Telehealth visits in a tertiary cardiovascular center as a response of the healthcare system to the severe acute respiratory syndrome coronavirus 2 pandemic in Poland



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Telehealth visits in a tertiary cardiovascular center as a response of the healthcare system to the severe acute respiratory syndrome coronavirus 2 pandemic in Poland
Introduction
With a rapidly growing number of patients infected with severe acute respiratory syndrome coronavirus 2 (SARS‑CoV‑2) spreading across the globe, the World Health Organization called this infection a pandemic.1 To cope with the outbreak, some modifications in the current healthcare system needed to be made immediately.
Telehealth systems seem to be ideally suited to face the necessity of interpersonal separation, as the crucial factor inhibiting the spread of the virus is social distancing defined as the reduction of the number and frequency of interpersonal contacts.2 A telehealth system enables physicians to assess the condition of patients with confirmed or suspected infection and to properly guide their future diagnostic and therapeutic pathway. In healthy individuals, especially those at higher risk of infection (such as the elderly with multiple comorbidities), it helps to provide them with continuous care, without increasing their risk of infection, which may occur during an in‑person visit.
The aim of this study was to analyze the 3‑week period of telehealth visits introduced to cope with the SARS‑CoV‑2 pandemic in the outpatient clinic of the Silesian Center for Heart Diseases in Zabrze, a tertiary cardiovascular center in Poland.
Methods
On March 13, 2020, the Polish Ministry of Health enabled the primary healthcare provider, the National Health Fund (Polish, Narodowy Fundusz Zdrowia [NFZ]) to reimburse telehealth visits performed in the country. As soon as this decision had been issued, the administrative personnel of the outpatient clinic of our center contacted each patient who had a scheduled visit in our clinic and informed them about the possibility of a telehealth visit instead of an in‑person consultation. All patients with scheduled in‑person visits were notified, excluding only those who did not report their phone numbers to the hospital records. If the patient had not provided the phone number, the originally scheduled in‑patient visit was conducted. Having obtained the patient’s consent, the physician who was supposed to perform the original visit contacted the patient by phone and performed a televisit at the time of the originally scheduled in‑person visit. In the case of worsening of the patient’s condition, the patient was encouraged to visit the outpatient clinic in person. Each of 106 physicians employed in the outpatient clinic were obliged to perform televisits at the time of originally scheduled in‑person visits.
The clinic is situated in the heart of the most highly urbanized region in Poland and its catchment area exceeds 3 million of inhabitants, with the average distance of patients commuting regularly to the clinic oscillating around 10 kilometers. The 3 primary specialties of the outpatient clinic are cardiology, cardiothoracic surgery, and transplantology. The prospective electronic database including patients’ records was analyzed retrospectively. All consecutive patients registered in our outpatient clinic database from the day of telehealth visit introduction (March 16, 2020) until the day of this analysis (April 3, 2020) were included in the study. The patients who had been admitted to the outpatient clinic in the corresponding period a year before were also included for comparison with the current year.
Based on digital records, the clinical diagnoses were obtained according to the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, and the procedures performed during the visits were classified according to the International Classification of Diseases, Ninth Revision.
Statistical analysis
Study subpopulations were compared using the χ2 test for categorical variables and the Mann–Whitney test for continuous variables owing to their nonnormal distribution assessed with the Shapiro–Wilk test. A 2‑sided P value less than 0.05 was considered significant. The Statistica software, version 10 (StatSoft, Inc., Tulsa, Oklahoma, United States), was used for analysis.
Results
In the analyzed period (between March 16, 2020 and April 3, 2020), there were 2368 televisits and 367 in‑person visits (a total of 2735 visits), hence televisits comprised 86.6% of all visits (Figure 1A). The mean age of patients consulted remotely was 65.2 years (median [interquartile range (IQR)], 67 [57–76]years) and that of those undergoing an in‑person visit was 65 years (median [IQR], 68 [59–75]years). In total, 1066 women (45%) and 1302 men (55%) had a televisit, while 219 men (59.7%) and 148 women (40.3%) visited the clinic in person. Of those, 28% of the patients presented for routine cardiac implantable electronic device (CIED) follow‑up.
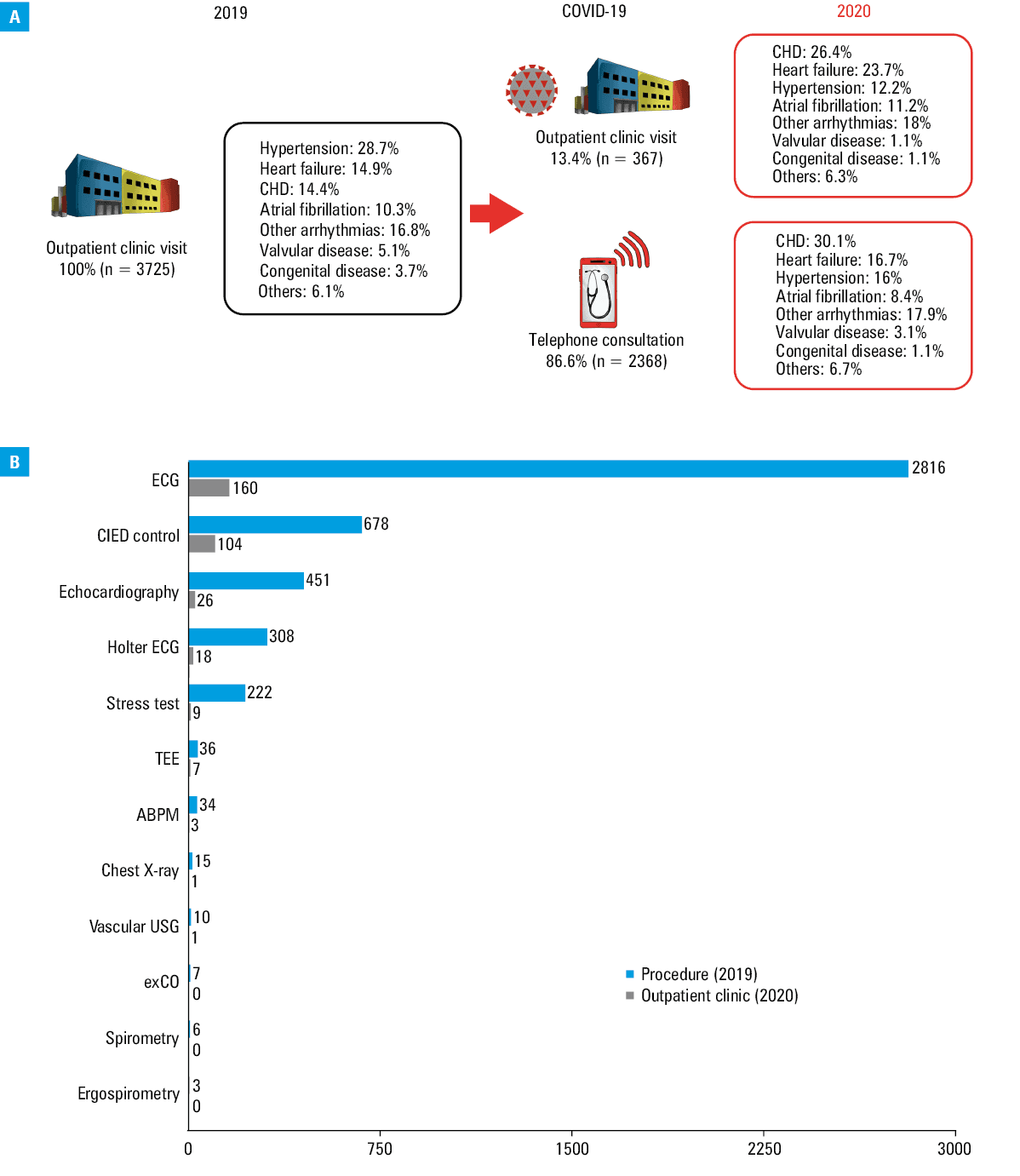
In the corresponding period in 2019, 3725 patients visited the clinic in person, of whom men constituted 52.9%, which was significantly higher than in 2020 (P <0.001). The mean age of that population was 63.5 years (64 years in men; 62.9 years in women), while the median (IQR) age of the overall group was 67 (56–64) years, which was significantly higher than in 2020 (P <0.001). No significant age differences between sexes were observed both in 2019 and in 2020. In 2019, the proportion of patients who underwent CIED follow‑up was 18.2%.
In comparison with 2019, the total number of clinic visits in 2020 decreased by 990 (26%). While electrocardiography was performed in 43.6% of the patients, and echocardiography in 7.1% in 2020, those numbers differed in 2019, with 75.6% and 12.1%, respectively. However, the purpose of some televisits performed in 2020 was to inform the patient about the results of the previously performed examinations and to discuss the future diagnostic workup and treatment strategies.
The clinical profile of patients treated in 2019 and 2020 differed between the groups, with the majority of patients who underwent televisits suffering from coronary heart disease (30.1%), heart failure (16.7%), and non–atrial‑fibrillation arrhythmias (17.9%), while the group of patients who visited the clinic in person had a significantly higher incidence of heart failure (23.7%) yet a lower incidence of coronary heart disease (26.4%; P <0.001).
In the analyzed period, the number of almost all procedures that had been routinely performed a year before were significantly decreased or suspended due to the epidemic (Figure 1B).
Discussion
Even before the pandemic outbreak, the alternative forms of contact between the doctor and the patient were analyzed and attempted. The first such institutionally organized service was started by the North Atlantic Treaty Organization to provide help for its soldiers operating in various regions of the globe.3 In following years, various telehealth systems were introduced, allowing for an alternative form of contact between the physician and local communities.4,5 However, except for extraordinary situations, its utilization remains very low, often not exceeding 1% of all visits.6 The factors contributing to such state can be an inadequately organized healthcare system, physicians’ unwillingness to implement telehealth strategies in their daily practice, or its insufficient reimbursement by healthcare providers.7
Without any doubt, the extraordinary conditions, such as the occurrence of a natural disaster or an epidemic, significantly alter the general approach to telehealth in order to safely and continually reach large numbers of patients in need for consultation, while maintaining their secure isolation and epidemiologic safety of their homes. To the best of our knowledge, there are currently no large‑scale data regarding outpatient clinics at the time of the pandemic.
In cardiovascular medicine, significant milestones in the field of telehealth have already been reached, including detection of arrhythmias with the use of a smartwatch,8 transmission of electrocardiographic recordings by medical rescue teams helping patients with suspected myocardial infarction,9 and, finally, remote monitoring of specific patient subgroups, including those with CIEDs.10 Such an approach, as indicated in our previous studies, can significantly improve the outcomes and patients’ quality of life.11,12
Nonetheless, in the routine daily practice, telehealth strategies were mostly considered as a valuable addition to standard treatment, with each patient being able to present for an in‑person examination in emergency. In the era of the pandemic, the possibility to offer such strategies remains elusive, as the efforts should be made to maximally reduce direct interpersonal encounters. Moreover, an important group of patients in whom televisits may be an inappropriate solution are those presenting to the clinic for the first time, in whom the proper assessment of their health status and extensive diagnostic workup seem to be difficult to perform during a remote visit.
Of note, the majority of patients gladly accepted the newly introduced form of visit in our clinic, but many of them underlined the temporariness of such an approach during telephone conversation, which, in their opinion, should not be the standard of care in cardiovascular medicine. In our opinion, after the cessation of the SARS‑CoV‑2 epidemic, televisits would be an appropriate solution in stable patients who would be able to undergo an in‑person visit in case of deterioration.
Conclusions
In the crisis situation related to the SARS‑CoV‑2 pandemic, telehealth visits enabled both patients and physicians to maintain the continuity of care due to cardiovascular diseases. The assessment of the safety of the advice provided will be possible after further assessment of adverse events in patients with cardiovascular diseases.
- World Health Organization. WHO Director‑General’s opening remarks at the media briefing on COVID‑19. March 11, 2020. https://www.who.int/dg/speeches/detail/who‑director‑general‑s‑opening‑remarks‑at‑the‑media‑briefing‑on‑covid‑19–-11‑may‑2020. Accessed March 8, 2020.
- Public Health England. Coronavirus (COVID‑19): what is social distancing? https://publichealthmatters.blog.gov.uk/2020/03/04/coronavirus‑covid‑19‑what‑is‑social‑distancing. Accessed March 8, 2020.
- Doarn, CR, Latifi, R, Poropatich, RK, et al. Development and validation of telemedicine for disaster response: the North Atlantic Treaty Organization multinational system. Telemed J E Health. 2018; 24: 657‑668. | Crossref
- Wicklund, E. Harvey’s aftermath brings mHealth, telehealth to the forefront. https://mhealthintelligence.com/news/harveys‑aftermath‑brings‑mhealth‑telehealth‑to‑the‑forefront. Published 2017. Accessed March 8, 2020.
- Zhao J, Zhang Z, Guo H, et al. E‑health in China: challenges, initial directions, and experience. Telemed J E Health. 2010; 16: 344‑349. | Crossref
ARTICLE INFORMATION