Pyoderma gangrenosum with visceral involvement: a severe, recurrent disease affecting pulmonary, splenic, mesorectal, and subcutaneous tissues



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Pyoderma gangrenosum with visceral involvement: a severe, recurrent disease affecting pulmonary, splenic, mesorectal, and subcutaneous tissues
Pyoderma gangrenosum (PG) is a rare, ulcerative skin condition of unknown origin, with an annual incidence of 3 to 10 cases per million people.
Skin lesions develop as painful, edematous nodules or vesicles that progress to ulcerations with violaceous, edematous margins. Lesions may progress rapidly, up to 2 cm per 24 hours. Pathergy is observed in approximately 30% of patients.
Pyoderma gangrenosum is a neutrophilic disease. It is regarded as a condition accompanying other systemic diseases and, in adults, it usually coexists with inflammatory, hematologic, or malignant diseases (paraneoplastic syndrome). As many as 50% to 70% of adult patients have an underlying disease at the moment of PG diagnosis.1 However, PG may also be either idiopathic or induced by drugs.2
Extracutaneous manifestation is very rare in PG. Visceral lesions are usually seen as rapidly progressing, cavitated or noncavitated nodules mimicking cancer, abscess, deep fungal infection, Wegener granulomatosis, or tuberculosis.
Visceral involvement may precede, follow, or develop together with skin lesions. The time between visceral and skin involvement may vary from days to months.1
The first‑line treatment for PG includes systemic corticosteroids. In most cases, rapid resolution of lesions is observed. Other therapeutic options are sulphonamides, a broad panel of immunosuppressive drugs, intravenous immunoglobulins, and biological drugs.3,4
Patient prognosis varies owing to underlying diseases, visceral involvement, and treatment complications.
A 51‑year‑old woman with a history of vitiligo, Hashimoto disease, and nephrolithiasis presented with multiple, rapidly progressing, necrotic skin ulcerations, fever, productive cough, multiple lung infiltrates, and pleural effusion. Inflammatory markers were significantly elevated (C‑reactive protein, 1104.8 mmol/l; white blood cell count, 13.4 G/l), but the infective etiology of lesions was finally excluded. Normocytic anemia with a hemoglobin level of 80 g/dl was another prominent abnormality found. Based on clinical presentation along with skin and lung biopsies, PG with lung involvement was diagnosed. At the time of diagnosis, the lungs were the only extracutaneous site affected by the disease.
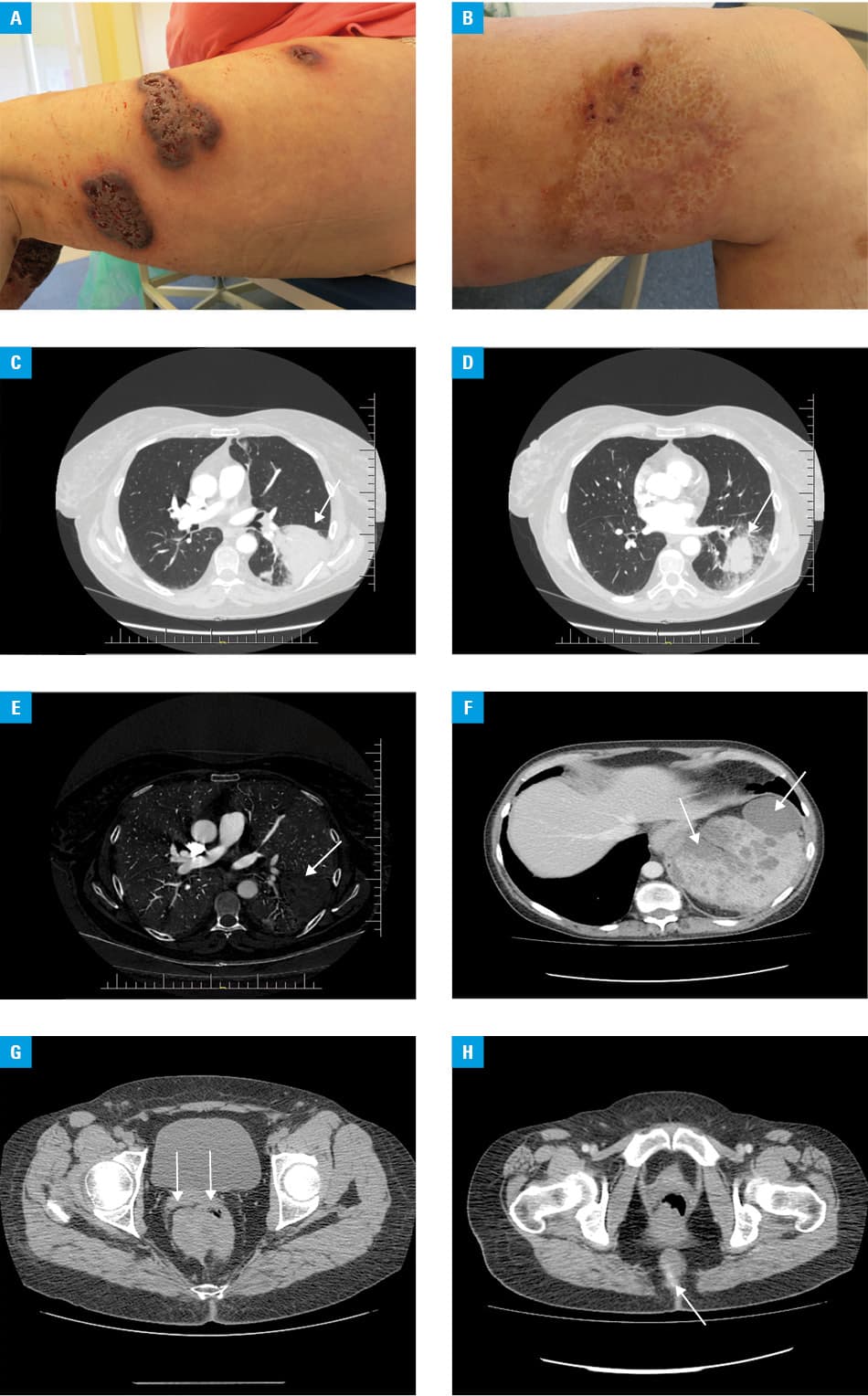
During the 11‑year follow‑up, the patient experienced multiple, severe flares resulting in new cutaneous (Figure 1A and 1B), pulmonary (Figure 1C–1E), splenic (Figure 1F), mesorectal (2 lesions, including 1 infiltrating the coccyx) (Figure 1G and 1H), and subcutaneous lesions. Due to typical clinical presentation, skin lesions were easy to diagnose. Subcutaneous lesions mimicked soft tissue abscess. Lung involvement resulted in cough, hemoptysis, rales, fever, and malaise. Chest computed tomography showed widespread inflammatory infiltrates with or without central necrosis, accompanied by ground glass opacities and pleural effusion. Splenic and mesorectal lesions were asymptomatic because of immunosuppressive treatment, found accidentally, and first suspected to be neoplastic. Pulmonary, splenic, mesorectal, and subcutaneous lesions showed rapid evolution in parallel with skin lesions, which strongly supported the diagnosis of visceral PG.
Due to the highly aggressive course of the disease, the patient received most of available treatments: prednisone, cyclosporine A, intravenous immunoglobulins, infliximab, methotrexate, mycophenolate mofetil, etanercept, dapsone, sulfamethoxazole‑trimetoprim (cotrimoxazole), azathioprine, cyclophosphamide administered intravenously in pulses, and adalimumab (approved by the local bioethics committee), always in combination (Supplementary material, Table S1).
Extracutaneous PG is potentially fatal and extremely difficult to diagnose. Disease awareness among clinicians, radiologists, and pathologists is fundamental and both diagnosis and treatment require a multidisciplinary approach.
- Gade M, Studstrup F, Andersen AK, et al. Pulmonary manifestations of pyoderma gangrenosum: 2 cases and a review of the literature. Respir Med. 2015; 109: 443‑450. | Crossref
- Wang JY, French LE, Shear NH, et al. Drug‑induced pyoderma gangrenosum: a review. Am J Clin Dermatol. 2018; 19: 67‑77. | Crossref
- Alavi A, French LE, Davis MD, et al. Pyoderma gangrenosum: an update on pathophysiology, diagnosis and treatment. Am J Clin Dermatol. 2017; 18: 355‑372. | Crossref
- McKenzie F, Cash D, Gupta A, et al. Biologic and small‑molecule medications in the management of pyoderma gangrenosum. J Dermatolog Treat. 2019; 30: 264‑276. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION