The clinical value of the routine analysis of cardiac implantable electronic devices after the patient’s death in a tertiary cardiovascular center
Key words: autopsy, cardiac implantable electronic device, implantable cardioverter-defibrillator retrieval, pacemaker retrieval, sudden death



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
The clinical value of the routine analysis of cardiac implantable electronic devices after the patient’s death in a tertiary cardiovascular center
Introduction: The postmortem interrogation of cardiac implantable electronic devices (CIEDs) has not been regularly practiced yet. We presumed that it can provide data not only on the mechanism of the patient’s death but also on possible device malfunctions contributing to its occurrence.
Objectives: The study aimed to determine the usefulness of the explantation and interrogation of CIEDs after the patient’s death in routine clinical practice, when combined with autopsy findings and clinical follow‑up starting from the time after device implantation.
Patients and methods: Between August 24, 2008 and August 30, 2018, all patients who underwent autopsy in the tertiary cardiovascular center or partner facilities had the device explanted and interrogated by the qualified electrophysiologist. Clinical characteristics obtained at the time of device implantation and patients’ death were obtained from medical records. Device interrogation results were then combined with autopsy report and clinical data.
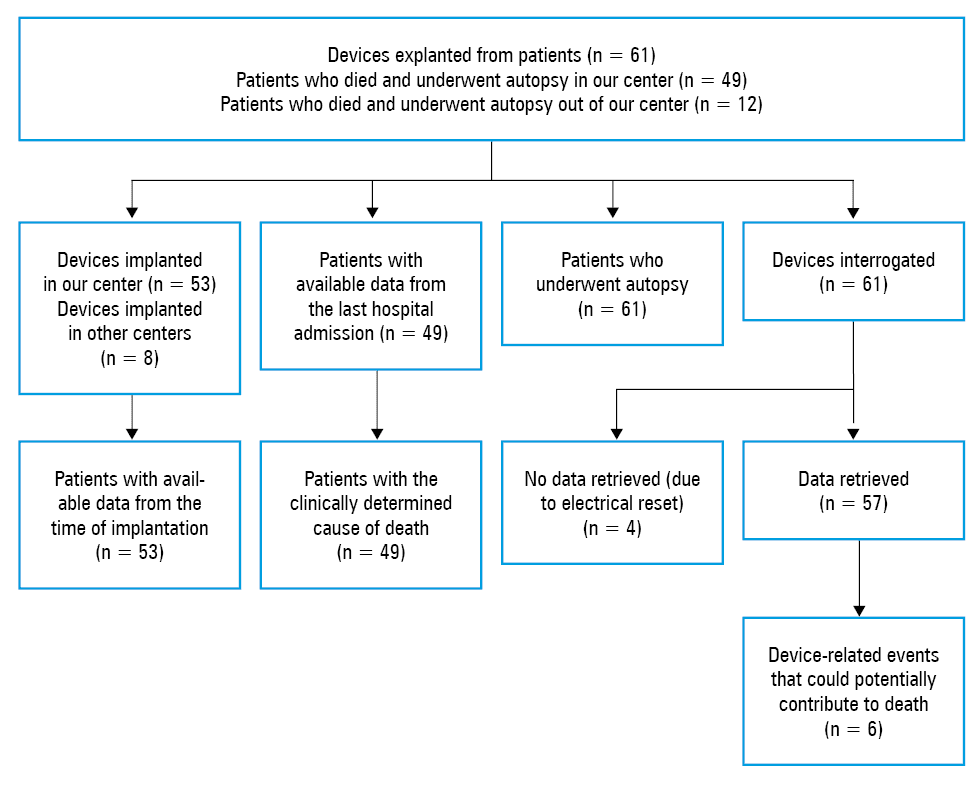
Results: Out of 1200 autopsied patients, the device was removed and analyzed in 61 individuals. Clinical characteristics from the time of implantation and patients’ death were available in 53 (86.7%) and 49 (80.3%) patients, respectively. Device‑related concerns, undetected during patients’ hospital stay, were noted in 6 cases (6.1%) and included 3 programming and 3 hardware issues.
Conclusions: To our knowledge, this is the first study to date to combine the clinical follow‑up of patients before death and on admission at the end of life, autopsy results, and postmortem CIED interrogation. Having implemented the device interrogation, we found 6 CIED‑related events potentially associated with patients’ death, which were not detected before its occurrence.
What's new?
Our study is the first to date to combine the clinical follow‑up of patients before death and on admission at the end of life, autopsy results, and the postmortem interrogation of cardiac implantable electronic devices (CIEDs). Complementing the standard examination with device interrogation allowed us to detect 6 CIED‑related events potentially associated with death, which had not been revealed before its occurrence. The inclusion of the routine postmortem interrogation of CIEDs can expand the knowledge of the mechanisms of patients’ death and possible device malfunctions, often undetectable in a different way.
Introduction
The implantation of cardiovascular implantable electronic devices (CIEDs) has become a routine procedure worldwide. According to the report of the European Heart Rhythm Association, more than 500000 permanent pacemakers (PPMs), 80000 implantable cardioverter‑defibrillators (ICDs), and 50000 cardiac resynchronization therapy (CRT) devices are implanted annually in Europe, and the rate of performed implantations is growing every year.1,2 The current European Society of Cardiology guidelines on cardiac pacing and cardiac resynchronization therapy2 and the HRS/EHRA/APHRS/SOLAECE expert consensus clearly determine the indications for CIED implantation and programming.3 The appropriate programming of the device, particularly an ICD or a cardiac resynchronization therapy–implantable cardioverter‑defibrillator (CRT‑D), should not only protect the patient from life‑threatening brady- or tachyarrhythmias but also maximally minimize the occurrence of its inadequate and unnecessary interventions.
Despite the development in the system of care, including enhanced surveillance of patients with cardiac devices and frequent device monitoring, there is still a certain percentage of individuals with CIEDs in whom sudden death occurs. Furthermore, despite the wide accessibility of healthcare facilities, the mechanism of death in those patients often remains unknown, and the exact cause of death can be only determined on autopsy in a limited number of individuals. The studies conducted to date have suggested that the postmortem CIED interrogation, when combined with autopsy findings, may be a useful source of additional data not only on the mechanism of the patient’s death but also on the possible hardware or software malfunctions of the device contributing to death.4-10 However, the majority of those studies were conducted more than 2 decades ago. Therefore, they investigated the devices of older generations, in which the algorithms and capacities of currently implanted CIEDs were unavailable. Moreover, some authors did not combine the data from device interrogation with the clinical characteristics of the deceased patients.8
The objective of our study was to assess the usefulness of the routine combination of clinical patient follow‑up before death and during hospitalization at the end of life with the postmortem interrogation of CIEDs and autopsy results.
Methods
Studied devices
All consecutive patients with CIEDs who underwent autopsy between August 24, 2008 and August 30, 2018 in the high‑volume cardiovascular center or in the remote partner facilities of our hospital were included in this analysis. During the autopsy, each patient had their CIED removed, disinfected, and stored under appropriate conditions to be later interrogated by a qualified electrophysiologist. The study protocol was followed in accordance with the ethical principles for medical research involving human subjects, established by the Declaration of Helsinki, protecting the privacy of all patients and the confidentiality of their personal information. The study was designed to investigate an all‑comer population of patients with CIEDs without any exclusion criteria.
Autopsy analysis
The autopsy was performed in the first 24 hours after the patient’s death yet not earlier than 12 hours after confirming clinical death. During the autopsy procedure, all body cavities were opened and, subsequently, brain, thoracic, abdominal, and pelvic organs were examined after excision. Acute coronary syndrome and sudden cardiac death (SCD) were diagnosed based on the gross results described by Basso et al11,12 and subsequent histopathological analysis. The histopathological examination included routine staining with hematoxylin and eosin, fuchsinophilia detection, and immunohistochemical staining using the anti‑CD4 antibody. In doubtful cases, CD3 immunohistochemical staining was additionally used and the CD3 index was calculated. Histopathological evaluation was performed by 2 independent pathologists.
Data collection and interrogation of cardiac implantable electronic devices
The general demographic and clinical characteristics of the study patients from the time of device implantation, the follow‑up period, and the last hospitalization, along with the type of the implanted CIED, were obtained from the medical records established in the hospital. All records obtained during and after hospitalization were preserved in both digital and paper versions, as required by the hospital administrative system. Data could be accessed only by the authorized personnel using personal system access codes.
All devices were interrogated by 2 independent researchers (MT and JNi) and by MD, always supervised by a qualified electrophysiologist. If any event potentially associated with the patient’s death was detected, an independent researcher, unaware of the clinical characteristics of the patient (such as the cause and time of death), was asked to additionally interrogate the device to maintain objectivity. The CIED interrogation results of all individuals were then combined with the data from the final autopsy report and patients’ clinical characteristics.
Statistical analysis
This was an explorative study using the methods of descriptive statistics. The basic parameters of descriptive statistics for the analyzed continuous variables were presented as mean (SD) for normal distribution or as median (first quartile–third quartile; Q1–Q3) for other distributions. Categorical variables were expressed as the absolute and relative proportion (percentage) of patients with the respective attribute. The normality of distribution was verified using the Shapiro–Wilk test. All analyses were conducted using the Statistica 10 software (StatSoft, Inc., Tulsa, Oklahoma, United States).
Definitions
Sudden cardiac death (SCD) was clinically defined as a “natural, unexpected fatal event occurring within 1 hour from the onset of symptoms in an apparently healthy subject or in one whose disease was not so severe as to predict an abrupt outcome.”9 Any death due to clinically determined cardiac causes which did not fulfil the SCD criteria was classified as nonsudden cardiac death (NSCD). All other cases of patients dying neither of SCD nor NSCD were assigned to the noncardiac‑death group. Electrical storm was defined as 3 or more distinct episodes of ventricular tachycardia (VT) or ventricular fibrillation (VF) within 24 hours, requiring the intervention of the defibrillator (antitachycardia pacing and/or shock). A subsequent episode that started within 5 minutes following the cessation of the previous episode was not considered a new episode. An inappropriate shock was defined as ICD therapy delivered because of any reason other than detected and confirmed VT or VF. A shock terminating VT or VF was considered successful.
Results
Study population
Out of 1200 patients autopsied in the analyzed period, 61 with CIEDs had their devices removed and stored for analysis. The study population is briefly characterized in Figure 1.
The baseline characteristics of the analyzed population from the time of device implantation were available in 53 patients (86.9%) (Table 1). The mean (SD) age of patients at the time of implantation was 60.3 (12.1) years. The most frequent indication for CIED implantation was ischemic cardiomyopathy (ICM), with the majority of patients having multivessel coronary artery disease (83.8%). About 28.3% of the study patients had myocardial infarction, and 45.3% underwent coronary revascularization before implantation. In 24.5% of the patients, nonischemic cardiomyopathy was recognized as the underlying cause of CIED implantation. Indications for pacemaker implantation included complete heart block and symptomatic sinus node dysfunction. The vast majority of patients presented with New York Heart Association (NYHA) class II or III (each class was reported in 45.3% of the study patients).
Data are presented as number (percentage) of patients unless otherwise indicated.
a Data available only in patients with implantable cardioverter‑defibrillators or cardiac resynchronization therapy–implantable cardioverter‑defibrillators
Abbreviations: ACE‑I, angiotensin‑converting enzyme inhibitor; APTT, activated partial thromboplastin time; ARB, angiotensin receptor blocker; CABG, coronary artery bypass grafting; eGFR, estimated glomerular filtration rate; GFR, glomerular filtration rate; INR, international normalized ratio; LVEF, left ventricular ejection fraction; MI, myocardial infarction; MVD, multivessel disease; NT‑proBNP, N‑terminal fragment of the prohormone brain natriuretic peptide; NYHA, New York Heart Association; PAD, peripheral artery disease; PCI, percutaneous coronary intervention; PLT, platelet; RBC, red blood cell; SVD, single‑vessel disease; WBC, white blood cell; Q1, first quartile; Q3, third quartile | ||
Demographics (total n = 61) | ||
Male sex | 52 (85.2) | |
Age at implantation, y, mean (SD) | 60.3 (12.1) | |
Characteristics at the time of implantation (total n = 53) | ||
Indication for implantation | ||
Ischemic cardiomyopathy | Any | 31 (58.5) |
SVD | 5 (16.2) | |
MVD | 26 (83.8) | |
Nonischemic cardiomyopathy | 13 (24.5) | |
Prior MI | 15 (28.3) | |
Prior PCI | 19 (35.8) | |
Prior CABG | 5 (9.4) | |
PAD | 9 (17) | |
Diabetes | 11 (20.8) | |
Dyslipidemia | 29 (54.7) | |
NYHA class | II | 24 (45.3) |
III | 24 (45.3) | |
IV | 5 (9.4) | |
Atrial fibrillation | 18 (34) | |
Laboratory results | ||
RBC, × 106/μl, median (Q1–Q3) | 4.11 (3.88–4.55) | |
WBC, × 103/μl, median (Q1–Q3) | 7.92 (6.77–9.20) | |
PLT, × 103/μl, median (Q1–Q3) | 190 (169–307) | |
GFR ≤60 ml/min/1.73 m2 | 19 (35.8) | |
eGFR, ml/min/1.73 m2, median (Q1–Q3) | 77 (40–83) | |
Spontaneous INR in patients without oral anticoagulation, median (Q1–Q3) | 1.15 (1.08–1.34) | |
INR in patients on oral anticoagulation, median (Q1–Q3) | 2.36 (2.22–2.59) | |
APTT, s, median (Q1–Q3) | 35.7 (29–41.9) | |
NT‑proBNP, pg/ml, median (Q1–Q3) | 315 (140–2 500) | |
LVEF, %, mean (SD)a | 19.6 (3.9) | |
Pharmacotherapy at discharge (total n = 44) | ||
ACE‑I or ARB | 40 (90.9) | |
β-Blocker | 43 (97.7) | |
Diuretics | 41 (93.2) | |
Amiodarone | 4 (9.1) | |
Sotalol | 2 (4.5) | |
Aldosterone antagonist | 28 (63.6) | |
Digoxin | 6 (13.6) | |
After the implantation, the majority of patients were administered a 3‑drug heart failure (HF) pharmacotherapy including a β-blocker (97.7%), a diuretic (93.2%), and an angiotensin‑converting enzyme inhibitor (90.9%). Four patients (9.1%) were given amiodarone, and 2 (4.5%) received sotalol at discharge. Digoxin was prescribed to 13.6% of the patients.
The characteristics of the analyzed devices are presented in Table 2. There were 24 ICDs and CRT‑Ds explanted (39.3% of each type), and the remaining 13 (21.3%) were PMs. Nine ICDs (18.7%) were implanted owing to the secondary prevention of SCD.
Data are presented as number (percentage) unless otherwise indicated.
Abbreviations: CRT‑D, cardiac resynchronization therapy–implantable cardioverter‑defibrillator; ICD, implantable cardioverter‑defibrillator; PM, pacemaker | |
Device type (total n = 61) | |
PM | 13 (21.3) |
ICD | 24 (39.3) |
Single‑chamber ICD | 10 (41.6) |
Dual‑chamber ICD | 14 (58.3) |
CRT‑D | 24 (39.3) |
CRT‑D implanted as the secondary prevention of sudden cardiac death | 9 (18.7) |
Device manufacturer (total n = 61) | |
Biotronik | 15 (24.6) |
Boston Scientific | 4 (6.5) |
Medtronic | 29 (47.6) |
St. Jude | 13 (21.3) |
Out of 61 patients whose devices were interrogated in our study, 49 died in our center and, therefore, the data from their last hospitalization were available (Figure 1). Their clinical characteristics from the last hospitalization are presented in Table 3. The mean (SD) age at death was 61.2 (11.8) years, and the median (Q1–Q3) survival after the device implantation was 1 (0.5–2.75) year. The median number of hospitalizations due to cardiovascular causes in that period was 2.
Data are presented as number (percentage) unless otherwise indicated.
Abbreviations: CIED, cardiac implantable electronic device; CRP, C‑reactive protein; ECMO, extracorporeal membrane oxygenation; HF, heart failure; IABP, intra‑aortic balloon pump; LVAD, left ventricular assist device; others, see Table 1 | ||
Characteristics from the last hospitalization (total n = 49) | ||
Age at death, y, mean (SD) | 61.2 (11.8) | |
Survival after implantation, y, median (Q1–Q3) | 1 (0.5–2.75) | |
Survival <1 y | 24 (49) | |
Hospitalizations due to cardiovascular causes from the implantation time to death, n, median (Q1–Q3) | 2 (0–5) | |
Cause of admission | ||
Decompensated HF | 30 (61.2) | |
Acute coronary syndrome | 8 (16.3) | |
Cardiac surgery | 4 (8.2) | |
CIED‑related | 6 (12.2) | |
Hospitalization data | ||
Cardiogenic shock | 24 (49) | |
Septic shock | 7 (14.4) | |
Mechanical circulatory support required | Any | 26 (53) |
LVAD | 6 (12.2) | |
ECMO | 9 (18.4) | |
IABP | 17 (34.7) | |
Hospital stay, d, median (Q1–Q3) | 16 (4–33) | |
RBC, × 106/μl, median (Q1–Q3) | 4 (3.51–4.6) | |
WBC, × 103/μl, median (Q1–Q3) | 11.04 (7.41–15.44) | |
PLT, × 103/μl, median (Q1–Q3) | 151 (105–205) | |
Procalcitonin, ng/ml, median (Q1–Q3) | 5.23 (1.26–27.24) | |
Amylase, U/l, median (Q1–Q3) | 30 (15.25–69) | |
CRP, mg/l, median (Q1–Q3) | 47.14 (11.18–138.8) | |
INR, median (Q1–Q3) | 1.51 (1.21–2.37) | |
INR in patients not receiving oral anticoagulation, median (Q1–Q3) | 1.37 (1.15–1.61) | |
INR in patients on oral anticoagulation, median (Q1–Q3) | 2.60 (2.41–4.51) | |
APTT, s, median (Q1–Q3) | 44.4 (33.2–61.12) | |
NT‑proBNP, pg/ml, median (Q1–Q3) | 6 923 (3 245–13 837) | |
NT‑proBNP in patients admitted due to HF decompensation, pg/ml, median (Q1–Q3) | 11 890 (806–23 822) | |
eGFR, ml/min/1.73 m2, median (Q1–Q3) | 41.5 (27.2–54) | |
The 3 most prevalent causes of the last admission before death included chronic HF decompensation (61.2%), acute coronary syndrome (16.3%), and cardiac surgery (8.2%). We identified 6 CIED‑related admissions (12.2%) due to suspicion of electrode dysfunction (n = 2) or infective endocarditis (n = 2), electrical storm (n = 1), and the need for the reoperation due to pocket hematoma after PPM implantation (n = 1). On admission, the majority of patients had elevated median levels of C‑reactive protein (47.14 mg/l) and N‑terminal fragment of the prohormone brain natriuretic peptide (6923 pg/ml). The median estimated glomerular filtration rate was 41.5 ml/min/1.73 m2. The median hospitalization time was 16 days.
Causes of death
As presented in Figure 1, all patients underwent autopsy, the findings of which, along with the final diagnoses made by physicians in charge, are presented in Table 4. In 31.1% of the study patients, the specific cause of death could not be established on autopsy (Figure 2A). In 18% of the patients, death was caused by acute coronary syndrome; in 24.6%, by other cardiovascular causes (such as HF decompensation or aortic aneurysm rupture); in 11.5%, by pneumonia; in 9.8%, by cerebrovascular accidents; and in 4.9%, by malignancy progression.
Data are presented as number (percentage) unless otherwise indicated.
Abbreviations: see Table 3 | ||
Specific cause of death on autopsy (total n = 61) | ||
Acute coronary syndrome | 11 (18) | |
Other cardiovascular causes | Any | 15 (24.6) |
Device‑related (general) | 4 (6.6) | |
LVAD thrombosis | 3 (4.9) | |
Infective endocarditis | 1 (1.6) | |
Pneumonia | 7 (11.4) | |
Cerebrovascular causes | 6 (9.8) | |
Metastatic malignancies | 3 (4.9) | |
Unspecified | 19 (31.1) | |
Clinically determined cause of death (total n = 49) | ||
Sudden cardiac death | 13 (26.5) | |
Nonsudden cardiac death | 26 (53.1) | |
Noncardiac death | 9 (18.4) | |
Unspecified | 1 (2) | |
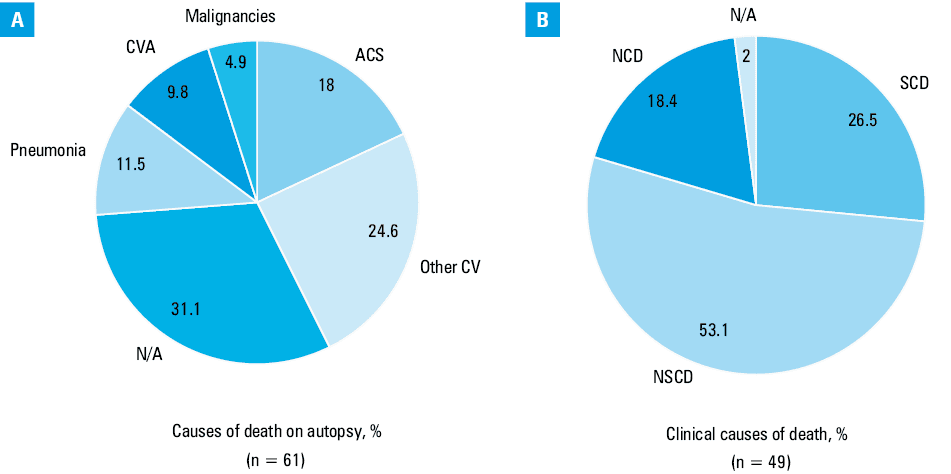
There were 4 deaths (6.6%) possibly associated with cardiac devices: 1 case of cardiac device‑related endocarditis and 3 cases of fatal left ventricular assist device thrombosis. However, no abnormalities were found during the interrogation of the CIEDs obtained from those patients. From the clinical perspective, the majority of patients died of NSCD (53.1%), 13 patients (26.5%) died suddenly of cardiac causes, and 9 patients (18.4%) died of noncardiac causes (Figure 2B).
Results of the postmortem cardiac implantable electronic device interrogation
The postmortem interrogation of all devices (n = 61) was performed. However, as electrical reset occurred in 4 devices, data were retrieved only from the remaining 57 (Figure 1). The median (Q1–Q3) battery life estimated after death was 5 (2.5–6.6) years, and indications for elective replacement were noted for 3 devices.
According to the study patients’ records, there were 8 individuals (13.1%) who died of asystole (5 with PPMs and 3 with ICDs) and 9 (14.7%) who died of pulseless electrical activity (5 with PPMs, 2 with ICDs, and 2 with CRT‑Ds). In the postmortem interrogation of the devices explanted from those patients, we found no traces of unsuccessful pacing potentially contributing to their death. Ventricular tachyarrhythmias during the last 48 hours occurred in 17 patients (27.8%). However, all of them were eventually successfully terminated by the devices. Seven patients (11.5%) experienced electrical storm in the last 48 hours. In 3 patients, the devices delivered only 1 successful adequate shock therapy. In other 4 individuals, the devices required the median (Q1–Q3) of 3 (2–5) unsuccessful shocks before the successful one terminating the electrical storm was delivered.
During the interrogation, we found 6 events (9.8%) possibly related to the medical condition of the study patients (Table 5). Four cases were related to ICDs and 2 to CRT‑Ds. In 1 patient (no. 25) with a marked progression of ICM, there were 6 unsuccessful ICD shocks due to electrical storm on the day before death. In another patient (no. 28) with severe HF, loss of left ventricular pacing 4 days before death was noted. In patient no. 57, who died just 13 days after CRT‑D implantation, no defibrillation threshold testing (DFT) was conducted, and the patient experienced electrical storm eventually terminated after 6 unsuccessful shocks on the day before death.
Patient no. | Age | Sex | CIED type | Indication for implantation | Survival | Regular CIED monitoring | CIED‑related issue | Autopsy results | Clinical diagnoses at the last hospitalization | CIED issue related to death |
Abbreviations: ACS, acute coronary syndrome; APE, acute pulmonary embolism; CTO, chronic total occlusion; DCM, dilated cardiomyopathy; DFT, defibrillation threshold testing; GI, gastrointestinal; ICM, ischemic cardiomyopathy; ICU, intensive care unit; LAD, left anterior descending artery; LCx, left circumflex artery; M, male; MI, myocardial infarction; NSTEMI, non–ST‑segment elevation myocardial infarction; RCA, right coronary artery; VA, ventricular arrhythmia; VF, ventricular fibrillation; others, see Tables 1, 2, and 3 | ||||||||||
17 | 56 | M | ICD | ICM, LVEF of 15% | 7 d | Yes | 1 day after LVAD implantation: 9 VT episodes in the detection zone, lasting 220 s; anti‑VT therapy turned off | Balser necrosis of the pancreas, splenic ischemic infarction, hemorrhage, and edema of the left brain hemisphere | Acute circulatory and respiratory failure despite LVAD therapy
Hemorrhagic stroke of the left brain hemisphere | Possible |
25 | 67 | M | ICD | ICM, LVEF of 25% | 4.5 y | Yes | 6 unsuccessful shocks for electrical storm, finally terminated by the device 1 day before death | Severe systemic atherosclerosis, large myocardial scar of the anterior and lateral walls | ICM, history of 7 MIs, 12 PCIs, and CABG
Admission due to NSTEMI with LVEF of 10%–15%
Significant stenoses across all coronary arteries, treated with PCI
2 days after PCI: symptoms of APE with multiple VFs and cardiogenic shock development | Probable |
28 | 74 | M | CRT‑D | ICM, QRS >150 ms, LVEF of 25% | 3.8 y | Yes | Spontaneous loss of biventricular pacing 4 days prior to death | Severe systemic atherosclerosis, substernal hematoma in reabsorption, perihilar fibrosis, lower pulmonary lobe congestion | GI infection and hemodynamic instability developed 7 days after CABG | Possible |
32 | 77 | M | ICD | ICM, secondary prevention | 2 y | Yes | 4 unsuccessful shocks for electrical storm, finally terminated by the device 6 days before death | Severe systemic atherosclerosis, large myocardial scar of the lateral, inferior, and posterior walls, cardiac hypertrophy
Pneumonia of the left inferior lobe | Admission due to NSTEMI with LVEF of 15%
CTO of RCA and LCx, no stenosis in LAD
Pneumonia and severe hemodynamic instability in the ICU
Death <36 hrs after admission | Probable |
34 | 52 | M | ICD | DCM, LVEF of 30% | 3 y | Yes | Rapid RV impedance rise 3 weeks before death | Biventricular heart dilation, thrombus in the LV at the apex, CIED lead vegetation/thrombus | Admission due to HF decompensation with LVEF of 18%
Hemodynamic instability, development of APE | Probable |
57 | 67 | M | CRT‑D | ICM, LVEF of 22% | 0.1 y | Yes | 6 unsuccessful shocks for electrical storm, finally terminated by the device 1 day before death
No DFT performed in the history of the device | Atherosclerotic aneurysm of the abdominal aorta, porcelain aorta, multiple myocardial scars of the anterior, lateral, and inferior LV walls | Admission due to angina and suspicion of CIED dysfunction—no VA in the memory of the device
Abrupt worsening of the patient’s condition
2 days after admission: hemodynamic instability and cardiac arrest with successful CPR
Death on the following day due to recurrent cardiac arrest not responding to external shocks | Probable |
Discussion
The main findings of our study could be summarized as follows: 1) our study is the first to date to combine a detailed clinical follow‑up of patients from the time of device implantation to the admission at the end of life with the results of autopsy and the postmortem CIED interrogation; 2) implementing the CIED interrogation allowed us to detect 6 CIED‑related events potentially associated with patients’ death, which had not been discovered before its occurrence; 3) the inclusion of the routine postmortem interrogation of CIEDs may expand the knowledge of the mechanisms of patients’ death and the presence and frequency of possible device malfunctions, often undetectable in any different way.
Although cardiovascular mortality has decreased in the last decades, still more than 17 million people die of cardiovascular causes worldwide, with 25% of those deaths being attributable to SCD.13 The population of patients with high‑voltage CIEDs (ICDs and CRT‑Ds), such as that investigated in our study, is usually burdened with multiple risk factors for premature death. In this population in Poland, the 1‑year mortality can reach 8.1% to 11.5%.14,15 Therefore, various attempts should be taken to prevent premature death in those patients.
The postmortem interrogation of CIEDs is one of those attempts. However, it is an extremely rarely used method and still a barely investigated field of cardiovascular medicine. In 2007, nearly half of the American morticians (44%) considered a CIED as useless medical waste.16 To date, there were only a few studies investigating the postmortem CIED interrogation,4-10 and their significant heterogeneity hinders their message in a wider context. Moreover, in the routine clinical practice, not every patient undergoes autopsy after death in the hospital. If the cause of death can be clinically determined, the autopsy—and the postmortem interrogation of the device—is not performed. Although this approach seems to be completely understandable, it leaves a plethora of the CIEDs unchecked after patients’ death and, thus, the rate of device failures in the real‑world population cannot be determined. Therefore, in our opinion, any contribution to this relatively underinvestigated field should be considered a valuable source of information.
Our study adopted a unique approach, which has not been followed before. We gathered the clinical characteristics of all consecutive patients with CIEDs who underwent autopsy in our facilities and combined them with the information obtained during the postmortem device interrogation. Thus, in the majority of patients, we could analyze the indications for implantation and a broad clinical profile of patients at the time of implantation. Then, we examined the association of these data with the disease progression resulting in patients’ death.
The clinical profile of patients admitted for their last hospital stay, consistent with the tertiary reference characteristics of our hospital, is an important issue to discuss here. Among patients in whom data on that hospitalization were available, the majority presented with severely advanced cardiovascular disease, mostly of ischemic etiology, which, as indicated in our recent analysis,17 could impact their outcomes. The majority of patients with acute coronary syndrome were admitted with cardiogenic shock, and their death was mostly caused by cardiac mechanical insufficiency (n = 7 [87.5%]). Therefore, those patients could not have benefited from their CIEDs. Almost 2/3 of patients with available data from their last hospital stay were admitted because of HF decompensation. In 53% of this population, mechanical circulatory support, mostly using an intra‑aortic balloon pump, was necessary. Their median (Q1–Q3) hospitalization time was 27 (8–49) days, and, in most cases, these patients required more intensive treatment including mechanical circulatory support devices.
In our study, we identified 6 possible CIED‑related events (all of them in patients with defibrillators), which might have played a role in the patients’ deterioration (Table 5). In the population of 61 patients, the occurrence of device‑related issues at the level of 9.8% is slightly higher than yet still comparable with the aforementioned findings of other authors. In the recent study by Lacour et al,10 the prevalence of device‑related concerns was 6% regarding 151 CIEDs, whereas in the study from the San Francisco area, conducted by Tseng et al,5 it was 50% regarding 22 CIEDs. Of note, the authors of the latter study determined the frequency of device‑related issues in high‑voltage devices to be 87.5%, with the majority of events being associated with improper sensing or detection of fatal tachyarrhythmia.
In patient no. 28, left ventricular pacing was lost 4 days before death, which could have resulted in loss of synchronized ventricular contraction and HF decompensation. However, loss of biventricular pacing could also have been caused by HF decompensation after coronary artery bypass graft surgery.18 According to the autopsy results, the patient died of circulatory congestion, which supported the hypothesis that loss of biventricular pacing contributed to the patient’s worsening condition. There are multiple causes of biventricular pacing loss, but only a few seemed to be relevant in that patient. Although the most frequent causes of short‑term or sustained biventricular pacing include supraventricular tachyarrhythmias (atrial fibrillation/atrial tachycardia) or improperly programmed paced and sensed atrioventricular intervals, this patient had no atrial tachycardia, and all intervals were programmed appropriately.19 Therefore, one could speculate that the loss of biventricular pacing could have been caused by either postsurgical lead dislodgement or device malfunction.
The number of patients suffering from electrical storm in the last 48 hours of their lives is another important issue to consider. There were 7 patients (11.5%) who experienced electrical storm during that time. As no other instances of electrical storm were recorded in the device memories, we assumed that, in all of those patients, the first electrical storm was also the last in their lives. Out of all those individuals, patient no. 57 had no DFT performed at the time of device implantation, and, later on, the device did not cease ventricular arrhythmia and delivered a series of unsuccessful shocks. Although the results of the SIMPLE (Shockless Implant Evaluation) trial did not support routine DFT at the time of device implantation, we presume that its abandonment could have been the possible cause of the device malfunction in the described case.20 However, that patient (no. 57) had severely advanced ICM after multiple myocardial infarctions, with left ventricular ejection fraction of 22% at the time of CRT‑D implantation, and had his device already programmed to deliver the maximum shock energy available (40 J). As the CIED still could not terminate electrical storm when necessary, the decision to dismiss DFT could have been dictated by the concern about the patient’s clinical condition.
Regarding the occurrence of electrical storm, the quality of death in patients with end‑stage HF need to be considered, as the development of electrical storm independently increases mortality in those with ICDs.21-24 Although, as shown in the Italian ICD registry, all patients with biventricular defibrillators who experienced electrical storm died at least 1 year after its occurrence, contradictory results were provided in the study by Duray et al,25 in which the patients who experienced electrical storm died either of arrhythmia or in the short period after its occurrence.26 One has to bear in mind that the majority of patients who survive electrical storm die of noncardiac or cardiac, albeit nonsudden, causes such as hemodynamic pump failure.
All 7 patients in our study who suffered from electrical storm died in up to 48 hours after its occurrence. In those in whom the initial therapy was unsuccessful, the devices required the median (Q1–Q3) of 3 (2–5) shocks to finally terminate electrical storm. On the other hand, lack of attempts to terminate ventricular arrhythmia would cause death anyway. Therefore, as all patients in our registry who experienced electrical storm had clinically evident end‑stage HF, the clinical utility of maintaining an active antitachyarrhythmic mode in this group of patients can be discussed.
Study limitations
Admittedly, our study had some limitations, which need to be considered when analyzing its results. First, some study patients had a CIED implanted in other hospitals. Therefore, some data concerning baseline characteristics are missing. Second, not all patients had their indications for CIED implantation fully documented, namely, data on left ventricular ejection fraction or the type of prevention applied in some patients were unavailable. Third, no information on hospital admissions in other facilities was available. Thereby, the number of hospitalizations during the follow‑up could be slightly underestimated. Finally, as seen in Figure 1, 4 devices were not analyzed because of electrical reset. As we did not contact the manufacturer representatives, who could have unlocked those devices to permit a complete software analysis, lack of information from those 4 devices could potentially influence the results of our study.
Conclusions
Our study results indicated that the combination of clinical findings, autopsy results, and the systematic postmortem CIED interrogation can expand the knowledge of causes and mechanisms of patients’ death. The routine device interrogation could help to detect potential device‑related issues. In the light of extremely rarely performed device retrieval after the patient’s death, we would recommend more pronounced campaigns to raise awareness of this issue among morticians and cardiac electrophysiologists.
- Raatikainen MJ, Arnar DO, Zeppenfeld K, et al. Statistics on the use of cardiac electronic devices and electrophysiological procedures in the European Society of Cardiology countries: 2014 report from the European Heart Rhythm Association. Europace. 2015; 17: 1‑75. | Crossref
- Brignole M, Auricchio A, Baron‑Esquivias G, et al. 2013 ESC guidelines on cardiac pacing and cardiac resynchronization therapy: the task force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association (EHRA). Europace. 2013; 15: 1070‑1118.
- Wilkoff BL, Fauchier L, Stiles MK, et al. 2015 HRS/EHRA/APHRS/SOLAECE expert consensus statement on optimal implantable cardioverter‑defibrillator programming and testing. J Arrhythm. 2016; 32: 1‑28.
- Sinha SK, Crain B, Flickinger K, et al. Cardiovascular implantable electronic device function and longevity at autopsy: an underestimated resource. Heart Rhythm. 2016; 13: 1971‑1976. | Crossref
- Tseng ZH, Hayward RM, Clark NM, et al. Sudden death in patients with cardiac implantable electronic devices. JAMA Intern Med. 2015; 175: 1342‑1350. | Crossref
ARTICLE INFORMATION