Association of muscular strength with pulsatile and steady hemodynamics in patients with acute myocardial infarction
Key words: aortic characteristic impedance, arterial load, grip, pulsatile hemodynamics



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Association of muscular strength with pulsatile and steady hemodynamics in patients with acute myocardial infarction
Introduction: Grip strength and blood pressure are strongly interrelated. Blood pressure is an essential component of arterial load, which modulates cardiac output.
Objectives: We aimed to asses the correlation between grip strength and both steady and pulsatile components of arterial load in patients with acute myocardial infarction.
Patients and methods: We included 295 participants (mean age, 63 years) with acute myocardial infarction. The following data were assessed: grip strength, echocardiography, local arterial stiffness, arterial tonometry, continuous arterial pulse, and beat‑to‑beat wave.
Results: In univariable analyses, grip strength correlated with arterial stiffness (pulse wave velocity), ventricular–arterial coupling, and measures of pulsatile arterial load: aortic characteristic impedance (Zao), total arterial compliance (TAC), and central fractional arterial pulse pressure (cFPP). In a multivariable model including age, grip strength, body mass index, systolic blood pressure, sex, and descriptors of pulsatile load, the following remained associated with grip strength: Zao (R2 for the model = 0.58; P <0.001), TAC (R2 = 0.23 for the model; P <0.001), and cFPP (R2 for the model = 0.2; P <0.001). In the second model that included sex, only Zao remained associated with grip strength (R2 for the model = 0.67). Comparisons between men and women of the adjusted mean value demonstrated that Zao and cFPP were considerably higher (P <0.001 and P = 0.02, respectively) and TAC was lower in women (P <0.001).
Conclusions: In a cohort of patients with acute myocardial infarction, grip strength correlated independently and significantly with descriptors of the pulsatile arterial load. The role of sex in these interrelations needs further study.
What's new?
The oscillatory properties of blood pressure and flow are best assessed by estimating aortic impedance. This marker was firmly, independently, and negatively associated with grip strength. Patients with greater grip strength may represent a more favorable hemodynamic trait.
Introduction
The grip strength test serves as a tool that predicts muscular strength as well as endurance. It is also a prognostic marker associated with diabetes, cardiovascular events and mortality.1-3 A recent patient data pooled meta‑analysis showed that in patients with cardiac disorders, grip strength predicted cardiac death, all‑cause death, and hospitalization due to heart failure.4 A Mendelian randomization study investigating the causal relationship between grip and health outcomes demonstrated that a 1‑kg increase in genetically determined grip strength reduced the odds ratio of coronary artery disease by 6% and the odds ratio of myocardial infarction (MI) by 7%.5 Muscle strength seems to be a significant determinant of the blood pressure (BP) response to isometric stress.6 Blood pressure is an essential component of arterial load (AL), which modulates cardiac output. Hemodynamic load on the left ventricle may contribute to a higher risk of cardiac events, particularly in patients with structural heart disease.7 Our study aimed to obtain mechanistic insight into the possible association between muscle strength and AL. We investigated the correlation between grip and aortic characteristic impedance (Zao), total arterial compliance (TAC), ventricular–arterial (VA) coupling, central fractional pulse pressure (cFPP), ejection fraction (EF), and arterial stiffness in a cohort of patients with acute MI.
Patients and methods
Consecutive patients referred for percutaneous coronary intervention (PCI) due to acute myocardial infarction (MI) such as non–ST‑segment elevation MI and ST‑segment elevation MI and presenting with more than 50% of coronary artery narrowing were included in the study. Patients with cardiogenic shock, advanced and refractory chronic heart failure, atrial fibrillation or flutter, chronic kidney disease on dialysis were excluded. All study patients underwent immediate coronary angiography, and PCI was attempted in the infarct‑related artery. Hemodynamic assessments were performed between 72 to 96 hours after admission.
Written informed consent was obtained from all patients prior to their inclusion in the study. This study was approved by the ethics committee of the Poznan University of Medical Sciences, and the study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki with later amendments.
Echocardiography
All patients underwent complete 2‑dimensional and Doppler echocardiography using an ultrasound system (MyLab Class C, Esaote, Genoa, Italy) with a 3‑MHz transducer. Left ventricular volume and EF were estimated using a modified biplane Simpson method based on 3 measurements.8
Ventricular–arterial coupling
To determine the end‑systolic pressure–volume relationship by the single‑beat technique described by Chen et al,9 left ventricular end‑systolic pressure, stroke volume, and timing intervals (total ejection time, pre‑ejection time, total systolic period) were measured for left ventricular end‑systolic elastance (stiffness) calculation. Effective arterial elastance was calculated as end‑systolic pressure (obtained from the formula 0.9 × [systolic BP] as estimated by cuff measurement at the brachial artery divided by stroke volume). Arterial elastance was divided by end‑systolic elastance, which represents the VA coupling ratio (arterial elastance / end‑systolic elastance).
Total arterial compliance
To obtain TAC, stroke volume was divided by central pulse pressure (systolic BP – diastolic BP). Results are shown as ml/mm Hg.
Local arterial (carotid) stiffness
The left common carotid artery was examined using a high‑resolution linear probe operating at 4 to 13 MHz (MyLab Class C). Brachial BP was obtained using the oscillometric method (M‑705IT; Omron Healthcare Co., Ltd., Kyoto, Japan) after a 5‑minute rest. All investigations were performed with the patient in the supine position with head elevation. The common carotid artery 1 cm before the bulb was used for measurements. All measurements were performed with the dedicated ArtLab software (Esaote, Genoa, Italy) using radiofrequency data technology (QASRF [Quality Arterial Stiffness by radiofrequency tracking method] for arterial stiffness). The system cyclically determines 6 consecutive measurements of both the arterial distension and diameter (with SD <35 µm). Local arterial stiffness is presented as pulse wave velocity (PWV) in m/s.
Determination of the central fractional pulse pressure
The radial pressure waveform was obtained noninvasively, using a piezoelectric tonometer (Colin BPM 7000, Colin Medical Instruments, Komaki, Japan) for automatic artery wave detection and recording. The recorded analog signal was sent to SphygmoCor Mx (AtCor Medical, Sydney, Australia) for online reconstruction (with the use of a validated transfer function) of pressure waveform characteristics for the ascending aorta. Pulse wave analysis was applied to assess the peripheral and central hemodynamics. Central pulse pressure (systolic BP – diastolic BP) was divided by mean BP to estimate the cFPP.
Estimation of aortic characteristic impedance
Continuous finger arterial pulse, beat‑to‑beat wave 30‑minute registration was performed by Portapres (TNO‑TPD, Finapres Medical Systems, Amsterdam, the Netherlands) with the patient in the semi‑Fowler position. Zao was obtained by the Modelflow method. Zao is presented in mm Hg × s/ml.
Grip measurement
Patients were asked to perform the maximum grip trial in the standing position with the dominant arm, using the Jamar Hydraulic Hand Dynamometers (Sammons Preston Rolyan, Bolingbrook, Illinois). The best of 3 maximal isometric contractions was determined for each patient. Results are presented in kg.
Statistical analysis
All analyses were performed with SPSS (version 23.0, IBM Corp, Armonk, New York, United States). Continuous data are reported as mean (SD). All tests were 2‑tailed and P value of less than 0.05 was considered significant. The association between clinical variables was assessed with the Pearson correlation or partial correlation when controlling for age. Multivariable regression was used to assess the association of aortic input impedance, cFPP, and TAC with other clinical variables. The general linear model univariate procedure was used to estimate means adjusted for the covariate, and results are demonstrated as mean (SEM).
Results
The baseline characteristics of the study patients are presented in Table 1. The mean (SD) age was 63 (11) years. A total of 26% of patients had a history of MI, 79% had hypertension, 31% had diabetes, and 38% were current smokers. Successful PCI was performed in 80% of patients.
Clinical characteristics | Total (n = 295) | Women (n = 80) | Men (n = 215) |
Data are presented as number (percentage) unless otherwise indicated.
Abbreviations: MI, myocardial infarction; NSTEMI, non–ST‑segment elevation myocardial infarction; PCI, percutaneous coronary intervention; STEMI, ST‑segment elevation myocardial infarction | |||
STEMI / NSTEMI, n | 119/176 | 29/51 | 90/125 |
Current PCI | 235 (80) | 63 (79) | 172 (80) |
History of MI | 76 (26) | 16 (20) | 60 (28) |
Hypertension | 233 (79) | 71 (89) | 162 (75) |
Diabetes | 90 (31) | 35 (44) | 55 (26) |
Current tobacco use | 113 (38) | 35 (44) | 78 (36) |
The hemodynamic characteristics are demonstrated in Table 2. The mean systolic and diastolic BP, as well as mean EF, were within the normal range. Grip strength, peripheral systolic BP, peripheral diastolic BP, and TAC were significantly lower in women. On the other hand, cFPP pressure, Zao, and VA coupling were significantly higher in women.
Clinical variable | Total | Women | Men | P value |
Data are presented as mean (SD).
Abbreviations: BMI, body mass index; cFPP, central fractional pulse pressure; DBP, diastolic blood pressure; EF, ejection fraction; SBP, systolic blood pressure; TAC, total arterial compliance; PWV, pulse wave velocity; VA, ventricular–arterial; Zao, aortic characteristic input impedance | ||||
Age, y | 63 (11) | 65 (10) | 63 (11) | 0.05 |
BMI, kg/m2 | 28.5 (9.9) | 28.1 (5.5) | 27.9 (4.1) | 0.78 |
Grip strength, kg | 34.6 (12.9) | 21.8 (6.8) | 39.3 (11.3) | 0.001 |
Peripheral SBP, mm Hg | 115 (18) | 112 (18) | 116 (18) | 0.04 |
Peripheral DBP, mm Hg | 69 (12) | 64 (12) | 70 (11) | 0.001 |
cFPP | 0.42 (0.12) | 0.46 (0.15) | 0.4 (0.11) | 0.001 |
Zao, mm Hg × s/ml | 50.6 (8.6) | 58.9 (8.9) | 47.5 (5.9) | 0.001 |
TAC, ml/mm Hg | 1.41 (0.59) | 1.15 (0.6) | 1.51 (0.57) | 0.001 |
VA coupling | 1.68 (0.57) | 1.71 (0.62) | 1.67 (0.54) | 0.04 |
EF, % | 49 (12) | 52 (12) | 49 (12) | 0.12 |
PWV, m/s | 9.6 (2.4) | 9.7 (2.1) | 9.5 (2.5) | 0.61 |
Association between dynamometer grip strength and clinical as well as hemodynamic parameters
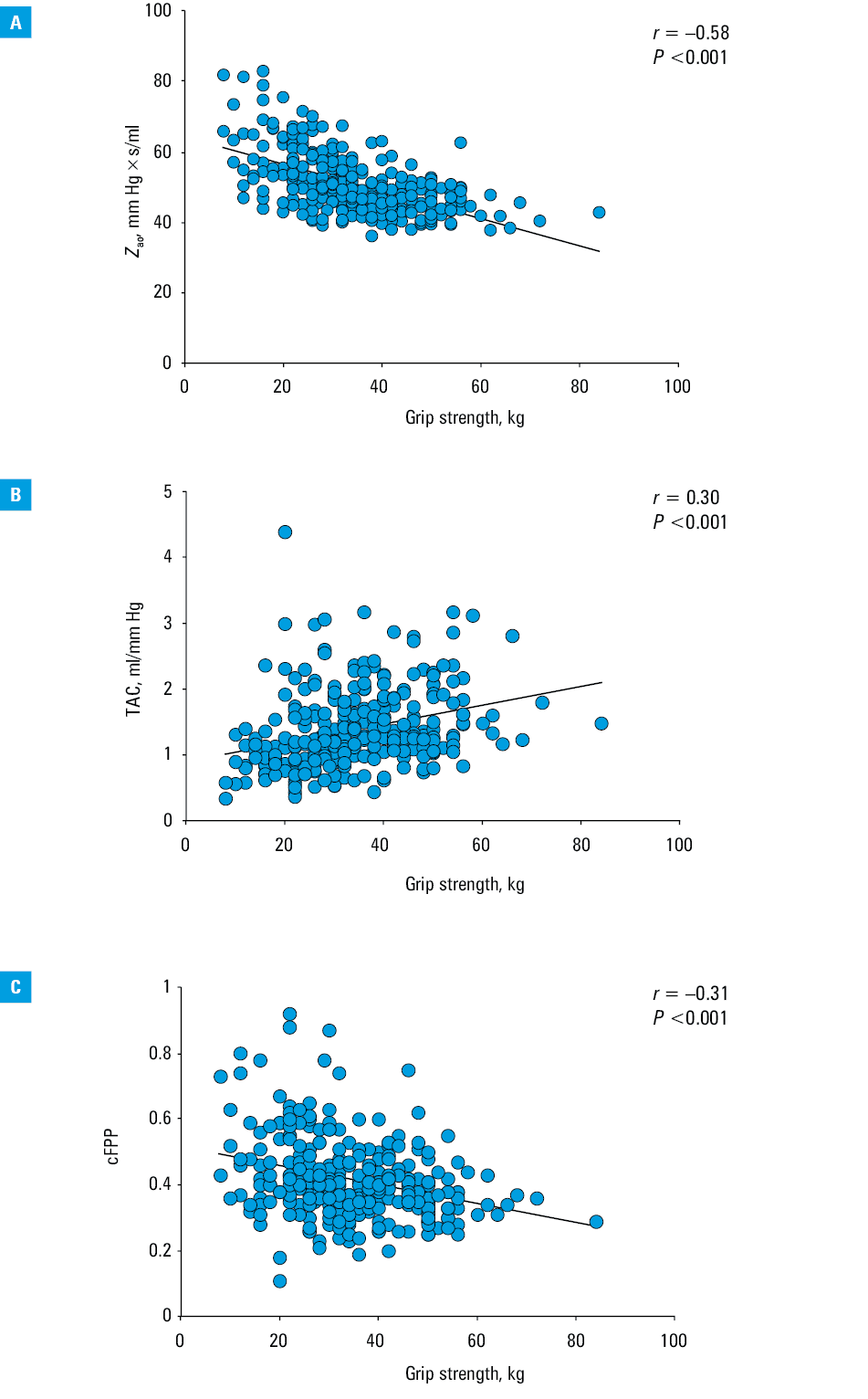
Grip strength in the study population correlated negatively and significantly with aortic input impedance (r = –0.58, P <0.001; Figure 1A), positively with TAC (r = 0.3, P <0.001; Figure 1B), negatively with the cFPP (r = –0.31, P <0.001; Figure 1C). Grip strength correlated negatively with age (r = –0.45, P <0.001), very weakly with VA coupling (r = –0.1, P = 0.04) and PWV (r = –0.16, P = 0.006), and did not correlate with EF (r = –0.03, P = 0.6), body mass index (BMI; r = 0.11, P = 0.06), or systolic BP (r = 0.06, P = 0.28). Partial correlation between grip and PWV or VA coupling was insignificant when controlling for age (data not shown).
Aortic input impedance was also significantly associated with age (r = 0.4, P <0.001), BMI (r = –0.45, P <0.001), PWV (r = 0.19, P = 0.002), and systolic BP (r = 0.23, P <0.001). Multiple linear regression showed that grip strength, age, BMI, systolic BP, but not PWV, were independently associated with aortic input impedance (model 1, Table 3). This model explained 56% variance in Zao.
Covariate | Zaoa | cFPPb | TACc | |||
Standardized coefficient | P value | Standardized coefficient | P value | Standardized coefficient | P value | |
a R2 = 0.56, P <0.001
b R2 = 0.2, P <0.001
c R2 = 0.23, P <0.001
Abbreviations: see Table 2 | ||||||
Grip strength | –0.48 | <0.001 | –0.18 | 0.004 | 0.19 | 0.002 |
Age | 2.35 | 0.02 | 0.27 | 0.001 | –0.29 | 0.001 |
BMI | –0.39 | <0.001 | –0.005 | 0.93 | –0.002 | 0.97 |
SBP | 6.17 | 0.02 | 0.036 | 0.51 | –0.15 | 0.005 |
PWV | 0.35 | 0.73 | 0.11 | 0.05 | –0.09 | 0.14 |
The multiple linear regression analysis demonstrated that grip strength, age, and systolic BP were independently associated with TAC (R2 = 0.23) while grip strength and age were independently associated with the cFPP (R2 = 0.2) (model 1, Table 3). In model 2, which included sex (women vs men) only Zao correlated independently and significantly with grip strength. This model explained 67% variance in Zao. Sex remained significantly and independently associated with Zao, cFPP, and TAC (model 2, Table 4).
Covariate | Zaoa | cFPPb | TACc | |||
Standardized coefficient | P value | Standardized coefficient | P value | Standardized coefficient | P value | |
a R2 = 0.67, P <0.001
b R2 = 0.26, P <0.001
c R2 = 0.39, P <0.001
Abbreviations: see Table 2 | ||||||
Grip strength | –0.12 | 0.01 | –0.08 | 0.28 | 0.02 | 0.74 |
Age | 0.21 | <0.001 | 0.27 | <0.001 | –0.29 | <0.001 |
BMI | –0.43 | <0.001 | –0.05 | 0.38 | 0.06 | 0.22 |
SBP | 0.14 | <0.001 | 0.26 | <0.001 | –0.45 | <0.001 |
PWV | 0.04 | 0.34 | 0.09 | 0.13 | –0.03 | 0.55 |
Sex | –0.52 | <0.001 | –0.17 | 0.01 | 0.28 | <0.001 |
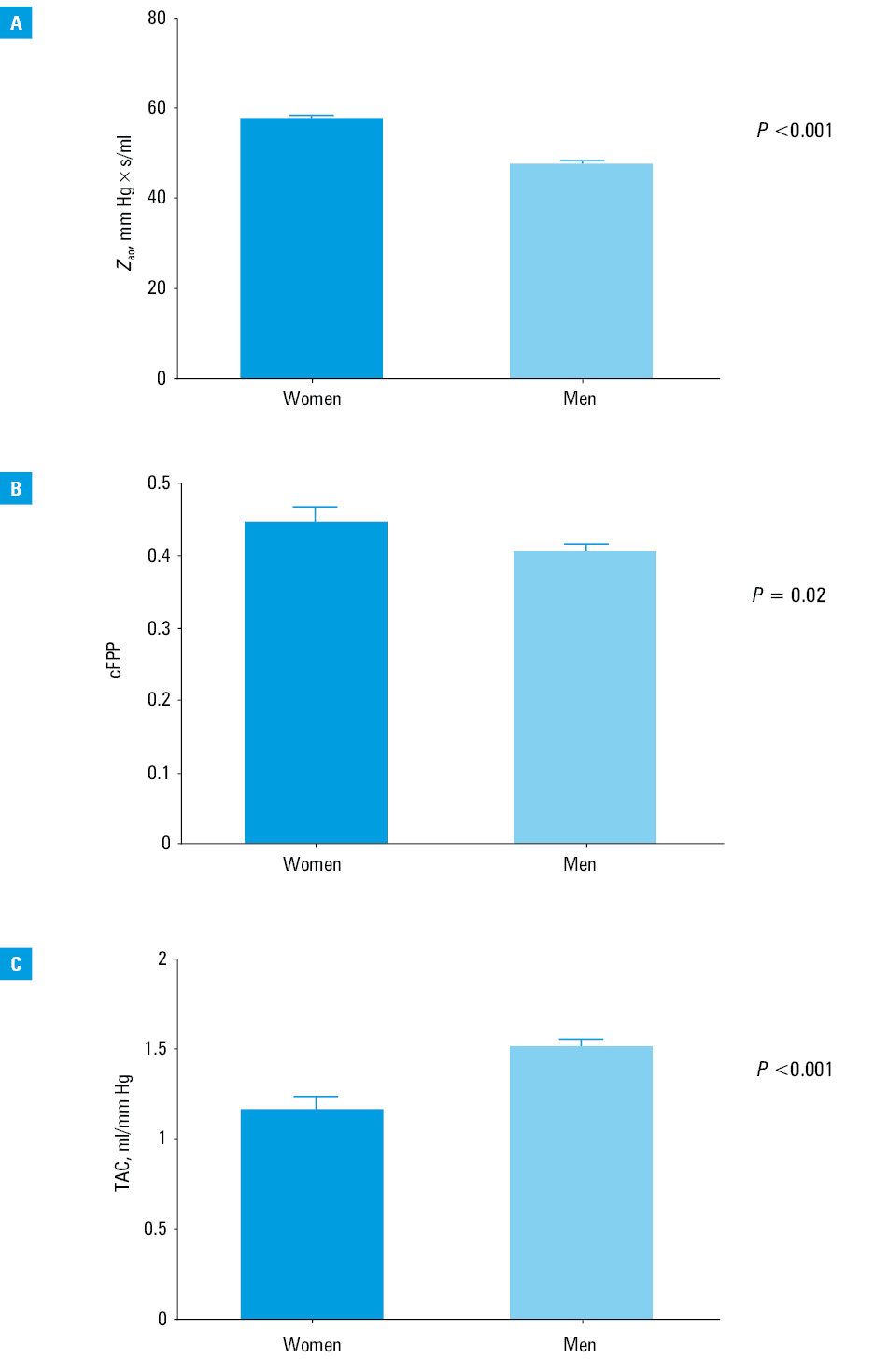
The Zao value was significantly higher in women than in men (mean [SE], 57.8 [0.7] vs 47.9 [0.4] mm Hg × s/ml; P <0.001) when compared after adjusting for age, BMI, systolic BP, arterial stiffness, and grip strength. Similar results were observed for the cFPP (mean [SE], 0.45 [0.02] vs 0.41 [0.008]; P = 0.02). In contrast, TAC was significantly lower in women than men (mean [SE], 1.16 [0.07] vs 1.51 [0.04] ml/mm Hg; P <0.001; Figure 2A–2C).
Discussion
Grip strength correlated independently and significantly with descriptors of pulsatile AL in a cohort of patients with acute MI. The association of sex with this interaction needs further study.
The grip strength test serves as a simple marker of overall muscular strength and a low result is associated with a host of adverse health outcomes. Grip maneuvers are performed very frequently during many everyday activities requiring holding and lifting up objects by hands. Grip strength is also a part of the diagnostic workup of frailty.10,11 Moreover, it was suggested that grip strength may serve as a proxy marker of sarcopenia. Thus, modifying this health burden might help prevent future complications.12 The increased AL imposed on the left ventricle due to an increase in BP, aging, left ventricle and aorta stiffening may contribute to the development of cardiovascular events such as, for example, heart failure, particularly in patients with prior myocardial insult. This cardiovascular mismatch may become apparent during the afterload challenge. Therefore, grip exercise is frequently used to unmask the abnormal left ventricular function or BP response.6,13,14 Flow generated by the left ventricle is opposed by the arterial system. These interactions are complex and consist of steady and pulsatile components of AL. Arterial load does not represent one specific property of the arterial system but is a combined descriptor of cardiac afterload. Various markers characterize both elements of AL. Systolic BP, systemic vascular resistance, arterial stiffness, cardiac output, stroke volume, or effective arterial elastance are usually used to depict steady components. Hemodynamic parameters describing pulsatile load include Zao, TAC, fractional pulse pressure, or pulse wave reflection.
Blood pressure is a well‑known risk factor for cardiovascular events, particularly in survivors of MI. Blanchard et al15 estimated the influence of resting BP on muscular strength. It was observed that adults with high BP displayed greater muscle strength than those with normal BP. The correlation between BP and grip was not estimated. Van Daele et al6 examined the BP response during submaximal grip and the determinants of grip strength. It was shown that higher baseline BP acted as an independent predictor of BP increase during grip. Moreover, grip strength itself was a predominant determinant of BP response. The authors concluded that grip strength should be accounted for in the future analysis. In our present study, grip strength did not correlate with systolic BP estimated from the brachial artery as well as by the beat‑to‑beat technique.
De Lima‑Junior et al16 demonstrated that grip strength was not associated with PWV in patients with hypertension. We showed that grip correlated weakly with arterial stiffness, but this association was not significant after correcting for age of study patients. A similar pattern of association was observed for correlation with VA coupling, an essential marker of cardiovascular interaction.17,18
Contrary to the relationship between grip strength and markers of steady components of AL, grip was significantly and independently correlated with pulsatile AL in our study cohort. Aortic characteristic impedance calculated from pressure and flow profiles was associated with left ventricular mass.19 Recently, an elevated pulse pressure in patients with systolic hypertension was attributed to an increase in Zao but not to enhanced aortic stiffness.20 It suggests that aortic function may play an active role in the pathophysiology of cardiovascular events beyond that attributed to the loss of elastin fiber integrity and increased proximal artery stiffness. We estimated Zao using the Modelflow method. The performed analysis showed that aortic impedance in survivors of MI was strongly and inversely correlated with grip strength. In the multivariable analysis, this association was independent of age, systolic BP, and BMI, which influenced aortic impedance in univariate correlation. Moreover, this model explains a large percent of the variability in aortic input impedance.
Reil et al21 demonstrated that effective treatment of patients with heart failure unload the left ventricle and improve (increase) TAC. We also observed that this index of pulsatile component of AL was significantly and independently increased in patients with stronger grip. Pulsatility of ascending aortic BP waveform, estimated as the cFPP, is associated with an increased risk of coronary artery disease and the presence of coronary artery narrowing.22 We observed that stronger grip is inversely and independently correlated with lower aortic pulsatility, estimated as the cFPP. Thus, whole evidence from our study indicates that grip strength is associated with descriptors of AL. However, the strongest and independent correlation exists between grip strength and pulsatile AL. Interestingly, grip strength was not associated with EF, which in turn remained within the normal range in our study population. VA coupling, a combined measure of left ventricular interaction with the arterial system, was also not correlated independently with grip strength.
Several studies reported sex differences in the physiological response to physical exercise.23,24 Joshi et al25 observed sexually dimorphic respiratory response to grip and postexercise circulatory occlusion. It is generally accepted that women and men differ in the clinical manifestation of cardiovascular diseases. In a recent analysis, Hongwei et al26 indicated that in contrast with the popular notion that cardiovascular disease in women lags behind men by 10 to 20 years, the early‑onset sexual dimorphism in BP measures exists. Moreover, these measures progress more rapidly in women than in men, beginning early in life. Although our study was not designed to test the hypothesis of sex differences in estimated associations, we showed that Zao, a significant marker of arterial pulsatility, was independently associated with grip strength even after adjustment for sex. Furthermore, sex was also an independent predictor of cFPP and TAC. We also observed a sex‑specific difference in the adjusted value of Zao, cFPP, and TAC. These observations confirm that sex plays an essential role in hemodynamic interrelations.
Most of the research concerning modifiable risk factors in cardiovascular events concentrates on BP, obesity, and / or body fat distribution but not on muscle mass or muscle strength. Despite a plethora of explanations on the potential mechanisms by which low grip strength predisposes to cardiovascular events, relatively little research is performed to estimate even mechanistic association between grip strength and cardiovascular descriptors of arterial or cardiac function. Our current study indicates that grip strength is correlated with pulsatile AL. Several studies assessing BP response to grip strength consistently demonstrated an increase in BP after grip maneuver. The oscillatory properties of BP and flow are best assessed by estimation of aortic impedance. This marker was firmly, independently, and negatively associated with grip strength. Thus, it is tempting to speculate that patients with greater grip strength may represent a more favorable hemodynamic trait.
Limitations and perspectives
Our study has several limitations. We did not estimate a dynamic response of hemodynamic markers after grip, which was mitigated by an early stage of acute MI. Our study was not well‑balanced to estimate sex‑specific correlations between grip value and descriptors of pulsatile and steady hemodynamics. Therefore, the role of sex in this interrelations needs further research. Another limitation of our study is that grip measurements were carried out in the standing position. Posture is known to affect cardiovascular response.27 Further studies should also address the relationship of hand muscle grip and strength of muscles in the legs and falls / orthostatic intolerance in patients with MI or older patients.28
We used the Modelflow method for the estimation of aortic input impedance. The evaluation of flow from pressure by the Modelflow method is based on the major properties of aorta and arterial system: Zao, Windkessel compliance, and peripheral resistance. This method is used mainly to estimate cardiac output from arterial pressure waveform and was tested for accuracy with Doppler echocardiography showing a reliable estimation of cardiac output.29 We are not aware of data showing the direct comparison of the Modelflow estimation of aortic impedance with the method based on a simultaneous assessment of pressure and flow in the aorta. Nevertheless, we are convinced that the association between aortic input impedance and grip strength will remain unchanged, despite the use of the different methods for Zao estimation. Moreover, one cannot exclude that improvement of physical fitness and muscle strength affects desirably pulsatile AL contributing to better health outcomes.
- Celis‑Morales CA, Lyall DM, Anderson J, et al. The association between physical activity and risk of mortality is modulated by grip strength and cardiorespiratory fitness: evidence from 498 135 UK‑Biobank participants. Eur Heart J. 2017; 38: 116‑122. | Crossref
- Izawa KP, Watanabe S, Osada N, et al. Handgrip strength as a predictor of prognosis in Japanese patients with congestive heart failure. Eur J Cardiovasc Prev Rehabil. 2009; 16: 21‑27. | Crossref
- Wander PL, Boyko EJ, Leonetti DL, et al. Greater hand‑grip strength predicts a lower risk of developing type 2 diabetes over 10 years in leaner Japanese Americans. Diabetes Res Clin Pract. 2011; 92: 261‑264. | Crossref
- Pavasini R, Serenelli M, Celis‑Morales CA, et al. Grip strength predicts cardiac adverse events in patients with cardiac disorders: an individual patient pooled meta‑analysis. Heart. 2019; 105: 834‑841. | Crossref
- Xu L, Hao YT. Effect of handgrip on coronary artery disease and myocardial infarction: a Mendelian randomization study. Sci Rep. 2017; 7: 954‑962. | Crossref
ARTICLE INFORMATION