Acromegaly due to ectopic growth hormone–releasing hormone secretion by lung carcinoid



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Acromegaly due to ectopic growth hormone–releasing hormone secretion by lung carcinoid
Neuroendocrine tumors secreting growth hormone–releasing hormone (GHRH) are very rare, causing acromegaly in less than 1% of all cases.1 The clinical presentation and hormonal manifestation of acromegaly do not differ between growth hormone (GH)–secreting pituitary adenoma and GHRH‑secreting tumors.1-4 While the diagnostic workup of acromegaly is easy, identification of the ectopic cause of the disease may be challenging.
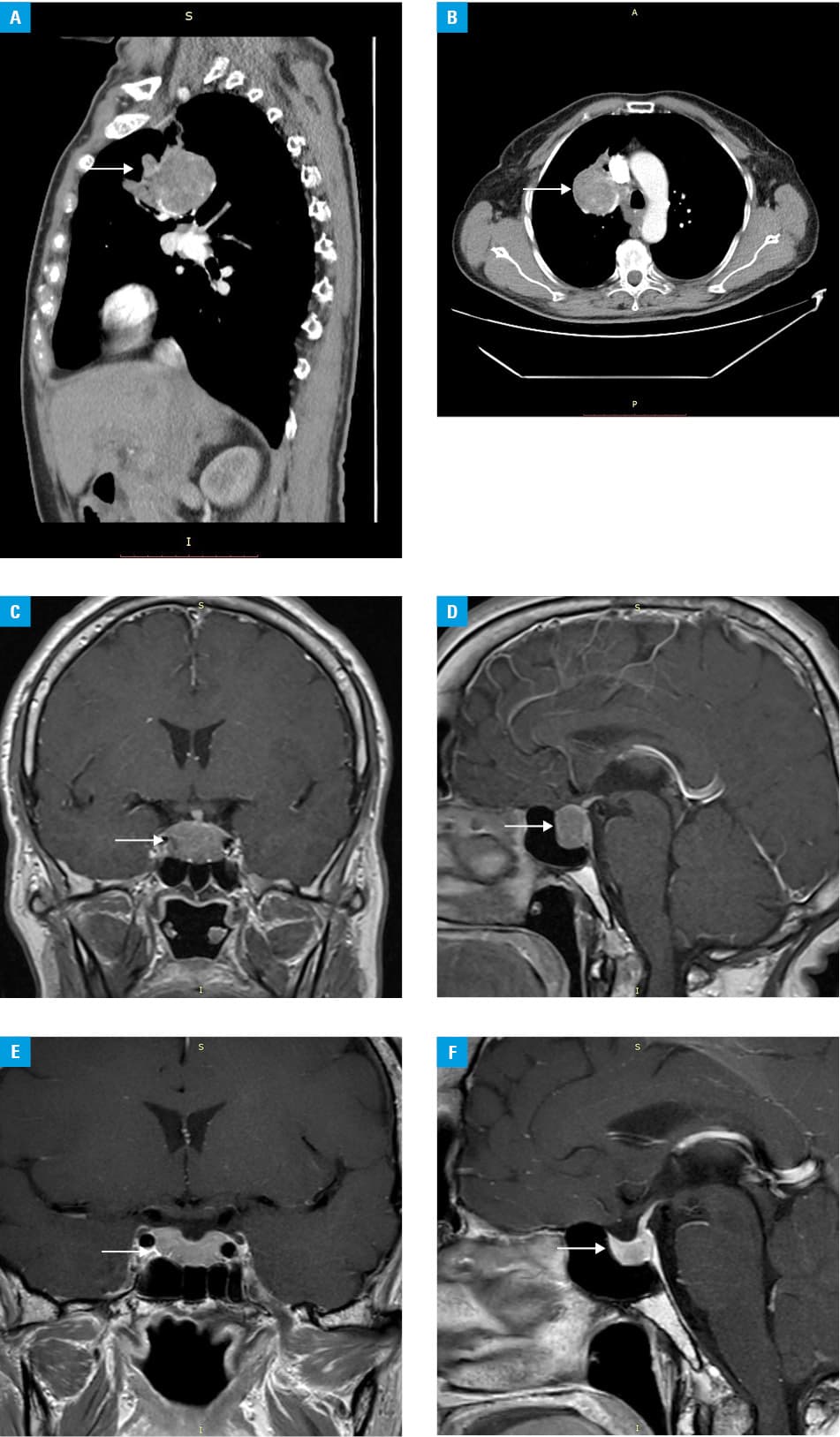
A 59‑year‑old woman was referred to the endocrinology department. She was diagnosed with tuberculosis 21 years earlier, when the tumor of the right lung, 40 × 50 mm in diameter, was detected. The patient had been receiving tuberculostatic drugs for several months, but the lung tumor did not change in size (Figure 1A and 1B). She visited an outpatient pulmonary clinic on a regular basis, in 1- to 2‑year intervals. The patient reported typical symptoms of acromegaly persisting for 6 years. Acromegaly was confirmed by serum GH concentration not suppressed below 1 ng/ml in an oral glucose tolerance test (GH nadir, 25.4 ng/ml) and an elevated level of insulin‑like growth factor 1 (IGF‑1) at 582 ng/ml (reference range, 75–212 ng/ml). A pituitary tumor, 14 × 17 × 27 mm in size, infiltrating the cavernous sinus bilaterally and compressing the optic chiasm, was seen on magnetic resonance imaging (MRI) (Figure 1C and 1D), although no visual field defect was reported. Other hormonal disturbances and carcinoid syndrome were excluded. Positron emission tomography–computed tomography using 18F‑fluorodeoxyglucose revealed a lung tumor of 58 × 48 × 53 mm in size (standardized uptake value, 5.3). Octreotide LAR therapy at a dose of 30 mg was initiated and, after 3 months of treatment, IGF‑1 and GH levels decreased to 364 ng/ml and 2.18 ng/ml, respectively. Signs and symptoms of acromegaly diminished. Neurosurgery of the pituitary tumor was planned, but first the patient was referred to the department of thoracic surgery for lung tumor resection. Biopsy of the tumor was performed and its results showed no specific abnormalities. Octreotide LAR therapy was discontinued after 6 months, just before the thoracic surgery. Histological examination showed features typical of carcinoid (Ki67 <1%); after the surgery, the patient reported milder joint pain, no headaches, and normalized sweating. The IGF‑1 level returned to normal and the GH level markedly decreased 4 months following the surgery (GH nadir, 1.62 ng/ml; IGF‑1, 223 ng/ml). A radiologist revised the previous diagnosis to pituitary hyperplasia. Head MRI showed a decreased pituitary diameter (Figure 1E and 1F). Plasma GHRH levels before (17727 pg/ml) and after lung tumor resection (<100 pg/ml; reference range <100 pg/ml) clearly confirmed ectopic acromegaly and full recovery. The GH and IGF‑1 levels normalized 1 year (GH nadir, 1.17 ng/ml; IGF‑1, 169 ng/ml) after the surgery.
The presented case of acromegaly due to ectopic GHRH secretion is the second one recorded in our center.3 The assessment of plasma GHRH concentration is crucial for proper diagnostic workup, since positive GHRH immunoreactivity may not translate to biochemical and clinical manifestations of acromegaly in some tumors.1-4 Extrapituitary tumors are usually located in the lungs or in the pancreas and have been presented in single case reports, rarely in national, multicenter series of up to 21 cases.1-5 Differential diagnosis is difficult owing to similar clinical presentation and results of biochemical tests or pitfalls in MRI, and pituitary tumor, hyperplasia, or a normal pituitary gland are described.1,2 Accurate hormonal workup and imaging are crucial to avoid unnecessary pituitary surgery and to preserve pituitary function.
- Ghazi AA, Amirbaigloo A, Dezfooli AA, et al. Ectopic acromegaly due to growth hormone releasing hormone. Endocrine. 2013; 43: 293‑302. | Crossref
- Kyriakiskis N. Trouillas J, Dang MN, et al. Diagnostic challenges and management of a patient with acromegaly due to ectopic growth hormone‑releasing hormone secretion from a bronchial carcinoid tumour. Endocrinol Diabetes Metab Case Rep. 2017; 2017: 16‑0104. | Crossref
- Bolanowski M, Schopohl J, Marciniak M, et al. Acromegaly due to GHRH‑secreting large bronchial carcinoid. Complete recovery following tumor surgery. Exp Clin Endocrinol Diabetes. 2002; 110: 188‑192. | Crossref
- Garby L, Caron P, Claustrat F, et al. Clinical characteristics and outcome of acromegaly induced by ectopic secretion of growth hormone‑releasing hormone (GHRH): a French nationwide series of 21 cases. J Clin Endocrinol Metab. 2012; 97: 2093‑2104. | Crossref
- Stelmachowska‑Banaś M, Głogowski M, Vasiljevic A, et al. Ectopic acromegaly due to growth hormone‑releasing hormone producing bronchial carcinoid causing somatotroph hyperplasia and partial pituitary insufficiency. Pol Arch Intern Med. 2019; 129: 208‑210. | Crossref
ARTICLE INFORMATION