Addressing multiple gastroenterological aspects of coronavirus disease 2019
Key words: coronavirus disease 2019, gastrointestinal symptoms, pandemic, severe acute respiratory syndrome coronavirus 2



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Addressing multiple gastroenterological aspects of coronavirus disease 2019
The outbreak of the coronavirus disease 2019 (COVID‑19) pandemic has become the biggest challenge for the whole human community since many years. It seems that the proper identification of all people infected with severe acute respiratory syndrome coronavirus 2 (SARS‑CoV‑2) is the best strategy to limit the transmission. However, in a significant proportion of patients, there are no clinical manifestations of the disease, and symptoms may be very mild or atypical. There is a growing body of evidence that digestive manifestations of COVID‑19 are frequently reported and may precede typical respiratory symptoms. Moreover, SARS‑CoV‑2 particles were found in the gastrointestinal epithelial cells, and viral RNA was detected in the feces of patients with COVID‑19. These data suggest that gastrointestinal symptoms in COVID‑19 are not accidental findings and they may result from direct digestive involvement. Patients with new‑onset diarrhea, abdominal pain, nausea, and vomiting without any other evident etiological factors should be tested for SARS‑CoV‑2 infection. Gastroenterologists and members of other medical specialties should also remember that the current epidemiological situation has changed diagnostic and therapeutic algorithms in the management of several gastrointestinal and liver disorders. This review article summarizes the currently available data on multiple gastroenterological aspects of COVID‑19 and provides information on practical recommendations and position statements of the most prominent associations in the field of gastroenterology, which appeared in response to the emergence of the pandemic.
Introduction
In recent weeks, the outbreak of the coronavirus disease 2019 (COVID‑19) pandemic has dramatically changed our everyday life all over the world. The first cases of a new disease entity, leading to severe pneumonia in some patients, were identified in December 2019 in China.1 Soon after that, the etiological factor was determined, that is, the novel virus belonging to the genus Betacoronavirus, currently known as severe acute respiratory syndrome coronavirus 2 (SARS‑CoV‑2).2 It is considered to be bat‑derived and transmitted to humans by an unknown intermediate host. Then, dynamic human‑to‑human spread resulted in a rapidly growing number of infected people worldwide.1,2 Droplets, aerosols, and direct contact with contaminated surfaces are the main transmission routes. As of April 19, 2020, more than 2300000 cases of COVID‑19 were reported, including almost 160000 deaths.3
The most frequent symptoms of COVID‑19 include fever, dry cough, chills, and shortness of breath.4 Taking into account the epidemiological and medical significance of this disease, a huge effort is continuously being made by the scientific community all over the world to better understand all issues related to COVID‑19 and fight the pandemic. Recently, some new interesting reports on possible, less typical clinical manifestations of COVID‑19 have been published. Namely, it has been suggested that isolated gastrointestinal symptoms could be present in the initial phase of the disease in about 10% of cases.5,6 Moreover, SARS‑CoV‑2 was found in the gastrointestinal epithelial cells, and viral RNA was detected in the stool of patients with COVID‑19, which raises the question as to whether fecal‑oral transmission of SARS‑CoV‑2 infection is possible.6,7 This review presents the currently available data on multiple gastroenterological aspects of COVID‑19, including the summary of practical recommendations and information covered in the position statements of the most prominent associations in the field of gastroenterology, which appeared in response to the emergence of the pandemic.
Pathogenesis of severe acute respiratory syndrome coronavirus 2 infection: what we know and why it is important
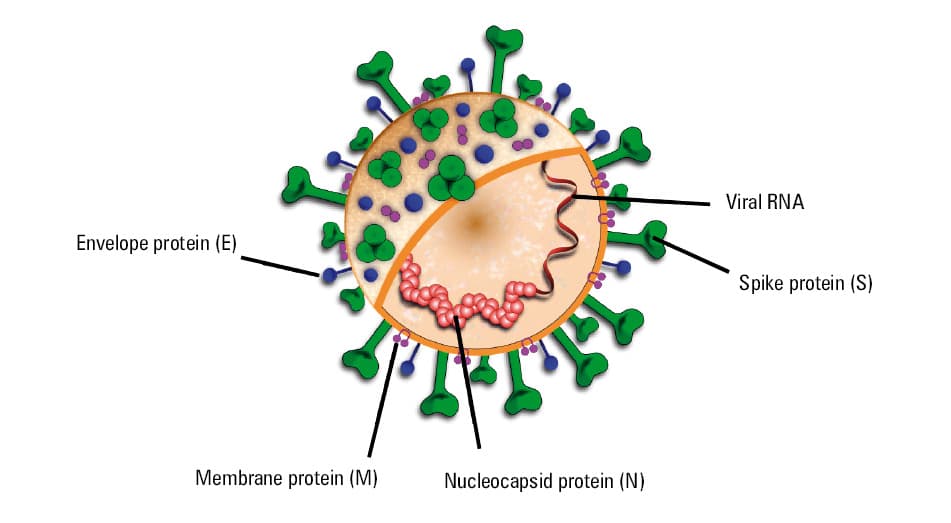
Severe acute respiratory syndrome coronavirus 2 belongs to the Coronaviridae family (Figure 1).8 It shares many similarities with other coronaviruses, like SARS‑CoV and Middle East respiratory syndrome coronavirus (MERS‑CoV), which were responsible for epidemics in 2003 and 2012, respectively.2,4 However, the number of patients who developed severe acute respiratory syndrome and Middle East respiratory syndrome was significantly lower than that of people with COVID‑19 reported nowadays. This was due to lower infectivity of these diseases and higher mortality associated with their development.9 The genome of SARS‑CoV is in almost 90% similar to that of SARS‑CoV‑2.4 It also appears that both viruses use similar molecular virulence pathways.
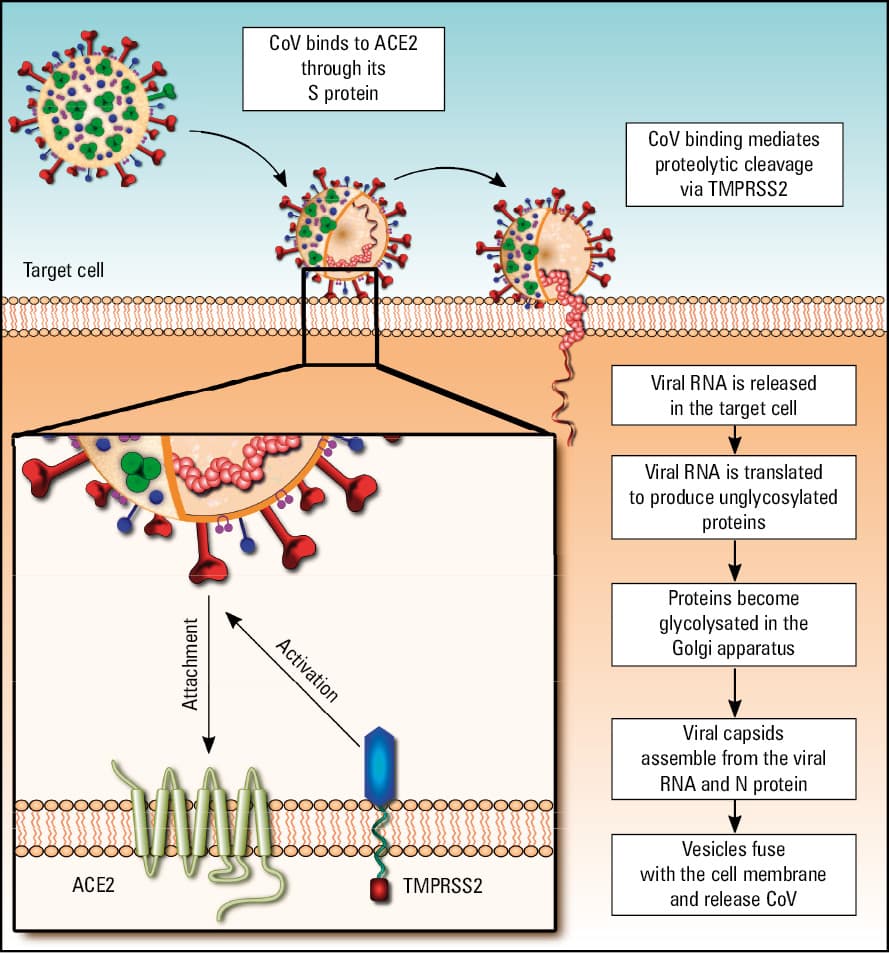
The angiotensin‑converting enzyme 2 (ACE2) plays the crucial role here, serving as an entry receptor for SARS‑CoV and SARS‑CoV‑2.4,10 Zhou et al,4 who discovered this, used the HeLa cell model to show that SARS‑CoV‑2 has a very high affinity to ACE2 and it does not infect cells in which ACE2 is not expressed. In contrast to SARS‑CoV, SARS‑CoV‑2 does not use other receptors, such as aminopeptidase N (APN) and dipeptidyl peptidase‑4 (DPP4) receptors. Further studies also revealed the key role of the host transmembrane serine protease (TMPRSS) in SARS‑CoV‑2 infectivity.11,12 It seems to be co‑localized with ACE2 in the same cells, dynamically interacting with the viral transmembrane spike glycoprotein (S protein). The angiotensin‑converting enzyme 2 acts on cellular attachment and recognition of the viral particles, whereas TMPRSS (particularly type 2 transmembrane serine protease [TMPRSS2]) regulates the cleavage of the S protein and membrane fusion of SARS‑CoV‑2 with the host cell (Figure 2).4,6,11,12
The main question is which molecular mechanisms are responsible for different clinical courses of COVID‑19, which vary from asymptomatic cases to developing severe acute respiratory syndrome leading to death. The same heterogeneity was observed in the case of SARS where older age, comorbidities (particularly cardiopulmonary diseases and severe immunosuppression), and male sex were the main risk factors for higher mortality.13 Considering numerous genomic (between SARS‑CoV and SARS‑CoV‑2) and clinical (between SARS and COVID‑19) similarities, it can be assumed that both diseases may share many pathogenetic mechanisms. In SARS, tracheobronchial and alveolar epithelium was shown to be the primary site of viral infection followed by a cascade of SARS‑CoV‑induced processes. The most important ones include: 1) a direct cytopathic effect, resulting in apoptosis of infected cells; 2) downregulation of ACE2 expression, a metalloproteinase playing the key protective role in severe lung injury; and 3) dysregulation of the immune system with excessive secretion of proinflammatory cytokines and activation of immunosuppressive mechanisms.13
The same findings are to be confirmed for COVID‑19, and some of them have been recently documented. For example, it was shown that the severity of the clinical course of COVID‑19 is associated with higher levels of several proinflammatory cytokines, suggesting that tissue injury may be mostly driven by excessive activation of immune mechanisms.10,14
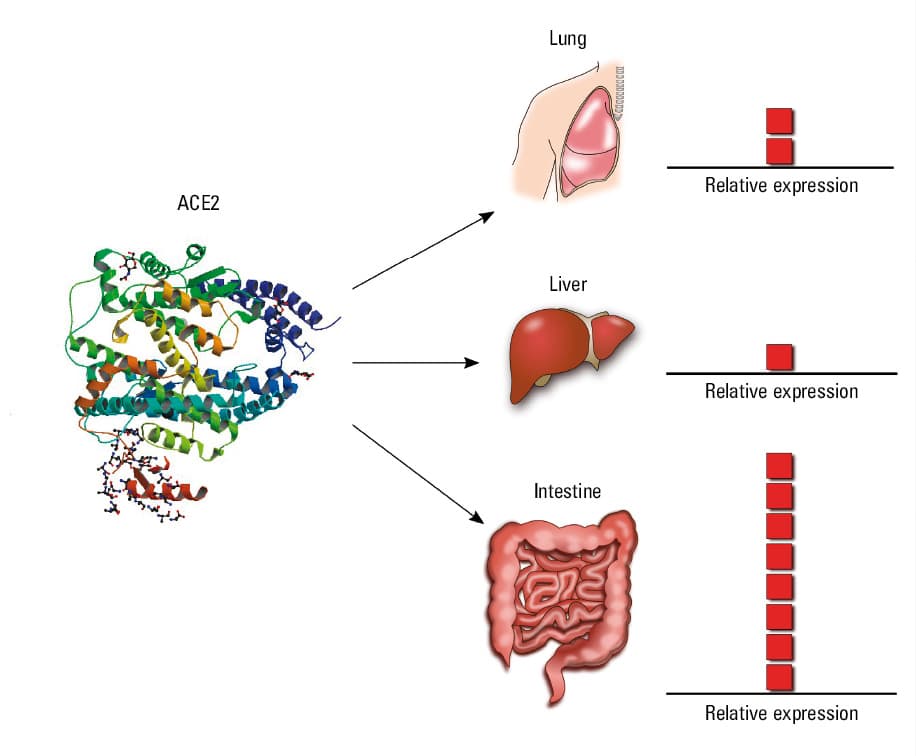
Interestingly, the crucial protein for SARS‑CoV‑2 infectivity, namely ACE2, is expressed not only in the tracheobronchial and alveolar epithelium (mainly on type 2 alveolar cells) but also in endothelial and smooth muscle cells of various visceral organs.13,15 Moreover, Xiao et al16 showed that ACE2 is present in the esophageal epithelium, glandular gastric mucosa, enterocytes, and colonocytes as well. This is in line with other reports suggesting that the gastrointestinal tract is one of those sites in the human body where the highest amount of ACE2 is expressed, even when compared with the lower respiratory tract (Figure 3).17-20 The liver is another digestive organ which may be infected by SARS‑CoV‑2. Recent analyses showed high ACE2 expression in cholangiocytes, indicating a possible link between viral infection and liver injury.6,21
Coronavirus disease 2019: gastrointestinal involvement and symptomatology
Gastrointestinal manifestations were frequently reported during the SARS epidemic in 2003.13 For example, more than a half of the patients developed watery diarrhea during the course of the disease. Surprisingly, although SARS‑CoV was found in the cytoplasm of mucosal epithelial cells and lamina propria lymphocytes (mainly in the stomach and the small intestine) when molecular methods were applied, there were no obvious inflammatory lesions detected in the histopathological examination.13 The depletion of mucosa‑associated lymphoid tissue was the most prominent abnormal finding. However, it was hypothesized that digestive involvement in SARS is not a result of oral transmission but is likely secondary to virus spread caused by infected immune cells from the lungs.13
Based on numerous clinical and pathophysiological similarities between SARS‑CoV and SARS‑CoV‑2, it can be expected that gastrointestinal manifestations may also occur in COVID‑19. There is a growing body of evidence confirming this hypothesis. However, the frequency of gastrointestinal symptoms is not consistent among various reports (Table 1).22 Wang et al23 were one of the first authors to report the full clinical profile of COVID‑19, showing that diarrhea, nausea, abdominal pain, and vomiting were noted in 10%, 10%, 2.2%, and 3.6% of patients, respectively. What is even more important, one‑tenth of patients had initial symptoms of diarrhea and nausea, which appeared before fever and dyspnea. In a large retrospective study, including 1099 patients with COVID‑19, it was shown that gastrointestinal symptoms were less frequent, including diarrhea and nausea or vomiting reported in 3.7% and 5% of patients, respectively.1 Luo et al5 published contradictory data. In a group of 1141 patients hospitalized in the Zhongnan Hospital of Wuhan University, in whom the diagnosis of COVID‑19 was made based on chest computed tomography and detection of viral RNA in the nasopharyngeal swab examined with the reverse transcriptase–polymerase chain reaction test, gastrointestinal symptoms were reported as the only manifestation of COVID‑19 at the time of diagnosis in 183 cases (16%). Loss of appetite, nausea, vomiting, abdominal pain, and diarrhea were the most common symptoms. These observations were confirmed in the most recent multicenter cross‑sectional study from China, which reported a 50% frequency of COVID‑19 digestive manifestations.24 After excluding loss of appetite, being a less specific gastrointestinal symptom, still almost one‑fifth of the analyzed group reported diarrhea, vomiting, and/or abdominal pain. Moreover, 3% of patients developed digestive symptoms only, with no respiratory manifestations present.
Study | Type | Patients, n | Frequency of digestive symptoms |
Guan et al1 | Retrospective descriptive study | 1099 | Nausea or vomiting (5%)
Diarrhea (4%) |
Luo et al5 | Retrospective descriptive study | 1141 | Any digestive symptom (16%):
• Loss of appetite (98%)
• Nausea (73%)
• Vomiting (65%)
• Diarrhea (37%)
• Abdominal pain (25%) |
Pan et al24 | Retrospective cross‑sectional descriptive study | 206 | Any digestive symptom (57%)
Diarrhea (32%) |
Jin et al26 | Retrospective descriptive study | 651 | Any digestive symptom (11%)
Diarrhea (8%)
Vomiting (2%)
Nausea (2%) |
Nobel et al29 | Retrospective case‑control study | 278 | Any digestive symptom (35%)
Nausea and/or vomiting (23%)
Diarrhea (20%) |
Cheung et al27 | Meta‑analysis | 4243 | Any digestive symptom (18%)
Loss of appetite (27%)
Nausea and/or vomiting (10%)
Diarrhea (12%)
Abdominal pain and/or discomfort (9%) |
Recently, several reports on the clinical characteristics of COVID‑19 outside Wuhan have been published. Wan et al25 reported that diarrhea occurred in 21% of patients. In another large cohort of 651 patients infected with SARS‑CoV‑2 from the Zhejiang province, 11.4% presented with at least 1 digestive symptom, including nausea, vomiting, and diarrhea.26
Moreover, in a systematic review and meta‑analysis of 60 studies, including 4243 patients, the pooled prevalence of digestive manifestations in COVID‑19 was 18%. Loss of appetite was the most frequent one, followed by diarrhea, nausea or vomiting, and abdominal pain and/or discomfort.27
Liver injury is another possible digestive manifestation of COVID‑19, although data in this respect are more scarce and controversial. The most commonly reported hepatic abnormalities include elevated levels of aspartate aminotransferase and alanine aminotransferase, seen in 20% to 40% of patients, as well as high total bilirubin levels, found in approximately 10% of COVID‑19 cases.21,22 Whether liver injury is directly related to SARS‑CoV‑2 infection or secondary to systemic inflammation and/or drug toxicity remains unclear.22
All the above mentioned data on the occurrence of gastrointestinal COVID‑19 manifestations come from China, but we expect to obtain similar results from other countries due to the dynamic spread of SARS‑CoV‑2 infection worldwide. Interestingly, the first patient diagnosed with COVID‑19 in the United States initially complained of subjective fever, dry cough, nausea, and vomiting, and then developed diarrhea accompanied by abdominal discomfort.28 Recently, Nobel et al29 published the first case‑control study on the gastrointestinal symptoms in COVID‑19 in a large cohort from the United States. In a multivariable analysis, they showed that digestive symptoms were associated with a 70% risk of testing positive for SARS‑CoV‑2. They found that 35% of patients had gastrointestinal manifestations, and they were related to longer disease duration and lower mortality in a short‑term follow‑up.29 Also the first patient diagnosed with COVID‑19 in Poland had gastrointestinal symptoms as a first clinical presentation of SARS‑CoV‑2 infection.30
Similarly, our initial experience shows a relatively high frequency of digestive manifestations in patients with COVID‑19. To date, more than 30 patients were hospitalized in our 2 centers in Poznań and Warsaw and we estimate that up to 25% of them reported a variety of gastrointestinal symptoms. Moreover, in a 78‑year‑old male kidney transplant recipient with multiple comorbidities, diarrhea was the only possible manifestation of COVID‑19, and the disease course was mild and uneventful (Mahadea et al, unpublished data).
Although there is a growing body of evidence that digestive manifestations of COVID‑19 are of key importance, little is known about the exact pathomechanisms underlying this finding. There are only single reports on possible alterations to the gastrointestinal tract caused by SARS‑CoV‑2 infection. Liu et al31 presented autopsy findings of a patient who died of COVID‑19—an 85‑year‑old man in whom a small intestinal segmental dilatation and stenosis were noted. However, it needs to be clarified whether these findings were coincidental or not. Xiao et al16 tested patients infected with SARS‑CoV‑2 for the presence of viral RNA in urine, stool, and tissues. Biopsies of different parts of the gastrointestinal tract were performed in 1 patient, a 78‑year‑old man with confirmed COVID‑19 who underwent gastroscopy and colonoscopy due to gastrointestinal bleeding. Gastroscopy revealed mucosal lesions in the esophagus, whereas no macroscopic abnormalities were found in other parts of the digestive tract (the stomach, the duodenum, and the colon). Histopathological examination showed no significant lesions except for occasional lymphoplasmacytic infiltrates associated with interstitial edema in the esophageal squamous epithelium, the lamina propria of the stomach, the duodenum, and the rectum. Immunofluorescent staining revealed the expression of the viral nucleocapsid protein and ACE2, mainly in the glandular gastric, duodenal, and rectal epithelial cells. A very weak expression of ACE2 and lack of nucleocapsid protein expression were observed in the esophageal epithelium. The authors declared that they were able to detect ACE2 and SARS‑CoV‑2 in gastrointestinal tissues of other patients, but they have not published these findings yet.
These very limited data do not explain the mechanisms underlying digestive symptoms in COVID‑19 and results of further studies are much awaited. On the other hand, the absence of significant macro- and microscopic abnormalities is in line with the observations reported in patients with SARS.13 Moreover, it is also in accordance with the mild course of gastrointestinal symptoms in COVID‑19. Although diarrhea, abdominal pain, nausea, or vomiting are relatively frequently reported in the majority of studies on the clinical profile of COVID‑19, these digestive manifestations are of mild or moderate intensity.32
There are only a few speculative concepts on the pathophysiological background of these symptoms. Zhou et al33 suggested that it could be mainly related to the disturbances in the gut–brain axis. They hypothesized that the increased permeability of the intestinal barrier could lead to enhanced exposure of the central nervous system to harmful metabolites synthesized in the gut lumen. Another hypothetical explanation could be associated with the impairment of ACE2‑mediated intestinal homeostasis. As previously discussed, the downregulation of ACE2 expression in the lungs, resulting from SARS‑CoV infection, seems to mediate severe tissue injury.13 The role of ACE2 in the gastrointestinal tract is still being explored. It was shown, however, that ACE2 regulates intestinal amino acid homeostasis, modulates gut microbiota, and influences the expression of antimicrobial peptides.34 Assuming that SARS‑CoV‑2 infection is capable of downregulating ACE2 expression in various tissues, it could lead to dysbiosis and low‑grade inflammation in the gastrointestinal tract, resembling phenomena observed in irritable bowel syndrome and other functional digestive disorders.35 It cannot also be excluded that concomitant medications used in the treatment of COVID‑19 could partly contribute to the gastrointestinal symptoms. On one hand, azithromycin, lopinavir, and ritonavir are relatively frequently associated with side effects like diarrhea, abdominal pain, or nausea.36,37 On the other hand, in the case of hydroxychloroquine and chloroquine, gastrointestinal complaints are rare and mild.38 Tocilizumab, a recombinant humanized monoclonal antibody against the human interleukin‑6 receptor, and remdesivir, a nucleotide analogue prodrug inhibiting viral RNA polymerase, are considered potentially hepatotoxic drugs.39,40 Nevertheless, it seems that these medications are not the main cause of digestive symptoms in various cohorts of patients with COVID‑19, because, in the majority of studies, these manifestations were reported on admission and before starting any therapy against SARS‑CoV‑2. Moreover, Wan et al25 showed that the frequency of diarrhea during the course of the disease was not associated with the use of antiviral medications and antibiotics.
What are the practical implications of the above mentioned data on the gastrointestinal manifestations of SARS‑CoV‑2 infection? Single attempts have been made to assess whether patients with coexisting digestive symptoms differ from those without them regarding the clinical course of COVID‑19.24-26,29,32 Unfortunately, the results of these studies are inconclusive. Wan et al25 suggested that patients with diarrhea had more severe symptoms of pneumonia than those not showing this symptom. Diarrhea was also found to be associated with the need for ventilator support and admission to the intensive care unit. Jin et al26 reported a more severe and/or critical course of COVID‑19 and increased family clustering in patients with gastrointestinal symptoms. Higher rates of fever higher than 38.5 °C, fatigue, shortness of breath, and headache also characterized this subgroup of patients infected with of SARS‑CoV‑2. Some authors also suggested that the need for treatment in intensive care units was associated with liver injury.32 However, this observation seems to be unspecific. In contrast to the data discussed above, a case‑control study from the United States revealed that digestive symptoms in patients with COVID‑19 were related to a mild course of the disease and lower mortality.29
What is of paramount importance to clinicians, the clinical picture of COVID‑19 can be more differentiated than expected. Interestingly, according to a large survey performed by the Chinese Society of Gastroenterology, the awareness of the digestive aspects of COVID‑19 was low even among physicians dealing with gastrointestinal disorders.32 These results were followed by several initiatives of the Chinese Society of Gastroenterology aimed at improving this situation (publication of guidelines or recommendations, launching a dedicated online platform to share clinical experience among gastroenterologists from the Hubei province and other regions of China).
Every clinician must be aware that up to 50% of patients infected with SARS‑CoV‑2 report gastrointestinal symptoms. There is a growing body of evidence showing that digestive manifestations are particularly frequent on the first days of the disease. In one‑tenth of all COVID‑19 cases, they can precede typical respiratory symptoms.5,24,30 Siddiqi et al41 proposed a 3‑stage COVID‑19 classification system, which reflects different pathophysiological and clinical phases of the condition. They suggested that gastrointestinal symptoms occur typically at the stage of early infection and, to some extent, in the pulmonary phase. Some proportion of patients will progress into the third phase of the host inflammatory response, in which digestive manifestations are rare. Acute respiratory distress syndrome, severe inflammatory response syndrome, shock, and heart failure are typical presentations of this most severe stage.
That is why it is advised to pay much attention to patients reporting unspecific new‑onset gastrointestinal complaints in order not to overlook this subgroup of individuals infected with SARS‑CoV‑2 in the early phase of the disease. Indeed, a study from 3 hospitals in the Hubei province showed that patients with initial digestive symptoms had a significantly longer time from the disease onset to hospital admission.24
Fecal‑oral transmission of severe acute respiratory syndrome coronavirus 2: is it possible and does it matter?
It has been shown that both SARS‑CoV and MERS‑CoV can be isolated from the stool as a result of enteric involvement. However, it is believed that clinically relevant fecal‑oral transmission is not possible.42 The RNA of SARS‑CoV is detectable in feces from the fifth day of the disease onset, with a subsequent increase in viral load in the next couple of days.42 In a minority of patients, viral RNA was present in the stool even 1 month after SARS resolution. In the case of SARS‑CoV‑2, there is also a growing body of evidence for the presence of its nucleic acid in the stool. Xiao et al16 collected different specimens (serum, urine, oro- and nasopharyngeal swabs, and stool) from 73 patients with COVID‑19. They found that more than a half of them (53.4%) were positive for fecal SARS‑CoV‑2 RNA for 1 day to 12 days. In more than 20% of cases, the viral RNA was detectable in the stool even after the conversion of molecular tests, performed on the oro- and nasopharyngeal swabs, to negative. This is in line with other reports from China and the United States, which showed similar results.6,27,28,43
These data suggest that gastrointestinal symptoms in COVID‑19 are not accidental findings and they are secondary to direct digestive involvement. The main question remains whether this means that fecal‑oral transmission of SARS‑CoV‑2 is possible or not. Detection of viral RNA in the stool does not necessarily imply its infectivity, as it was shown in the case of SARS‑CoV or MERS‑CoV.32,42 It seems that only complete, live SARS‑CoV‑2 virions have the infectious potential. To date, any confirmed data on the infectivity of SARS‑CoV‑2 detected in the stool are available. However, Xiao et al16 together with the staff of other laboratories in China declared that they were able to isolate live, infectious virions from the stool of patients with COVID‑19, but these data have not been published yet (Xiao et al, unpublished data).
Nevertheless, even assuming that it is possible to detect fully virulent SARS‑CoV‑2 in the stool, it remains unclear whether the digestive tract can be a potential route of systemic disease. In the case of other coronaviruses, fecal MERS‑CoV does not seem to have the infectious potential. However, it was suggested in an animal model that oral transmission of live virions could cause infection not only in the digestive tract but also in other organs.44 Namely, Zhou et al44 showed that intragastric inoculation of MERS‑CoV resulted in intestinal inflammation progressing to systemic disease, including respiratory infection. Regarding SARS‑CoV‑2, Zhang et al7 analyzed various datasets with single‑cell transcriptomes of the lung, the esophagus, the stomach, the ileum, and the colon. They performed complex bioinformatics analysis suggesting that the gastrointestinal tract can be a possible transmission route of SARS‑CoV‑2 infection; however, this hypothesis needs to be confirmed in further studies.
In light of these data, we cannot currently exclude the possibility of the fecal‑oral transmission of SARS‑CoV‑2 and we have to take appropriate precautions to prevent virus shedding via this route. This is of paramount importance, because it was suggested that SARS‑CoV‑2 could be stable and viable on plastic or stainless steel after 72 hours.45 It is still debatable whether this should be considered while defining the criteria for discharging patients with COVID‑19 from the hospital or ending home isolation.32 The majority of guidelines on de‑isolation recommend discharging the patient after long‑standing, significant clinical improvement followed by 2 negative results of reverse transcriptase–polymerase chain reaction tests for SARS‑CoV‑2 performed at 24‑hour intervals.46 Since the significance of fecal‑oral transmission is not fully determined, it is advised that all discharged patients should strictly follow personal hygiene precautions.
Guidelines of associations in the field of gastroenterology in the context of the coronavirus disease 2019 pandemic
The COVID‑19 pandemic causes reasonable concern, both among patients and physicians. The pandemic is developing very rapidly around the world and has a significant impact on social life as well as on healthcare systems in almost every country. Being aware of the great significance of the problem, many scientific societies in the field of gastroenterology issued recommendations regarding the diagnostic workup and management of patients with digestive disorders. Here, we present a summary of the most important information covered in position statements and guidelines published by the British Society of Gastroenterology (BSG), European Crohn’s and Colitis Organization (ECCO), Polish Society of Gastroenterology (PSG), American Gastroenterological Association (AGA), European Association for the Study of the Liver (EASL), European Society of Clinical Microbiology and Infectious Diseases (ESCMID), and European Society of Gastrointestinal Endoscopy and European Society of Gastroenterology and Endoscopy Nurses and Associates (ESGE and ESGENA).47-56 All of them are based on guidelines for the management of other similar infections and experience of countries previously affected by the COVID‑19 pandemic. As the epidemiological situation is very dynamic, these recommendations can change frequently. Therefore, it is essential to follow their updates on the websites of the organizations.
Inflammatory bowel diseases
Among all gastroenterological patients, those with inflammatory bowel disease (IBD) constitute a specific group. They are often treated with immunosuppressants, so the risk of infection is a serious problem. As SARS‑CoV‑2 appeared only a few months ago, it is difficult to make specific observations regarding the impact of COVID‑19 on the course of IBD and the effect of drugs used for the treatment of IBD on the course of infection.47 Little is known as to whether recovery from COVID‑19 gives long‑lasting immunity and how the immunosuppressive treatment influences this state.47,48
We present the most important conclusions put forward in the position statements published by ECCO and BSG.47-50 Based on these information sources, numerous local recommendations were formulated, adapting the general principles to local conditions.51
Due to the high infectivity of the virus, it is very important to ensure an adequate level of social isolation in patients with IBD, both in everyday life and when providing healthcare services.47,51 Direct contact with other people, particularly with healthcare providers and those with suspicious symptoms, seems to be the most significant risk factor for SARS‑CoV‑2 infection.47,48,51 It was also demonstrated that the period of increased infectivity may fall before the onset of clinical symptoms.48 That is why it is crucial to limit the need for direct contact between patients and healthcare centers, both in hospitals and ambulatory care clinics.47,51
Regarding the reorganization of healthcare facilities, it is recommended to limit personal visits of patients with IBD in clinical remission or with symptoms of mild exacerbation, who can be diagnosed and treated on an outpatient basis. In such situations, it is advised to create a system of virtual visits, which will help to maintain continuity of care and to reduce patients’ exposure to infection.47,51 Patients have many doubts and questions about their treatment and risks arising from IBD. A conversation with a professional can help to dispel doubts and avoid treatment mistakes.
If possible, endoscopic examinations should be postponed, and other diagnostic procedures should be limited in favor of noninvasive testing, eg, abdominal ultrasound and measurement of fecal calprotectin concentration.47,51 If the patient’s visit in the center is necessary, it is recommended to separate the admission zone from the zone with potentially infected patients. This applies particularly to patients receiving biological treatment with intravenous infusions.
Each personal visit should be preceded by a medical interview regarding any suspicious symptoms of respiratory tract infection and measurement of body temperature.47,51 If symptoms are present, the patient’s visit in the gastroenterological center should be postponed and appropriate diagnostic workup, treatment, or isolation should be advised in line with local guidelines. In patients in remission who receive biological treatment, the dosing interval should be prolonged until the infection resolves.47-51 It is difficult to determine the safe time from the resolution of infection symptoms to administering the next dose. A generally accepted quarantine period of 2 weeks should be considered sufficient.47,51 However, as new data become available, these recommendations may change. The above principles apply for both confirmed cases of COVID‑19 and patients with respiratory tract infections who have not been tested for SARS‑CoV‑2 or whose results were negative.47,51
Treatment of patients in clinical remission should be maintained, even if based on immunosuppressive drugs.47-51 The risk of infection associated with disease exacerbation far outweighs the risk of treatment, except for high‑dose steroids (rapid reduction or the use of locally acting preparations are recommended) and immunosuppressive medications taken by the elderly or those with comorbidities (withdrawal should be discussed).47,51 The use of medications that can be administered at home instead of intravenous forms requiring hospitalization can be also considered. In particular, this refers to biological drugs administered subcutaneously compared with intravenous drugs. This advice applies to starting new therapies and changing those already implemented only because the route of administration is not recommended.47,51 Since there are still many unknowns, essential decisions should be made by an interdisciplinary team.
Patients should strictly follow the recommendations of national sanitary departments. They stipulate special protection (called “shielding”) for people at high risk of developing infection and a severe course of the disease.47,51 According to BSG, this group includes patients with IBD and comorbidities, older people treated with immunosuppressive drugs, taking high doses of steroids, and all those with moderate‑to‑severe disease activity despite immunosuppression and/or use of biologics.47 Other patients should adhere to the principle of social isolation or distancing, which is particularly strict for patients on immunosuppressive therapy. Patients should not change treatment regimens without consulting their physicians.47,51,52
Liver diseases
It remains unclear whether SARS‑CoV‑2 infection may aggravate chronic liver diseases. Nevertheless, patients with advanced liver diseases, particularly in the exacerbation phase, and transplant recipients are at high risk of developing a severe course of COVID‑19.53 General recommendations for the management of such diseases as well as for the organization of healthcare are similar to those for IBD. Immunosuppressive treatment in autoimmune hepatitis should be continued.53 Patients qualified for transplants and donors should be routinely tested for SARS‑CoV‑2 before the procedure.53 Living‑donor transplants should be considered on a case‑by‑case basis. In transplant recipients, discontinuation of immunosuppressive therapy is not advised.53
The most relevant conclusions presented in the position statements and guidelines on the diagnostic workup and management of IBD and liver disorders during the COVID‑19 pandemic are summarized in Table 2.
Abbreviations: COVID‑19, coronavirus disease 2019; IBD, inflammatory bowel disease; SARS‑CoV‑2, severe acute respiratory syndrome coronavirus 2 |
• Inform your patients about the need for maintaining an appropriate level of social isolation and/or distancing.
• Reduce the patient’s personal contact with the hospital to a minimum.
• Ensure that your patients can easily contact a member of the IBD and/or liver disease team virtually.
• Conduct a triage before each patient’s visit in the center.
• Patients in clinical remission should continue their current treatment (except for the elderly or patients with comorbidities in whom discontinuation of immunosuppressive therapy may be considered).
• The risk associated with immunosuppressive treatment and of disease exacerbation should always be balanced.
• Avoid high doses of steroids.
• When starting a new biological therapy, consider treatment with subcutaneous instead of intravenous drugs.
• Postpone the next dose of a biologic drug if the patient has symptoms of respiratory tract infection until they resolve; a 2‑week quarantine period is considered sufficient.
• If in doubt, perform a test for SARS‑CoV‑2.
• Pay attention to the unusual symptoms and course of COVID‑19 in immunosuppressive patients.
• Guidelines change very quickly. Follow the websites of scientific societies. |
Gastrointestinal endoscopy
Performing endoscopy during the COVID‑19 pandemic is another problem in daily gastroenterological practice. Inhalation of airborne droplets, aerosols, and direct contact with contaminated surfaces increase the risk of infection during endoscopic procedures.54 To minimize this risk in healthcare professionals and to reduce the probability of shedding SARS‑CoV‑2 among patients in the endoscopy unit, many national and international societies have issued dedicated recommendations.54-56 They contain guidelines on the appropriate qualification of patients for endoscopic procedures and proper management when performing them.
Patients’ qualification for endoscopic procedures should be based on verifying indications and assessing the risk of SARS‑CoV‑2 infection. It is recommended to postpone all planned procedures, as long as it does not affect patients’ health.54,55 This includes, for example, screening for bowel cancer, surveillance for IBD or Barrett esophagus. On the other hand, procedures such as oncological diagnostic workup and treatment, diagnosis of alarm symptoms, continuation of treatment necessary in the planned period (eg, secondary prophylaxis of esophageal variceal bleeding or removal of self‑expandable stents) should be performed by personnel wearing appropriate protective equipment after prior risk stratification for COVID‑19.54-56
The patient’s visit in the endoscopy unit should be preceded by a medical interview aimed to gather information on possible respiratory tract infection and contact with persons with COVID‑19, preferably by phone the day before the examination.54-56 Triage applies not only to patients but also to the endoscopy unit staff.54 Endoscopists and endoscopy nurses must be familiar with the infection prevention and control strategy for COVID‑19, as well as with the proper use of personal protective equipment (PPE).54-56 Risk stratification should be repeated on the day of the endoscopic procedure. It is recommended that patients in the unit wear surgical masks at all times.
Considering droplet transmission of the virus, endoscopy of the upper gastrointestinal tract is believed to be the procedure of the highest risk. Despite this, the ESGE and ESGENA guidelines recommend to wear the same PPE during all procedures.54
The minimum PPE for procedures performed in low‑risk patients includes surgical masks, gloves, disposable hairnets, protective eyewear (goggles or disposable face shields), and waterproof disposable gowns.54-56 For high‑risk patients or those with confirmed infection: respiratory PPE (FFP2/FFP3 masks), 2 pairs of gloves, a disposable hairnet, protective eyewear (goggles or a disposable face shield), a waterproof disposable gown, and foot cover. It should be emphasized that it is advisable to perform the procedures in this group of patients only if there are urgent indications for doing so: in the case of gastrointestinal bleeding, esophageal food impaction, or severe acute pancreatitis with acute calculous cholangitis.54-56
The key conclusions drawn from position statements and guidelines on the gastrointestinal endoscopy during the COVID‑19 pandemic are summarized in Table 3.
Abbreviations: FFP, filtering facepiece; PPE, personal protective equipment; others, see Table 2 |
• Endoscopy belongs to procedures posing a high risk of SARS‑CoV‑2 infection.
• Postpone planned procedures.
• Verify the urgency of the endoscopy.
• Assess the risk of SARS‑CoV‑2 infection.
• Make sure that you and the whole team are well trained in using PPE.
• Use appropriate PPE regardless of the type of procedure:
− For low‑risk patients: a surgical mask, gloves, a disposable hairnet, protective eyewear (goggles or a disposable face shield), and a waterproof disposable gown
− For high‑risk patients or those with confirmed COVID‑19: respiratory PPE (an FFP2/FFP3 mask), 2 pairs of gloves, a disposable hairnet, protective eyewear (goggles or a disposable face shield), a waterproof disposable gown, and foot cover |
Conclusions
The emergence of COVID‑19 has become the biggest challenge for the whole human community since many years. Our knowledge of the clinical course and progress in the diagnostic workup and treatment of COVID‑19 are still increasing. However, we have to pay much attention to distinguish high‑quality research from “fake science,” as numerous studies on COVID‑19 are published before completion of the peer‑review process.57,58
Unfortunately, although healthcare providers, scientists, politicians, and societies of countries affected by the disease are making many attempts to fight the disease, we are still far away from overcoming the pandemic.59,60 It seems that appropriate identification of all people infected with SARS‑CoV‑2 is the best strategy to limit disease transmission and to protect those who are at high risk of developing a severe course of COVID‑19.61 This is, however, very difficult, since there are no clinical manifestations of the disease or symptoms are very mild or atypical in a significant proportion of patients.61
Digestive manifestations of COVID‑19 seem to occur most frequently, apart from typical respiratory symptoms. That is why it is essential to bear in mind that a patient with new‑onset diarrhea, abdominal pain, nausea, and vomiting without any other evident etiological factors should be tested for SARS‑CoV‑2 infection. This is of particular importance to gastroenterologists, because the differential diagnosis of the symptoms mentioned above is the main task in their everyday practice.
Gastroenterologists and members of other medical specialties should also remember that the current epidemiological situation has changed diagnostic and therapeutic algorithms in the management of several gastrointestinal and liver disorders. Depending on how efficiently the humanity overcomes the COVID‑19 pandemic, it will turn out whether these changes will be only temporary.
- Guan W, Ni Zhu Y, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020; 382: 1708‑1720.
- Andersen KG, Rambaut A, Lipkin WI, et al. The proximal origin of SARS‑CoV‑2. Nat Med. 2020; 26: 450‑452. | Crossref
- COVID‑19 coronavirus pandemic Worldometers website. https://www.worldometers.info/coronavirus/. Accessed April 19, 2020.
- Zhou P, Yang XL, Wang XG, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature. 2020; 579: 270‑275.
- Luo S, Zhang X, Xu H. Don’t overlook digestive symptoms in patients with 2019 novel coronavirus disease (COVID‑19). Clin Gastroenterol Hepatol. 2020 Mar 18. . | Crossref
ARTICLE INFORMATION