Foreign metal bodies: an unexpected cause of epigastric pain in a patient after bariatric surgery



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Foreign metal bodies: an unexpected cause of epigastric pain in a patient after bariatric surgery
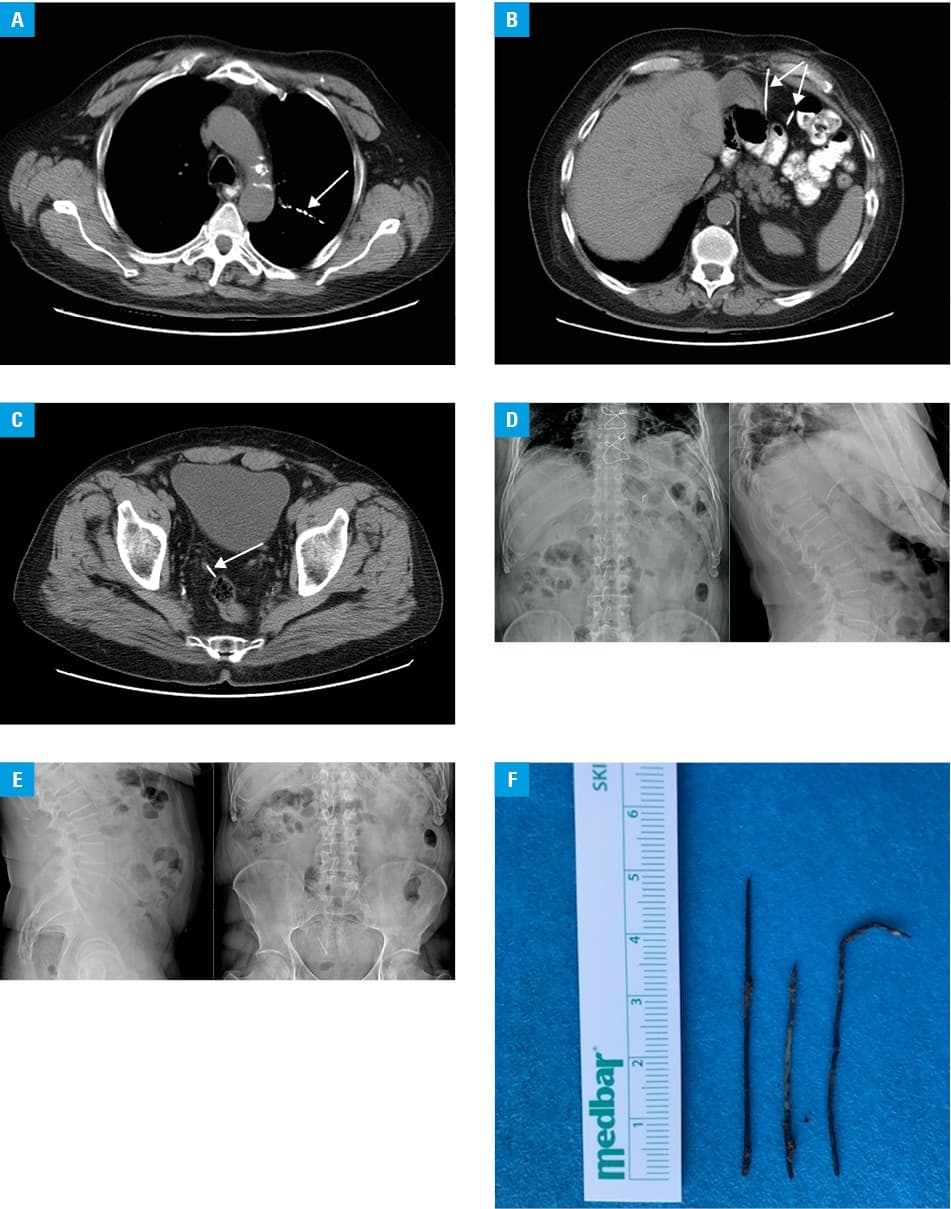
A 68‑year‑old man with numerous comorbidities was transferred to the department of internal medicine from the department of cardiac rehabilitation after exclusion of cardiovascular causes due to atypical thoracoabdominal pain. He had chronic heart failure, ischemic heart disease, metabolic syndrome, depression, and a history of non–ST‑elevation myocardial infarction (2017), percutaneous coronary intervention with drug‑eluting stent implantation, coronary artery bypass grafting (the left internal mammary artery to the left anterior descending artery, the aorta to the circumflex artery), ischemic stroke, and bariatric surgery (a sleeve gastrectomy) years before (medical records unavailable). On admission, the patient complained of dysphagia, strong retrosternal and epigastric pain (numeric rating scale, 10/10), that has been present since 2016. The physical examination revealed pain upon palpation in the epigastrium and numerous postsurgical scars on the thorax and abdomen. Laboratory abnormalities included anemia (hemoglobin, 13.4 g/dl; reference range, 13.5–16.5) and increased pro–brain natriuretic peptide activity (234 pg/ml; reference range, 0–125). Gastroscopy revealed oesophagojejunal anastomosis, most likely with an Omega‑loop, only a very short fragment of gastric mucosa or gastric metaplasia area (as in subtotal gastrectomy). Due to the unclear clinical picture, computed tomography was performed, which showed linear foreign body within the bronchi, another 2 in the stomach wall (5 cm in length) and intraperitoneally – between the anterior abdominal wall, stomach, and small intestine (3.5 cm and 5 cm, respectively), and the last one on the right to the sigmoid colon (3.7 cm) (Figure 1A‑1C). According to the patient’s relative, he had inserted several metal foreign bodies into his chest and abdomen through the skin during incarceration in 2012. Self‑mutilation was complicated by perforation of the left ventricle. Despite that information, the patient denied ingesting or inserting foreign bodies and threatened to commit suicide if the pain was not removed. The patient was transferred to the department of gastrointestinal surgery, as the clinical evaluation suggested that epigastric pain was caused by foreign metal bodies, located in the stomach wall. X‑ray of the abdomen was performed (Figure 1D‑1E). Open laparotomy was carried out under fluoroscopy. Two fragments of a metal wire of approximately 5 cm × 2 mm and 3.5 cm × 2mm were removed from the greater omentum in the stomach area. Another one (5 cm × 2 mm) was removed from the recto‑uterine pouch (Figure 1F). The patient was discharged home 8 days after the surgery in a good, stable condition.
Intentional nonsuicidal self‑injuries occur more frequently among prisoners than in the general population.1 The most common mechanisms of self‑injury in inmates include foreign body ingestion, self‑cutting, and head banging. Intrathoracic and intraabdominal insertion through the skin occurs rarely.2,3 Foreign bodies located in abdominal cavity may remain asymptomatic. In the described case, pain occurred after the migration of metal foreign bodies within the tissues and was caused by the external pressure on the stomach wall. The patient tended to have selective amnesia. He claimed that he did not remember the self‑mutilation, despite having reported the imprisonment and tried to explain memory loss by the stroke in the past. Despite repeated hospitalizations, the diagnosis was postponed by 3 years. This might have been caused by unavailability of medical records, a patient who was not willing to cooperate, and the need for exclusion of other more common causes of pain, such as pectoris angina, gastritis, or postoperative adhesions.
- Dixon‑Gordon K, Harrison N, Roesch R. Non‑suicidal self‑injury within offender populations: a systematic review. Int J Forensic Ment Health. 2012; 11: 33‑50. | Crossref
- Carli V, Mandelli L, Poštuvan V, et al. Self‑harm in prisoners. CNS Spectr. 2011; 16: 75‑81. | Crossref
- Morales YM, Guarnero PA. Non‑suicidal self‑injury among adult males in a correctional setting. Issues Ment Health Nurs. 2014; 35: 628‑634. | Crossref
ARTICLE INFORMATION