Can we predict the severity of coronavirus disease 2019 with a routine blood test?
Key words: coronavirus disease 2019, neutrophil-to-lymphocyte ratio, routine blood test



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Can we predict the severity of coronavirus disease 2019 with a routine blood test?
Introduction: The ongoing worldwide pandemic of coronavirus disease 2019 (COVID‑19) has posed a huge threat to global public health. However, the issue as to whether routine blood tests could be used to monitor and predict the severity and prognosis of COVID‑19 has not been comprehensively investigated so far.
Objectives: This study aimed to provide an overview of the association of markers in the routine blood test with the severity of COVID‑19.
Methods: PubMed, Embase, Cochrane Library, Wanfang, and China National Knowledge Infrastructure (CNKI) databases were searched to identify studies reporting data on markers in the routine blood test and the severity of COVID‑19, published until March 20, 2020. The STATA software was used for meta‑analysis.
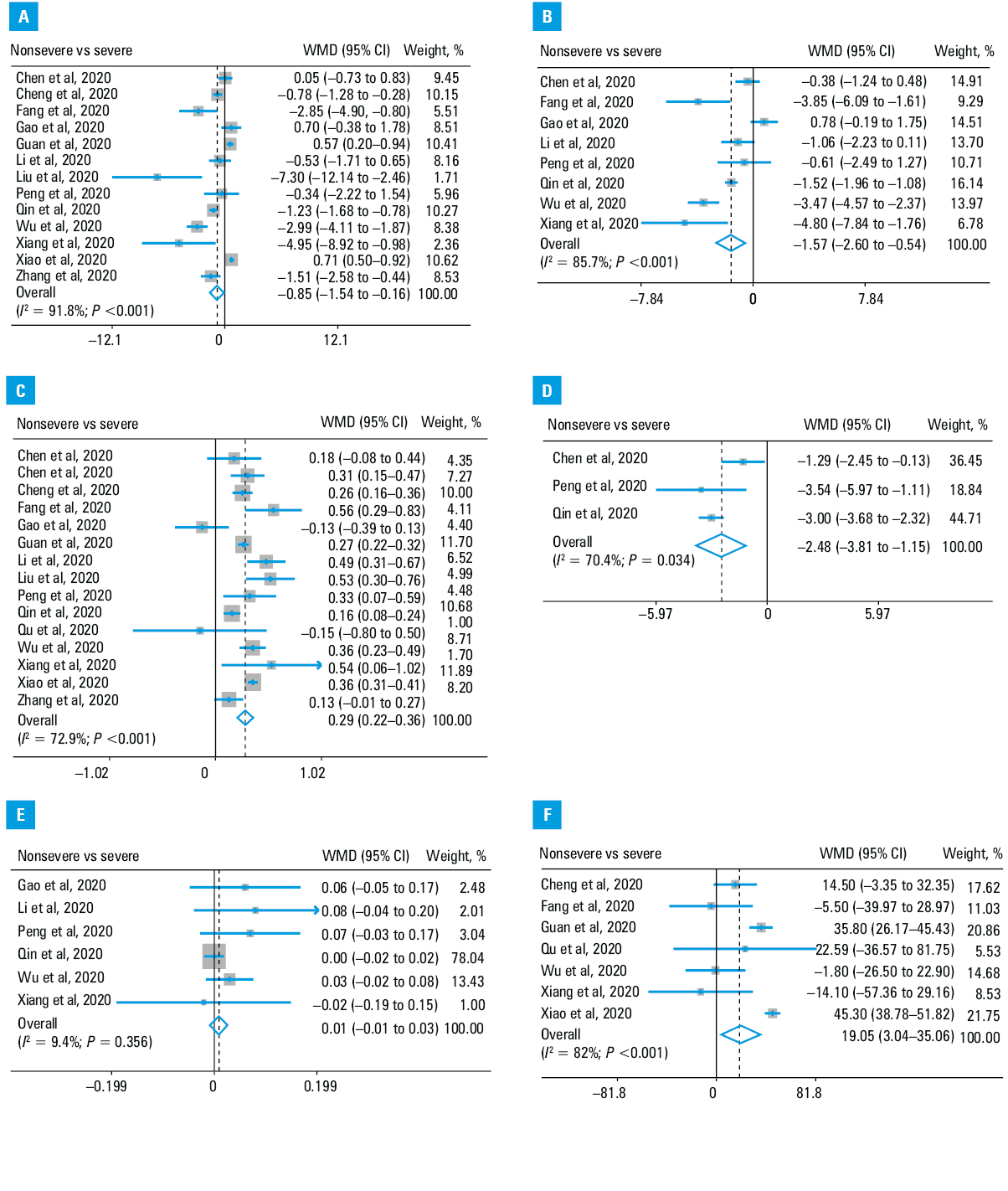
Results: A total of 15 studies with 3090 patients with COVID‑19 were included in this analysis. Patients in the nonsevere group, compared with those in the severe group, had lower counts of white blood cells (weighted mean difference [WMD], –0.85 [ × 109/l]; 95% CI,–1.54 to –0.16; P=0.02) and neutrophils (WMD, –1.57 [ × 109/l]; 95% CI, –2.6 to –0.54; P = 0.003), greater counts of lymphocytes (WMD, 0.29[ × 109/l]; 95% CI, 0.22–0.36; P <0.001) and platelets (WMD, 19.05 [ × 109/l]; 95% CI, 3.04–35.06; P=0.02), and a lower neutrophil‑to‑lymphocyte (NLR) ratio (WMD, –2.48; 95% CI, –3.81 to –1.15; P <0.001). There was no difference in the monocyte count (WMD, 0.01 [ × 109/l]; 95% CI, –0.01 to 0.03; P=0.029) between these 2 groups. Sensitivity analysis and meta‑analysis based on standard mean difference did not change the conclusions regarding neutrophils, lymphocytes, and NLR, but yielded inconsistent results for white blood cells and platelets.
Conclusions: Patients with severe COVID‑19 had a greater neutrophil count, a higher NLR, and a lower lymphocyte count than those with nonsevere COVID‑19. Evaluation of these markers might help clinicians to monitor and predict the severity and prognosis of COVID‑19.
What's new?
The ongoing worldwide pandemic of coronavirus disease 2019 (COVID‑19), caused by severe acute respiratory syndrome coronavirus 2 (SARS‑CoV‑2), has posed a huge threat to global public health, and combating the disease has therefore become one of the top priorities. However, it has not been comprehensively investigated so far whether routine blood tests could be used to monitor and predict the severity and prognosis of COVID‑19. In our study, we aimed to provide an overview of the association between markers in routine blood tests and the severity of COVID‑19. We found that patients with severe COVID‑19, compared with those with a nonsevere course of the disease, had a greater neutrophil count, a higher neutrophil‑to‑lymphocyte ratio (NLR), and a downregulated lymphocyte count. Evaluation of these markers in a routine blood test (particularly the neutrophil‑to‑lymphocyte ratio) might help clinicians to better monitor and predict the severity and prognosis of COVID‑19.
Introduction
The ongoing worldwide pandemic of coronavirus disease 2019 (COVID‑19), caused by severe acute respiratory syndrome coronavirus 2 (SARS‑CoV‑2), has posed a huge threat to global public health.1,2 As of March 21, 2020, a total of 266073 confirmed cases were reported, including 11183 deaths worldwide.3 An increasing number of studies has shown that most patients with COVID‑19 are asymptomatic or have mild pneumonia. However, a proportion of patients may develop severe or critical pneumonia, acute respiratory distress syndrome, or even die.4,5 Serum inflammatory markers such as C‑reactive protein and interleukin 6 have been reported to be positively correlated with the severity of COVID‑19, and the issue as to whether markers evaluated in a routine blood test could be used to predict the severity of COVID‑19 remains to be further investigated.6
A typical routine blood test is used to determine red blood cell (RBC), white blood cell (WBC), and platelet counts as well as levels of hemoglobin and other blood components. Besides, some potential inflammatory markers, such as neutrophil‑to‑lymphocyte (NLR) and platelet‑to‑lymphocyte (PLR) ratios, could also be calculated based on the routine blood test.7-10 A series of changes can be induced in the routine blood test by SARS‑CoV‑2 infection and some of them could be used to monitor and predict the severity and prognosis of COVID‑19.11,12 To date, although numerous studies reported the results of routine blood tests in patients with severe and nonsevere COVID‑19, a comprehensive analysis of all published studies4,7-10,13-22 has not been conducted yet. Here, we performed a meta‑analysis to evaluate the relationship between the markers detected in the routine blood test and the severity of COVID‑19.
Methods
Search strategy
This meta‑analysis was performed according to the Preferred Reporting Items for Systematic Reviews and Meta‑Analyses (PRISMA) guidelines. PubMed, Embase, Cochrane Library, Wanfang, and China National Knowledge Infrastructure (CNKI) databases were searched until March 20, 2020. The following combined search terms were used: (“novel coronavirus” OR “nCoV‑2019” OR “2019‑nCoV” OR “COVID‑19” OR “SARS‑CoV‑2”). All eligible articles were retrieved, and their references were searched for further potentially relevant articles. This study was performed in compliance with the declaration of Helsinki and local legislation. Neither ethics committee approval nor patient consent were required.
Selection criteria
English- or Chinese‑language publications reporting data on markers detected in routine blood tests in patients with COVID‑19 were included if they met the following criteria: 1) patients could be divided into the severe and nonsevere groups. Patients in the severe group were diagnosed with severe or critical COVID‑19, and patients in the nonsevere group, with mild or moderate COVID‑19, based on the New Coronavirus Pneumonia Prevention and Control Program published by the National Health Commission of China6; 2) literature and necessary hospital admission data were available; and 3) the diagnostic criteria of COVID‑19 were clarified based on laboratory‑confirmed SARS‑CoV‑2 infection. Studies were excluded if full texts were not available or they did not fulfill the inclusion criteria.
Data extraction and quality assessment
Two authors independently scanned the records from the initial search to exclude any duplicate and irrelevant studies. The following data were extracted: first authors, publication date, country of origin, grouping, cases, age, sex, and markers detected in the routine blood test in patients with severe and nonsevere COVID‑19. Stratified data or interquartile ranges were converted to mean (SD) based on mathematical formulas for meta‑analysis. Any discrepancies were resolved by consensus. The Newcastle–Ottawa Scale (NOS) was used to assess the quality of all potentially eligible studies. Studies with fewer than 7 NOS stars were considered of inferior quality and therefore excluded.
Statistical analysis
All statistical analyses were carried out using the STATA software, version 12.0 (STATA Corporation, College Station, Texas, United States). The I2 and P values were used to evaluate statistical heterogeneity. In the case of low heterogeneity (I2 ≤50% and P ≥0.1), the fixed‑effects model was adopted, and in other cases the random‑effects model was used (I2 >50% or P <0.1).23 Weighted mean difference (WMD) with 95% CIs was calculated for the markers detected in the routine blood test. Standard mean difference (SMD) was used to explore the consistency of the conclusion. Sensitivity analysis was performed by omitting 1 study each time through influence analysis to assess the stability of results. Publication bias was assessed by the Egger test. If it was confirmed, the Duval and Tweedie trim‑and‑fill method was implemented to adjust for this bias. A P value less than 0.05 was considered significant.
Results
Literature search and study characteristics
A total of 5385 records were generated by the initial literature search, and 734 studies were subsequently excluded due to duplication (Figure 1). Then, we excluded 4616 studies after reviewing titles and abstracts and further 19 after scanning full texts. Finally, 15 studies were included in our analysis and all of them reported data on markers detected in the routine blood test.4,7-10,13-22 The basic characteristics of 15 eligible studies are presented in Table 1. All of these studies were published in 2020, came from China, and involved 3090 patients. All studied patients could be divided into the nonsevere and severe groups. In general, patients in the severe group were older than those in the nonsevere group, except for the study by Peng et al.8 One study did not report patients’ age, and 2 studies did not provide data on patients’ sex.10,18 All studies with 7 or more NOS stars were deemed to be of high quality and detailed data can be found in Supplementary material, Table S1.
Study | Year | Country | COVID‑19 group | Patients, n | Age, y, mean (SD) | Male sex, % | Inflammatory markers | Quality |
Abbreviations: COVID‑19, coronavirus disease 2019; NLR, neutrophil‑to‑lymphocyte ratio; PLR, platelet‑to‑lymphocyte ratio; RBCs, red blood cells; WBCs, white blood cells | ||||||||
Chen et al13 | 2020 | China | Nonsevere | 15 | – | – | Lymphocytes | 7 |
Severe | 14 | – | – | |||||
Chen et al7 | 2020 | China | Nonsevere | 108 | 42.9 (12.8) | 58 (53.7) | Lymphocytes, WBCs, neutrophils, NLR | 7 |
Severe | 31 | 55.5 (17.9) | 18 (58.1) | |||||
Cheng et al14 | 2020 | China | Nonsevere | 282 | 49.7 (11.9) | 145 (51.42) | Lymphocytes, WBCs, platelets | 8 |
Severe | 181 | 54.7 (13.5) | 99 (54.7) | |||||
Fang et al15 | 2020 | China | Nonsevere | 55 | 39.9 (14.9) | 27 (49.1) | Lymphocytes, WBCs, neutrophils, platelets | 7 |
Severe | 24 | 56.7 (14.4) | 18 (75) | |||||
Gao et al16 | 2020 | China | Nonsevere | 28 | 43 (14) | 17 (60.7) | Lymphocytes, WBCs, neutrophils, monocytes | 9 |
Severe | 15 | 45.2 (7.7) | 9 (60) | |||||
Guan et al4 | 2020 | China | Nonsevere | 926 | 45.4 (17.1) | 537 (58.2) | Lymphocytes, WBCs, platelets | 8 |
Severe | 173 | 52.4 (18.7) | 100 (57.8) | |||||
Li et al17 | 2020 | China | Nonsevere | 58 | 41.9 (10.6) | 29 (50) | Lymphocytes, WBCs, neutrophils, monocytes | 7 |
Severe | 25 | 53.7 (12.3) | 15 (60) | |||||
Liu et al18 | 2020 | China | Nonsevere | 26 | – | – | Lymphocytes, WBCs | 7 |
Severe | 4 | – | – | |||||
Peng et al8 | 2020 | China | Nonsevere | 96 | 61.5 (9.4) | 44 (45.83) | Lymphocytes, WBCs, neutrophils, NLR, monocytes | 8 |
Severe | 16 | 58.2 (7.3) | 9 (56.25) | |||||
Qin et al9 | 2020 | China | Nonsevere | 166 | 52 (15.5) | 80 (48.2) | Lymphocytes, WBCs, neutrophils, NLR, monocytes | 7 |
Severe | 286 | 60.3 (13.4) | 155 (54.2) | |||||
Qu et al10 | 2020 | China | Nonsevere | 27 | 49.4 (14.9) | – | Lymphocytes, platelets, PLR | 7 |
Severe | 3 | 60.0 (5.3) | – | |||||
Wu et al19 | 2020 | China | Nonsevere | 117 | 47.3 (10.5) | 68 (58.1) | Lymphocytes, WBCs, neutrophils, monocytes, platelets | 7 |
Severe | 84 | 59.2 (14.3) | 60 (71.4) | |||||
Xiang et al20 | 2020 | China | Nonsevere | 40 | 40.6 (14.3) | 25 (63.5) | RBCs, lymphocytes, WBCs, neutrophils, monocytes, platelets | 8 |
Severe | 9 | 53 (14) | 8 (88.9) | |||||
Xiao et al21 | 2020 | China | Nonsevere | 107 | 43.05 (1.13) | 52 (48.6) | Lymphocytes, WBCs, platelets | 7 |
Severe | 36 | 51.28 (5.58) | 20 (55.6) | |||||
Zhang et al22 | 2020 | China | Nonsevere | 82 | 51.6 (10.7) | 38 (46.3) | Lymphocytes, WBCs | 7 |
Severe | 56 | 62.7 (13.6) | 33 (56.9) | |||||
Association of markers detected in the routine blood test with the severity of coronavirus disease 2019
Thirteen studies reported WBC count in the nonsevere and severe groups. Random‑effects results demonstrated that patients in the nonsevere group had lower WBC count than those in the severe group (WMD, –0.85[ × 109/l]; 95% CI, –1.54 to –0.16; P = 0.02) (Figure 2). Besides, 8 studies reported neutrophil counts in these 2 groups. Random‑effects results showed that a lower neutrophil count were found in the nonsevere group compared with the severe group (WMD, –1.57[ × 109/l]; 95% CI, –2.6 to –0.54; P = 0.003). Fifteen studies reported lymphocyte counts in both groups, and random‑effects results showed higher values in the nonsevere group compared with the severe group (WMD, 0.29[ × 109/l]; 95% CI,0.22–0.36; P <0.001). NLR is a potential inflammatory marker and has been reported in 3 studies. Data pooled using a random‑effects model showed that patients with nonsevere COVID‑19 had lower NLR than those with severe COVID‑19 (WMD, –2.48; 95% CI,–3.81 to –1.15; P <0.001). Six studies provided data on monocyte counts. Fixed‑effects results showed no difference between both patient groups (WMD, 0.01[ × 109/l]; 95% CI,–0.01 to 0.03; P = 0.029). Seven studies reported platelet counts, and random‑effects results revealed higher values in the nonsevere group compared with the severe group (WMD, 19.05[ × 109/l]; 95% CI, 3.04–35.06; P = 0.02). Additionally, Xiang et al20 found no difference in the RBC count between these 2 groups, whereas Qu et al10 observed a higher PLR in patients with severe COVID‑19 than in those with nonsevere COVID‑19. The meta‑analysis of RBC and PLR values could not be conducted due to limited data.
Investigation of heterogeneity
Strong evidence of heterogeneity was found in some comparisons. As for neutrophils, lymphocytes, and NLR, sensitivity analysis and meta‑analysis based on SMD did not affect the conclusions. In the case of WBCs, when we deleted the study by Wu et al,19 the conclusion changed (WMD, –0.61[ × 109/l]; 95% CI, –1.27 to 0.06; P = 0.07). Besides, it also changed when we used SMD for meta‑analysis (SMD, –0.31; 95% CI,–0.69 to 0.06; P = 0.1). Regarding platelets, when we excluded the study by Guan et al,4 the conclusion changed (WMD, 12.3 [ × 109/l]; 95% CI, –11.91 to 36.5; P = 0.32), but using SMD for meta‑analysis did not alter it. As for monocytes, a greater monocyte count was observed in the nonsevere group than in the severe group after deleting the study by Qin et al9 (WMD, 0.04 [ × 109/l]; 95% CI, 0.01–0.08; P = 0.02). Detailed data on sensitivity analysis are shown in Supplementary material, Figure S1. The results of meta‑analysis based on SMD are shown in Table 2. Moreover, publication bias was present regarding data on WBCs and platelets (P <0.05), while no trimming was performed through the Duval and Tweedie trim‑and‑fill method (Supplementary material, Figure S2). Overall, the conclusions on WBCs, platelets, and monocytes should be treated with caution.
Parameter | Studies, n | Patients, n | Heterogeneity | Model | SMD | 95% CI | P value | |
I2 value | P value | |||||||
Abbreviations: SMD, standard mean difference; others, see Table 1 | ||||||||
WBCs | 13 | 3031 | 94% | <0.001 | Random | –0.31 | (–0.69 to 0.06) | 0.1 |
Neutrophils | 8 | 1158 | 82% | <0.001 | Random | –0.62 | (–0.96 to –0.28) | <0.001 |
Lymphocytes | 15 | 3090 | 91% | <0.001 | Random | 0.81 | (0.49–1.13) | <0.001 |
NLR | 3 | 703 | 0 | 0.8 | Fixed | –0.69 | (–0.86 to –0.52) | <0.001 |
Monocytes | 5 | 488 | 0 | 0.81 | Fixed | 0.23 | (0.04–0.43) | 0.02 |
Platelets | 7 | 2064 | 96% | <0.001 | Random | 0.67 | (0.03–1.31) | 0.04 |
Discussion
Coronavirus disease 2019 has rapidly spread globally, and currently there is no specific medication to treat this condition.24 As previously mentioned, COVID‑19 represents a spectrum of clinical severity ranging from asymptomatic to critical pneumonia, acute respiratory distress syndrome, and even death. Therefore, the close assessment of the severity of COVID‑19 and effective early interventions are key measures to reduce mortality. A routine blood test is easy to conduct even in community hospitals. Emerging studies have reported the results of routine blood tests performed in patients with severe and nonsevere COVID‑19. Further comprehensive studies are needed to determine whether these tests could be used to monitor and predict the severity and prognosis of COVID‑19.
In this meta‑analysis, we included 15 studies, which presented some results of routine blood tests carried out in patients with COVID‑19. In detail, 13 studies reported data on WBCs, 8 on neutrophils, 15 on lymphocytes, 3 on NLR, 6 on monocytes, 7 on platelets, 1 on RBCs, and 1 on PLR. Compared with patients with nonsevere COVID‑19, those with severe COVID‑19 had upregulated WBC and neutrophil counts and a higher NLR but downregulated lymphocyte and platelet counts. Sensitivity analysis and meta‑analysis based on SMD did not change the conclusion about neutrophils, lymphocytes, and NLR, whereas the results regarding WBCs and platelets were inconsistent. There was no difference in monocyte counts between these 2 patient groups. Thus, we could conclude that the neutrophil count and NLR were positively correlated with the severity of COVID‑19, and the lymphocyte count was negatively related to the severity of this disease.
The role of neutrophils in viral infections has not been fully elucidated yet, and an increasing number of studies have shown that neutrophils exhibit both protective and pathologic functions.25 On one hand, infection with the influenza A (H3N2) virus or recombinant H1N1 virus could cause severe disease in mice, depleting neutrophils with an anti‑Gr‑1 monoclonal antibody.26,27 On the other hand, neutrophil survival could be prolonged for several days after virus infection.28 The prolonged activation of neutrophils results in producing proinflammatory mediators and toxic substances, which is detrimental to the host.26,27 In this meta‑analysis, we found a greater neutrophil count in patients with severe COVID‑19 than in those with nonsevere disease. Although the impact of neutrophils on SARS‑CoV‑2 was unknown, we could use them to monitor the severity of COVID‑19. Lymphocytosis is often seen in viral infections, as its underlying mechanism has a protective role exhibited by taking up and inactivating infectious viruses. In our study, a decreased lymphocyte count was observed in patients with severe COVID‑19. A possible reason for this finding is that lymphocytes are depleted, as the virus is engulfed. Another reason may be that lymphocytes could be directly infected and destroyed by SARS‑CoV‑2, because the coronavirus angiotensin‑converting enzyme 2 receptor was expressed in lymphocytes.29
The neutrophil‑to‑lymphocyte ratio is a parameter, which amplifies the value of neutrophils and lymphocytes.30 Numerous studies have highlighted the importance of NLR in the diagnosis and prognosis of virus infection. For example, Han et al31 found that NLR had a higher sensitivity than neutrophil and lymphocyte counts alone and could act as a preferable diagnostic tool to screen patients infected with influenza virus. Besides, NLR is associated with chronic hepatitis B virus infection and could be used to predict its recurrence.32,33 In our analysis, 3 studies reported data on NLR, which was positively correlated with the severity of COVID‑19. This conclusion was consistent with the results of a recent study,34 although we had different research purposes and selection criteria. This finding was easy to explain due to more neutrophils and fewer lymphocytes detected in patients with severe COVID‑19 than in those with nonsevere disease. Also, 1 study reported that severely ill patients had a higher PLR than patients with nonsevere COVID‑19. Similar to NLR, PLR amplifies the value of platelets and lymphocytes. Further large‑scale studies are needed to validate the value of PLR.
Limitations
To our knowledge, this is the first meta‑analysis on the associations of markers detected in the routine blood test with the severity of COVID‑19. Admittedly, our meta‑analysis had some limitations. First, notable heterogeneity was seen in some comparisons and could not be fully eliminated, although sensitivity analysis and SMD were used for meta‑analysis. Second, publication bias was present regarding data on platelet and monocyte counts, but the conclusion did not change after using the trim‑and‑fill method. Third, other markers, such as eosinophils and basophils, were not included in the study due to data unavailability. Finally, it needs to be further investigated whether the conclusion is consistent among other countries, since the studies included in our meta‑analysis were from China.
Conclusions
In conclusion, our study showed that patients with severe COVID‑19 had a greater neutrophil count, a higher NLR, and a lower lymphocyte count than those with nonsevere COVID‑19. Evaluation of these markers in routine blood tests might help clinicians to monitor and predict the severity and prognosis of COVID‑19.
- World Health Organization. WHO virtual press conference on COVID‑19. https://www.who.int/docs/default‑source/coronaviruse/situation‑reports/20200311‑sitrep‑51‑covid‑19.pdf?sfvrsn=1ba62e57_10. Published March 11, 2020. Accessed March 11, 2020.
- Bedford J, Enria D, Giesecke J, et al. COVID‑19: towards controlling of a pandemic. Lancet. 2020; 395: 1015‑1018. | Crossref
- World Health Organization. WHO virtual press conference on COVID‑19. https://www.who.int/docs/default‑source/coronaviruse/situation‑reports/20200321‑sitrep‑61‑covid‑19.pdf?sfvrsn=ce5ca11c_2. Published March 21, 2020. Accessed March 21, 2020.
- Guan WJ, Ni ZY, Hu Y, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020; 382: 1708‑1720.
- Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID‑19 in Wuhan, China: a retrospective cohort study. Lancet. 2020; 395: 1054‑1062. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION