach in discriminating patients with symptomatic and asymptomatic atherosclerotic carotid artery stenosis. J Clin Neurol. 2013; 9: 165‑175. | Crossref
ARTICLE INFORMATION