Clinical characteristics and short-term outcomes of patients with coronavirus disease 2019: a retrospective single-center experience of a designated hospital in Poland
Key words: clinical characteristic, coronavirus disease 2019, severe acute respiratory syndrome coronavirus 2



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Clinical characteristics and short-term outcomes of patients with coronavirus disease 2019: a retrospective single-center experience of a designated hospital in Poland
Introduction: Since the first reported case of coronavirus disease 2019 (COVID‑19) in Poland, the worldwide pandemic has spread throughout the country, leading to many hospital admissions. There has been an urgent need to determine clinical characteristics of Polish patients with laboratory‑confirmed severe acute respiratory syndrome coronavirus 2 (SARS‑CoV‑2) infection in the clinical setting.
Objectives: The aim of this retrospective study was to outline characteristics and short‑term outcomes of SARS‑CoV‑2–positive patients.
Patients and methods: We retrospectively assessed 169 consecutive patients with laboratory‑confirmed COVID‑19 with regard to their clinical manifestations, radiological findings, treatment, complications, and outcomes.
Results: Of the 169 patients, more than half was aged 65 years or older (88; 52.1%), 51.5% were male, and 78.3% had comorbidities. The majority of patients (106; 62.7%) were transferred from outbreak locations in medical facilities. The most common symptoms on admission were fever (42%), shortness of breath (35%), and fatigue (33%). Twenty seven (15.4%) patients required intensive care unit admission. Overall mortality was 26.3% (n = 46) and was significantly higher in patients transferred from other facilities (38 out of 106; 35.8%), than in patients admitted directly to the hospital (8 out of 63; 12.69%; P <0.001). Seventeen out of 29 patients admitted to the intensive care unit died (mortality, 58.6%), including 30 out of 41 patients with acute respiratory distress syndrome (73.2% mortality rate).
Conclusions: Polish patients with COVID‑19 have similar characteristics and risk factors for adverse outcomes to those observed in countries in which outbreaks occurred earlier. Significantly higher mortality in patients transferred from other centers warrants special attention and transfer policy should be verified.
What's new?
This is the first report of clinical characteristics and short‑term outcomes of 169 hospitalized patients with new coronavirus disease 2019 (COVID‑19) coming from a designated hospital in Warsaw, Poland. We describe epidemiology, symptoms, and radiological characteristics of hospitalized patients with COVID‑19, focusing on the clinical course and outcomes. Our data confirm that the most exposed populations are the elderly and patients with comorbidities. Polish patients with COVID‑19 have similar characteristics and risk factors for adverse outcomes to patients from countries with earlier outbreak. Both public health policy actions and hospital management should focus on these particularly vulnerable patients.
Introduction
Coronavirus disease 2019 (COVID‑19) is an infectious disease caused by severe acute respiratory syndrome coronavirus 2 (SARS‑CoV‑2), with the first outbreak in humans in the city of Wuhan, China in December, 2019, as a result of a probable zoonotic transfer from bats.1 Since the first reported case of COVID‑19 in Poland on March 4, 2020, there have been 6674 diagnosed and 232 fatal cases of COVID‑19 nationwide (as of April 12, 2020).2
Initially, ordinances of the Polish Minister of Health introduced a state of epidemiological threat, followed by a state of COVID‑19 epidemic on March, 20, 2020. The tertiary multispecialty hospital in which the study took place was commissioned a designated infectious diseases center as a part of the general healthcare system reorganization program in response to the pandemic threat.
Our institution is located in the capital of Poland and is admitting solely patients with COVID‑19 who are frequently referred from various outbreak locations in medical facilities. Presented data provide information on clinical characteristics, treatment, and short‑term outcomes of patients with COVID‑19.
Patients and methods
This retrospective study was performed at the Central Clinical Hospital of the Ministry of the Interior and Administration in Warsaw, which was transformed into a designated referral COVID‑19 unit. According to the World Health Organization guidance, a confirmed case of COVID‑19 was defined as a positive result on real‑time reverse‑transcriptase‑polymerase‑chain‑reaction assay of nasal or pharyngeal swab specimens.3
Patients were admitted either directly from the emergency department, outpatient clinics, or external hospitals (so‑called transferred patients). Reasons for admission were moderate or severe COVID‑19 or SARS‑CoV‑2–positive patients with other severe concomitant acute or chronic diseases.
The period of hospitalization and status as of the day of discharge were analyzed. Electronic records from the Hospital Information System of consecutive patients with COVID‑19 were used and checked by 2 independent researchers. Electronic records from the Hospital Information System of consecutive patients with COVID‑19 hospitalized between March 16, 2020 and April 7, 2020 were analyzed by 2 independent researchers. Demographic, epidemiologic, clinical, imaging studies, treatment, complications, and outcomes, including admissions to an intensive care unit (ICU), the use of mechanical ventilation, and death, were analyzed. The study was retrospective in nature and therefore patient consent was deemed not necessary. The study was approved by the ethics committee of the Central Clinical Hospital of the Internal Affairs and Administration Ministry (58/2020).
Definitions
Transferred patients were defined as patients admitted from other healthcare facilities: hospitals, long‑term care facilities, and dialysis facilities. Pneumonia, acute respiratory distress syndrome, septic shock, were defined according to the interim guidance of the World Health Organization for novel coronavirus.4 Acute kidney injury was defined according to the 2012 Kidney Disease Improving Global Outcomes (KDIGO) guidelines.5
Statistical analysis
Continuous variables were expressed as means and SD or medians and interquartile ranges, as appropriate. Categorical variables were summarized as counts and percentages. No imputation was made for missing data. All statistics were deemed to be descriptive only.
We compared clinical characteristics of survivors vs nonsurvivors as well as patients admitted directly from the emergency department versus patients transferred from other facilities. Parametric (the t test for independent samples) or nonparametric (the Mann–Whitney test for independent samples) tests were performed, as appropriate. A P value of less than 0.05 was considered significant.
Results
Demographic, clinical, and radiological characteristics
Demographic, clinical, and radiological characteristics are shown in Table 1. The number of men and women were comparable, with a slight predominance of male sex (51.5% vs 48.5%, respectively). More than half of admitted patients were 65 years old or older (88; 52.1%). A total of 106 patients (61%) were transferred from external hospitals, long‑term care facilities, and dialysis facilities. Only 5 patients (3%) were healthcare workers. The most common symptoms at onset were fever (42%), shortness of breath (35%), fatigue (33%), cough (32%), followed by single cases of headache, nausea, vomiting, and diarrhea. Anosmia and ageusia were observed in 3 (1.7%) patients. At admission, mean blood oxygen saturation was 96%. The majority of patients (137 out of 169; 78.3%) had at least 1 comorbidity, the most common being hypertension (45.7%) followed by peripheral and cerebrovascular disease (33.1%), coronary heart disease (29.7%), malignancy, and chronic renal disease (both 35; 20.7%). Only 22 patients (12.6%) had chronic obstructive pulmonary disease. Just over a quarter of patients (26.6%) were asymptomatic at admission. At admission, chest X‑ray was done in 118 patients (67.4%). The most common finding was bilateral patchy shadowing (27.7%) but 42 patients (24%) had no abnormalities on initial chest radiography.
Parameter | All (n = 169) | Survivors (n = 123) | Nonsurvivors (n = 46) | P valuea | |
Data are presented as number (percentage) of patients unless otherwise indicated.
a Survivors vs nonsurvivors (t test or χ2 test, as appropriate)
Abbreviations: CHD, coronary heart disease; COPD, chronic obstructive pulmonary disease; CRD, chronic renal disease; CVD, cardiovascular disease; DM, diabetes mellitus; HCP, healthcare provider | |||||
Age, y, mean (SD) | 63.7 (19.6) | 59.3 (20.1) | 75.3 (11.9) | <0.00 | |
Sex | Male | 87 (51.5) | 57 (46.3) | 30 (65.2) | 0.29 |
Female | 82 (48.5) | 66 (53.7) | 16 (34.8) | ||
Symptoms | Fever | 74 (43.8) | 58 (47.2) | 16 (34.8) | 0.23 |
Cough | 56 (33.1) | 49 (39.8) | 7 (15.2) | – | |
Fatigue | 57 (33.7) | 41 (33.3) | 16 (34.8) | 0.86 | |
Shortness of breath | 61 (36.1) | 38 (30.9) | 23 (50) | 0.02 | |
Nausea and vomiting | 6 (3.6) | 4 (3.3) | 2 (4.3) | 0.73 | |
Diarrhea | 8 (4.7) | 7 (5.7) | 1 (2.2) | 0.34 | |
Comorbidities | COPD | 22 (13) | 13 (10.6) | 9 (19.6) | 0.13 |
DM | 32 (18.9) | 16 (13) | 16 (34.8) | – | |
Hypertension | 80 (47.3) | 53 (43.1) | 27 (58.7) | 0.07 | |
CHD | 52 (30.8) | 33 (26.8) | 19 (41.3) | 0.07 | |
CVD | 58 (34.3) | 36 (29.3) | 22 (47.8) | 0.02 | |
Malignancy | 35 (20.7) | 20 (16.3) | 15 (32.6) | 0.02 | |
CRD | 35 (20.7) | 27 (22) | 8 (17.4) | 0.52 | |
Other | 51 (30.2) | 33 (26.8) | 18 (39.1) | 0.12 | |
Radiological chest imaging | Ground‑glass opacity | 7 (4.1) | 4 (3.3) | 3 (6.5) | 0.34 |
Local patchy shadowing | 40 (23.7) | 29 (23.6) | 11 (23.9) | 0.96 | |
Bilateral patchy shadowing | 31 (18.3) | 17 (13.8) | 14 (30.4) | 0.01 | |
Interstitial abnormalities | 11 (6.5) | 8 (6.5) | 3 (6.5) | 0.98 | |
No abnormalities | 42 (25) | 35 (28.5) | 7 (15.2) | 0.04 | |
Treatment and complications
The following treatments for COVID‑19 were used in a compassionate use program: 70.2% patients received chloroquine and 15.7% patients received lopinavir with ritonavir. In addition, the majority of patients (67.3%) received intravenous or oral antibiotic therapy for concomitant bacterial infections. Half of the patients (50.9%) received low‑molecular‑weight heparin to prevent thromboembolic complications. Oxygen therapy was administered in 94 patients (55.6%), including 1 patient on high‑flow oxygen therapy, and mechanical ventilation was initiated in 26 patients (15.6%). One patient needed extracorporeal membrane oxygenation, and 1 patient needed continuous renal replacement therapy. Pneumonia was diagnosed in 87 patients (51.8%), acute respiratory distress syndrome in 41 (24.4%), acute kidney injury in 17 (10.2%), and septic shock also in 17 (10.2%).
Outcomes
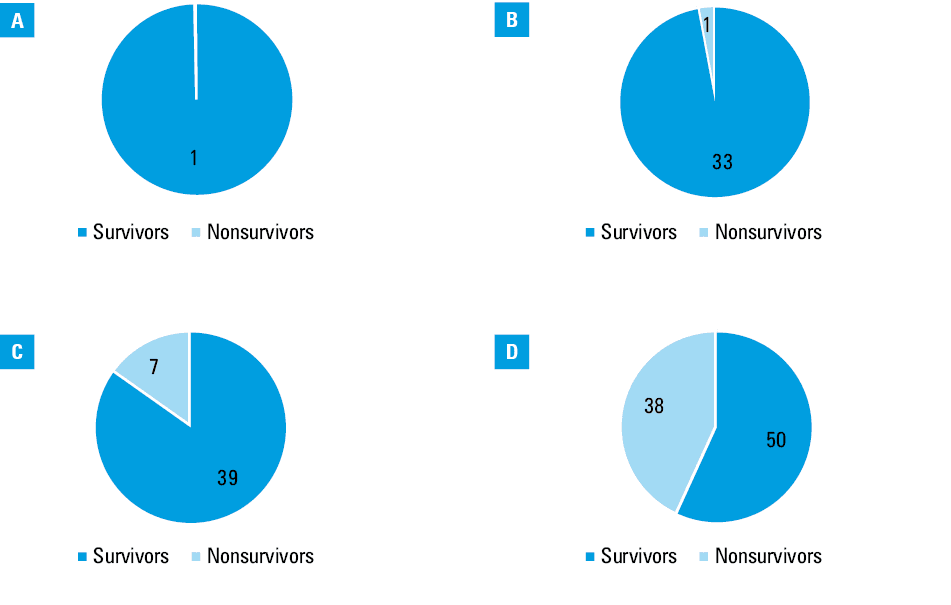
As of April 7, 2020, 80 patients (45.7%) were still hospitalized and 46 (26.3%) were discharged home or to isolation areas. Mean (SD) hospitalization time was 5.3 (3.5) days for discharged patients. Admission to the ICU was required in 27 (15.4%) patients, and mechanical ventilation was necessary in 26 (14.9%) patients (Table 2). Figure 1 illustrates the demographic structure and age‑related deaths. Overall mortality was 26.3% (46) and was significantly higher in patients transferred from other facilities (38 out of 106; 35.8%) than in patients admitted directly to the hospital (8 out of 63; 12.69%; P <0.001). Seventeen out of 29 patients admitted to the ICU died (58.6%) including 30 out of 41 patients with severe pneumonia (73.2% mortality).
Parameter | All (n = 169) | Survivors (n = 123) | Nonsurvivors (n = 46) | P valuea |
Data are presented as number (percentage) of patients unless otherwise indicated.
a Survivors vs nonsurvivors (t test or χ2 test, as appropriate)
Abbreviations: AKI, acute kidney injury; ARDS, acute respiratory distress syndrome; CRRT, continuous renal replacement therapy; DIC, disseminated intravascular coagulation; ECMO, extracorporeal membrane oxygenation; ICU, intensive care unit; NIV, noninvasive ventilation | ||||
Pneumonia | 87 (51.5) | 49 (39.8) | 38 (82.6) | 0.001 |
ARDS | 41 (24.3) | 11 (8.9) | 30 (65.2) | 0.001 |
AKI | 17 (10.1) | 7 (5.7) | 10 (21.7) | 0.001 |
DIC | 4 (2.4) | 2 (1.6) | 2 (4.3) | 0.31 |
Septic shock | 17 (10.1) | 6 (4.9) | 11 (23.9) | 0.001 |
Oxygen | 94 (55.6) | 58 (47.2) | 36 (78.3) | 0.001 |
Ventilator | 26 (15.4) | 11 (8.9) | 15 (32.6) | 0.001 |
NIV | 1 (0.6) | 1 (0.8) | 0 | Not performed |
ECMO | 1 (0.6) | 0 | 1 (2.2) | Not performed |
CRRT | 1 (0.6) | 0 | 1 (2.2) | Not performed |
ICU | 27 (16) | 11 (8.9) | 16 (34.8) | 0.001 |
Discussion
Over the past 2 decades, epidemics of 2 betacoronoviruses, severe acute respiratory syndrome coronavirus (SARS‑CoV) and Middle East respiratory syndrome coronavirus (MERS‑CoV) have caused more than 10000 cumulative cases with mortality rates of 10% for SARS‑CoV and 37% for MERS‑CoV.6,7 However, over the past 4 months, a novel‑coronavirus named SARS‑CoV‑2 led to over 100000 deaths and nearly 2000000 people infected all over the world.8 The first European cases were reported in France on January 24, 2020.9 In Poland, the first laboratory‑confirmed case was announced on March 4, 2020. On April 12, 2020, in Poland, there were 6674 laboratory‑confirmed cases with 232 fatal cases.2
Clinical manifestations of COVID‑19 in symptomatic patients were similar to the ones reported in large cohorts from China. A large proportion of asymptomatic patients (26.6%) is explained by the nature of our center designated to treat both severe COVID‑19 cases and patients infected with SARS‑CoV‑2 with mild or no COVID‑19 symptoms but severe concomitant conditions requiring hospitalization.
Based on the Hospital Therapeutic Committee recommendations, a high proportion of patients (70.3%) received chloroquine as part of the compassionate use program. These guidelines were based on the initial Chinese and Italian experience.10
In our study, 55.6% of patients required oxygen therapy, 16% were admitted to the ICU, and 15.4% required mechanical ventilation. Number of ventilated patients was not limited by the number of ventilators at our institution. Most Chinese studies report mechanical ventilation in less than 10% of patients. For example, Guan et al11 reported mechanical ventilation in 2.3%, and Huang et al,12 in 5% of patients. In a recent report from New York City, however,13 33.1% of patients required mechanical ventilation. These differences were explained by the authors by the illness severity and early‑intubation strategy in New York. Our results indicate an intermediate severity and more conservative intubation strategy. The latter is in concordance with the recent comments on the potential harms of the very aggressive intubation strategy.14
A recent systematic review and meta‑analysis conducted by Rodriguez‑Morales et al15 estimated mortality for hospitalized patients at 13%. Overall mortality in our study was unusually high (27.2%); however, this difference could be explained by the number of patients transferred from other centers, frequently in very severe condition or with multimorbidity (35.8%). For emergency department admissions, mortality was similar to the one observed by Rodriguez‑Morales et al15 (12.69%).
Overall, our cohort was older, with mean (SD) age of 63.7 (19.6) years, and had more comorbidities (78.3%) than cohorts described by the Chinese centers. For example, in a retrospective review by Guon et al,11 1099 hospitalized patients had mean (IQR) age of 47 (35–58) years, and only 23.7% had coexisting diseases. This explains low in‑hospital case fatality ratio of 1.4%. In another Chinese study of 102 hospitalized patients16 mortality was 16.7% in patients whose median (IQR) age was 54 (37–67) years and with 46.1% comorbidity ratio. In general, mean age of patients with COVID‑19 and comorbidities are higher in the European and American populations as compared with Chinese patients.13,16,17
Central Clinical Hospital of the Ministry of the Interior and Administration in Warsaw serves as a Polish reference center admitting patients with the most severe COVID‑19. Higher in‑hospital mortality in transferred patients should be analyzed taking into consideration very specific role of designated hospitals in the Polish healthcare system during the pandemic. Transferred patients represented a highly preselected population as usually those severely/critically ill were relocated to our hospital from their primary hospital locations where infection outbreaks occurred.
Therefore, epidemiological and clinical characteristics as well as outcomes are not representative for the general population of hospitalized patients with COVID‑19.
This study has several limitations. First, this is a retrospective study, and most of the data were obtained from the electronical patients history. Importantly, we are still in the initial/middle phase of the pandemic; patients are still hospitalized, so data are not generalizable. Importantly, given the specific nature of the designated hospital, substantial proportion of patients with SARS‑CoV‑2 were hospitalized due to severe concomitant diseases rather than for COVID‑19 itself. Therefore, some deaths were not classified as SARS‑CoV‑2–related deaths. Their detailed analysis will be presented elsewhere.
Conclusions
Polish patients with COVID‑19 have similar characteristics and risk factors for adverse outcomes to those observed in countries where outbreaks occurred earlier. Data from our center differ from general characteristics of hospitalized patients with COVID‑19 due to the specific role of the designated hospital and a large number of transferred patients. Nevertheless, a significantly higher mortality in patients transferred from other centers warrants special attention. Transfer policy should be verified with possible earlier admission to the reference center, before deterioration occurs.
- Andersen KG, Rambaut A, Lipkin WI, et al. The proximal origin of SARS‑CoV‑2. Nat Med. 2020; 26: 450‑452. | Crossref
- List of coronavirus infections (SARS‑CoV‑2) . Serwis Rzeczypospolitej Polskiej website. https://www.gov.pl/web/koronawirus/wykaz‑zarazen‑koronawirusem‑sars‑cov‑2. Accessed April 12, 2020.
- World Health Organization. Laboratory testing for coronavirus disease (COVID‑19) in suspected human cases: interim guidance, 19 March 2020. https://apps.who.int/iris/handle/10665/331501. Accessed April 18, 2020.
- World Health Organization. Clinical management of severe acute respiratory infection (SARI) when COVID‑19 is suspected: interim guidance, 13 March 2020. https://www.who.int/publications‑detail/clinical‑management‑of‑severe‑acute‑respiratory‑infection‑when‑novel‑coronavirus-(ncov)-infection‑is‑suspected. Accessed April 18, 2020.
- Khwaja A. KDIGO clinical practice guideline for acute kidney injury. Nephron Clin Pract. 2012; 120: c179‑c184. | Crossref
ARTICLE INFORMATION