Endoscopic narrow-band imaging for the diagnostic workup of intraductal papillary mucinous neoplasm with duodenal fistula



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Endoscopic narrow-band imaging for the diagnostic workup of intraductal papillary mucinous neoplasm with duodenal fistula
The Fukuoka guidelines state that imaging findings indicative of malignancy are high‑risk stigmata/worrisome features in the management of patients with intraductal papillary mucinous neoplasm (IPMN). However, a reliable diagnosis of malignancy is difficult.1 Direct visualization of IPMN by peroral pancreatoscopy is useful, yet challenging, for more accurate diagnosis. We report a rare case of IPMN with a duodenal fistula. In this case, we observed microvascular patterns of IPMN using narrow‑band imaging (NBI) in detail. The imaging characteristics identified in this case could facilitate the diagnosis of IPMN by peroral pancreatoscopy.
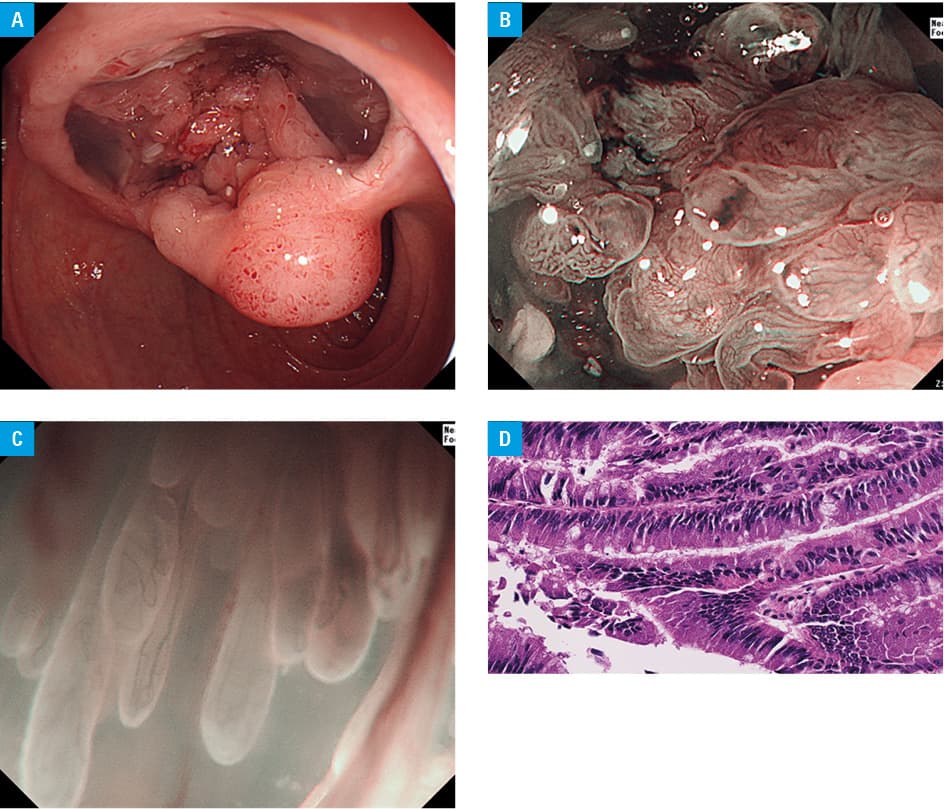
A 65‑year‑old man visited our hospital for evaluation of a cystic pancreatic lesion. Contrast‑enhanced computed tomography revealed a 53‑mm cystic lesion in the head of the pancreas. Esophagogastroduodenoscopy performed before endoscopic ultrasound (EUS) revealed a huge mucin‑filled cavity in the oral side of the main duodenal papilla (Figure 1A). We diagnosed IPMN with duodenal fistula. After mucin removal by irrigation, nodules and capillary villous structures were observed, which were also clearly visible on NBI (Figure 1B and 1C). Based on the diagnostic algorithm for early gastric cancer with NBI, the microvascular patterns were gradually dilated without irregularity or structural unevenness. Therefore, we diagnosed the lesion as adenoma.2 A biopsy from villous structures under direct visualization revealed mucinous adenoma. There was strong suspicion of carcinoma on imaging by other modalities; therefore, we performed tumor resection. The resected specimen revealed a tumor originating from the accessory pancreatic duct that had spread over a wide area in the pancreas. A 50 × 45 mm whitish nodule was located posterior to villous structures. Histopathological examination of the nodule and villous structures showed carcinoma and adenoma, respectively (Figure 1D).
Intraductal papillary mucinous neoplasm is an intraluminal tumor characterized by extensive histopathological changes that range from papillary and hyperplastic mucin‑producing epithelium to adenocarcinomatous cells. Therefore, it is important to determine whether IPMN is benign or malignant.
Types of IPMN protrusion are classified on the basis of findings from peroral pancreatoscopy; lesions of fish‑egg‑like type with vascular images, villous type, and vegetative type were considered malignant.3,4 Endoscopic ultrasound is useful for the detection of papillary protrusions that indicate papillary adenocarcinoma and adenoma in large protrusions; however, detecting a malignant lesion in a demarcated area of a flat protrusion using EUS is challenging. In this case, we clearly observed findings of adenoma using NBI. The malignant component could not be observed, but the benign portion showed findings similar to NBI diagnostic findings of the stomach. By defining the presented feature as NBI finding of benign IPMN, peroral pancreatoscopy with NBI may facilitate the diagnostic differentiation of IPMN as benign or malignant.
- Tanaka M, Fernández‑Del Castillo C, Kamisawa T, et al. Revisions of international consensus Fukuoka guidelines for the management of IPMN of the pancreas. Pancreatology. 2017; 17: 738‑753. | Crossref
- Muto M, Yao K, Kaise M, et al. Magnifying endoscopy simple diagnostic algorithm for early gastric cancer (MESDA‑G). Dig Endosc. 2016; 28: 379‑393. | Crossref
- Yamao K, Ohashi K, Nakamura T, et al. Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases. Gastrointest Endosc. 2003; 57: 205‑209. | Crossref
- Miura T, Igarashi Y, Okano N, et al. Endoscopic diagnosis of intraductal papillary‑mucinous neoplasm of the pancreas by means of peroral pancreatoscopy using a small‑diameter videoscope and narrow‑band imaging. Dig Endosc. 2010; 22: 119‑123. | Crossref
ARTICLE INFORMATION