Pneumatosis intestinalis and hepatic portal venous gas in paralytic ileus due to Strongyloides stercoralis infestation



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Pneumatosis intestinalis and hepatic portal venous gas in paralytic ileus due to Strongyloides stercoralis infestation
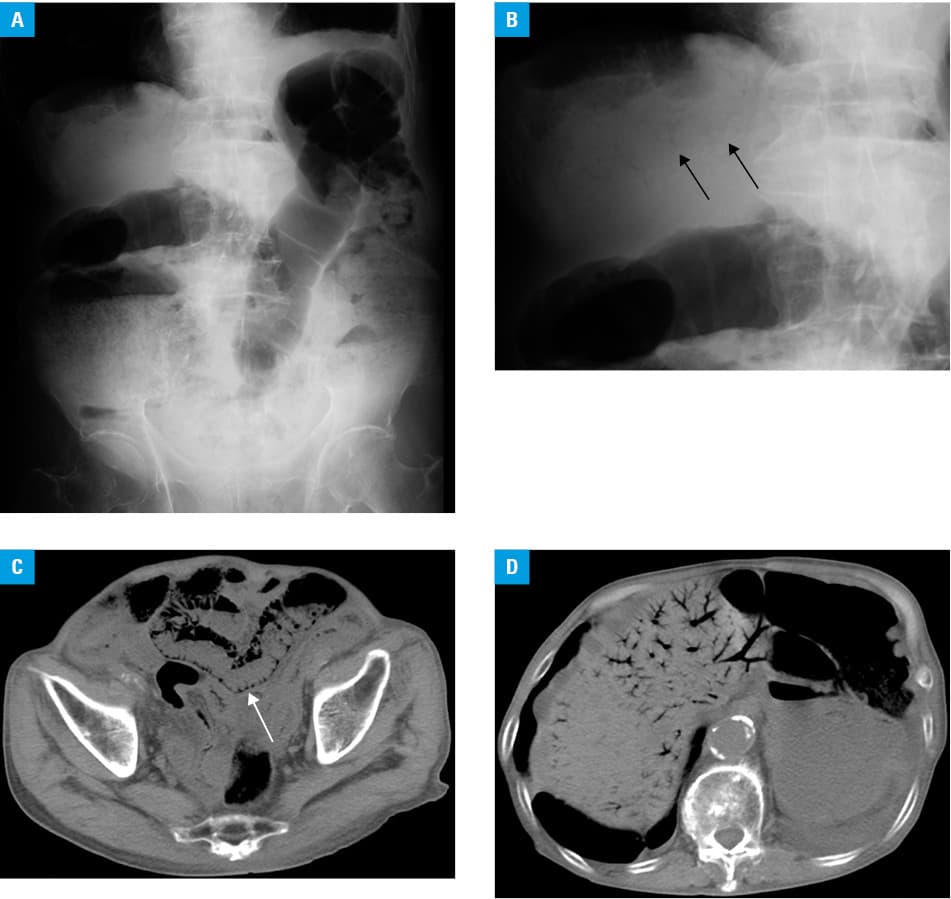
A 91‑year‑old man presented with vomiting and abdominal pain. His medical history was remarkable for hypertension, chronic obstructive pulmonary disease, and surgeries for laryngeal cancer and lung cancer. Physical examination revealed stable vital signs, a decreased body mass index of 16 kg/m2, and leg edema. The abdomen was distended and nontender, with decreased bowel sounds. Complete blood cell count yielded the following results: white blood cells, 3400/mm3; eosinophils, 60/mm3; and hemoglobin, 9.3 g/dl. Biochemical tests showed an elevated level of C‑reactive protein (10.5 mg/dl; reference range <0.14 mg/dl) and a markedly decreased level of albumin (2.1 g/dl; reference range, 4.1–5.1 g/dl). No parasite was found in the stool and blood culture was negative. Plain abdominal radiography showed distension of the intestine (Figure 1A) and a branching gas pattern in the liver, suggestive of hepatic portal venous gas (HPVG) (Figure 1B). Abdominal computed tomography demonstrated pneumatosis intestinalis (PI) of the small intestine (Figure 1C) and the colon and confirmed HPVG (Figure 1D). No mesenteric ischemia or pneumoperitoneum were observed. The patient was diagnosed with paralytic ileus presenting PI and HPVG. Conservative treatment with fluids and antibiotics resulted in improved symptoms, but paralytic ileus recurred. Repeated stool examination using agar plate culture finally revealed Strongyloides stercoralis infestation. Ivermectin, a broad‑spectrum antiparasitic drug, was started. Unfortunately, the patient died of gram‑negative septic shock.
Strongyloides stercoralis is a parasitic nematode, which infects the human intestine in tropical and subtropical regions. Approximately 100 million people are infected worldwide. This parasite resides in the intestine by an internal autoinfection cycle. Immunosuppressive conditions including aging, immunosuppressive medication, coinfection with viruses, and malignancies can cause complications of hyperinfection syndrome and disseminated strongyloidiasis carrying a high risk of mortality, which are characterized by small bowel obstruction due to bowel wall thickening, paralytic ileus, protein‑losing enteropathy, pneumonia, and gram‑negative sepsis.1,2 To the best of our knowledge, although these manifestations have been well known, this is the first report of strongyloidiasis presenting PI and HPVG. Pneumatosis intestinalis and HPVG are mostly caused by mesenteric ischemia and necrosis, observed in inflammatory, infectious, traumatic, and iatrogenic disorders.3 Endoscopic findings of PI can be seen as multiple submucosal air cysts. The following pathogenic mechanisms have been speculated in this case: in paralytic ileus due to hyperinfection syndrome, mucosal damage and increased intraluminal pressure may allow intraluminal gas to enter the damaged wall, resulting in PI, and to enter the portomesenteric veins, leading to HPVG.3 As for the diagnosis of strongyloidiasis, it should be emphasized that examination of many stool samples or repeated examinations is recommended,4 since direct stool examination is relatively insensitive. Given the low sensitivity of stool examination worldwide, advanced serological diagnosis using enzyme‑linked immunosorbent assays has been introduced recently.5
In conclusion, strongyloidiasis should be included in the differential diagnosis of paralytic ileus of unknown etiology in patients who have lived in or travelled to the endemic regions.
- Kishimoto K, Hokama A, Hirata T, et al. Endoscopic and histopathological study on the duodenum of Strongyloides stercoralis hyperinfection. World J Gastroenterol. 2008; 14: 1768‑1773. | Crossref
- Nabeya D, Haranaga S, Parrott GL, et al. Pulmonary strongyloidiasis: assessment between manifestation and radiological findings in 16 severe strongyloidiasis cases. BMC Infect Dis. 2017; 17: 320. | Crossref
- Sebastià C, Quiroga S, Espin E, et al. Portomesenteric vein gas: pathologic mechanisms, CT findings, and prognosis. Radiographics. 2000; 20: 1213‑1224; discussion: 1224‑1226. | Crossref
- Hirata T, Nakamura H, Kinjo N, et al. Increased detection rate of Strongyloides stercoralis by repeated stool examinations using the agar plate culture method. Am J Trop Med Hyg. 2007; 77: 683‑684. | Crossref
- Arifin N, Hanafiah KM, Ahmad H, et al. Serodiagnosis and early detection of Strongyloides stercoralis infection. J Microbiol Immunol Infect. 2019; 52: 371‑378. | Crossref
ARTICLE INFORMATION