Isolated subsegmental pulmonary embolism: current therapeutic challenges
Key words: anticoagulation, isolated subsegmental pulmonary embolism, subsegmental pulmonary embolism, treatment



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Isolated subsegmental pulmonary embolism: current therapeutic challenges
The advent of computed tomography pulmonary angiography allowed better visualization of peripheral vessels, thereby increasing rates of subsegmental pulmonary embolism (SSPE), but there are minimal changes in mortality. The true clinical significance of SSPE and isolated SSPE (ISSPE) remains unclear. Patients with small pulmonary embolism (PE) usually present with chest pain or no symptoms, frequently classified as having a low clinical probability of PE. Those with central embolism, on the other hand, present dyspnea as the most common symptom. It is possible that ISSPE could represent a subset of a more benign disease and be not clinically relevant among patients with PE. There is a therapeutic dilemma in patients with small PE: should anticoagulation be used or not in all cases? As there are limited data to guide the appropriate management of ISSPE, this short review addresses the controversy over the therapeutic challenges in SSPE and ISSPE.
Introduction
Pulmonary embolism (PE) is the third most common cause of death among cardiovascular diseases, after coronary artery disease and stroke. It is associated with multiple inherited and acquired risk factors as well as advanced age.1 Acute PE causes 300 000 deaths each year with the annual incidence estimated as 1 episode per 1000 patients in the United States, and despite that, the diagnosis frequently is not made until the autopsy.1,2 Approximately 79% of patients with PE present deep vein thrombosis (DVT) in their lower limbs. Conversely, PE occurs in up to 50% of patients with proximal DVT.1
The clinical manifestation of PE is commonly nonspecific, making the diagnosis a challenge. Clinical presentation ranges from mild dyspnea, sustained hypotension to shock causing immediate death due to right ventricular failure. Sometimes it may even be asymptomatic and diagnosed incidentally on imaging performed for causes other than suspected PE.1-4
Advances in computed tomography pulmonary angiography (CTPA) in the early 1990s and its use as the technique of choice in the diagnostic workup of PE provided a foundation for innovations in the approach to PE and changed the assessment of patients with suspected PE.2 Since then, CTPA has widely replaced other diagnostic modalities for PE such as ventilation / perfusion (V / Q) lung scans and invasive pulmonary angiography.3
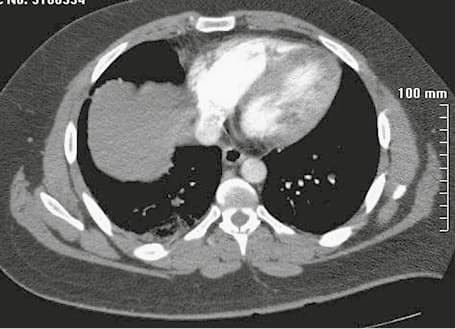
The use of multidetector CTPA (MDCT) instead of single‑detector CTPA (SDCT) reduced section thicknesses and scanning times, substantially improving resolution of peripheral vessels. This, in turn, improved the sensitivity of PE diagnosis by allowing high‑quality workstations and more effective detection of perfusion defects in pulmonary arteries as small as 1 to 3 mm in diameter, thereby leading to higher rates of subsegmental pulmonary embolism (SSPE) (figure 1).3,5
SSPE is expected to become an even more common diagnosis in patients with suspected PE. The rate of SSPE ranges from 4.7% by SDCT, to 15% by 64‑slice MDCT.2 Furthermore, the unsuitable use of CTPA became a facilitator of overtesting for PE, this is, despite several guidelines and algorithms for suspicious PE, there is a large body of evidence that CTPA is inappropriately ordered even in patients at low risk of PE.1-3
Previously, SSPEs were reported to be frequent among patients with suspected PE and nondiagnostic V / Q lung scans. In the PIOPED (Prospective Evaluation of Pulmonary Embolism Diagnosis) study, 17% of patients with a low probability V / Q lung scan were diagnosed as SSPE on pulmonary angiography. Therefore, it is plausible to assume that many patients with SSPE on MDCT had a nondiagnostic V / Q lung scan.2-4
Historically, patients with PE are equally anticoagulated regardless of size, quantity, and location of the thrombus since there is no proven hemodynamic instability. However, from 1998 to 2006, despite a 81% increase in the PE diagnosis rate in the United States (from 62.1 to 112.3 per 100 000 adults), there was no concomitant reduction in the mortality rate (fatal PE / US population) (3% reduction, from 12.3 to 11.9 per 100 000 adults).3 Besides, the case fatality (fatal PE / PE diagnosis) due to PE decreased from 12.1% to 7.8%, suggesting that most of diagnosed PE might be associated with a lower severity of illness, and a similar reduction in mortality by effective treatment was not demonstrated in the general population.4
Moreover, previous studies have suggested that the positive predictive value of CTPA for SSPE in patients at the emergency department may be only 25%. Likewise, the interobserver agreement for SSPE among radiologists with varied levels of experience is low (κ of 0.38; 95% CI, 0–0.89), and there is a high rate of inaccuracy for small pulmonary artery defects caused by motion and streak artifacts or other nonthrombotic material as the imaging pitfalls with uncertain clinical significance.4,6 Thus, the probability of a false‑positive interpretation for PE increases with more peripheral location and decreasing short‑axis diameter of the lesion ranging a maximum of 4% of subsegmental lesions compared with 0.8% of central lesions.7
The specificity of the CTPA varies according to the size of vessels, for proximal branches of the pulmonary artery it is near 100%, and 37% to 46% for SSPE.8 It was reported that 11% to 59% of SSPEs were considered negative on reinterpretation for PE.8,9 Similarly, another study including reinterpretations by 5 radiologists reported that for small PE, at least 1 radiologist disagreed with the initial interpretation in 60% of the cases.7
In fact, a decrease in examination quality led to an increase in the incidence of false‑positive interpretations. This also rises concerns about overdiagnosis and overtreatment at the same time, since some patients are anticoagulated unnecessarily with increased detection of incidental SSPE.8 Therefore, it is prudent that the interpretation for confident diagnosis of SSPE should only be made if multiple experienced radiologists agree on the presence of an embolism to avoid unnecessary anticoagulation.7
In contrast, due to absence of classic symptoms such as sudden dyspnea, chest pain, and hemoptysis, especially in patients with confounding factors, for example, coexistent cardiorespiratory diseases, PE is one of the most commonly missed or delayed diagnoses in daily clinical practice.3,4 Obviously, absence of characteristic symptoms does not exclude PE.
Isolated subsegmental pulmonary embolism (ISSPE) (figure 2) is defined as PE shown on CTPA with 1 or more pulmonary artery filling defects located in the subsegmental branch, with no filling defects visualized at more proximal pulmonary artery levels.10 The ISSPE rate reported in the literature ranges from 4% to 9.4% of all CTPAs.2,11-13

Clinical characteristics of isolated subsegmental pulmonary embolism
The true clinical impact and significance of ISSPE remain debatable. Patients with small PE usually present with chest pain or are asymptomatic, frequently classified as low clinical probability for PE, whereas those with central embolism present with dyspnea as the most common symptom.14
Besides, patients with peripheral PE present lower plasma levels of biomarkers (N‑terminal pro–brain natriuretic peptide, creatine kinase MB, troponin I), are hemodynamically stable, and show less changes on echocardiography and echocardiographic parameters, which contribute to low clinical suspicion and low PE diagnosis.15
One of the roles of the pulmonary circulation is to preclude small clots from entering the lower extremities to reach the systemic circulation, acting as a filter in a benign “clearing” process occurring in the lungs. It is believed that such distal clots may occur even in healthy people without symptoms.16,17 Such PE patients would be absolutely asymptomatic and many small PE may be a normal part of existence and may remain unrecognized until identified by CTPA that would not have been fatal even if left undiagnosed and untreated.10 Thus, in theory, anticoagulation in these cases would be dispensable.
Therefore, it is possible that ISSPEs could represent a subset of more benign diseases which are nonclinically relevant among patients with PE. Indeed, at 3‑month follow‑up, the majority of the untreated patients with ISSPE without DVT of the lower extremities did not experience significant bleeding, recurrence, or death.2,18
A systematic review conducted by Bariteau et al19 found that the frequency of bleeding in patients with SSPE treated with anticoagulation was 8.1%. The frequency of venous thromboembolism (VTE) recurrence at 3‑month follow‑up was 5.3% in treated patients as compared with 3.9% in untreated, whereas the frequency of death was 2.1% in treated as compared with 3% in untreated. Those data suggest that in this subgroup of patients, the clinical outcomes are comparable between patients with a distinct strategy of management. Therefore, no plausible conclusion can be made about the risk‑benefit ratio of anticoagulation therapy in SSPE.
Another important point is concomitant DVT as an independent prognostic factor of death in PE. In a cohort study, Jiménez et al20 reported that of 707 patients with the first episode of acute PE, all‑cause mortality (hazard ratio [HR], 2.05; 95% CI, 1.24–3.38; P = 0.005) and PE‑specific mortality (HR, 4.25; 95% CI, 1.61–11.25; P = 0.04) were both significantly higher in patients with concomitant DVT in the subsequent 3 months after the diagnosis.
Patients with PE limited to small branches often do not have DVT of the lower limbs.10 On the other hand, Le Gal et al21reported that concomitant DVT in SSPE was lower than in patients with more proximal PE (7.1%; 95% CI, 1.2%–31.5% vs 41.8%; 95% CI, 34.5%–49.1%). Accordingly, it is prudent to exclude DVT by ultrasonography of veins of the lower limb in those patients, especially if it is planned to withhold anticoagulation.19,21
Incidental (“silent”) pulmonary embolism and cancer
Incidental PE is defined as a filling defect of 1 or more pulmonary arteries shown on computed tomography (CT) performed for cancer staging and for reasons other than the diagnostic workup of PE. As opposed to SSPE, these lesions are typically asymptomatic.20 Whether all incidental PE should be treated in the same manner as classic PE is unclear.
Interestingly, incidental or silent PE is associated with a significant risk of recurrence of VTE even in anticoagulant treatment. Some asymptomatic patients with PE and proven lower limb DVT tend to have more frequent proximal and unprovoked DVT.22
Incidental PE has been gradually identified on CT images, but still remains a management challenge for clinicians because its clinical significance is unclear. Patients with incidental PE are usually asymptomatic and previous autopsy studies have reported rates of incidental PE ranging from 9% to 63% but not related to the main cause of death.23-26 In fact, some patients with underdiagnosed and untreated PE may not have an unfavorable outcome.27 The available literature focusses mostly on incidental PE in patients with cancer, but it is also clearly relevant to other groups, including those referred for coronary artery imaging, evaluation of pulmonary infections, pulmonary nodule, or those had major trauma.28
Of all incidental PE cases, nearly 11% to 27% are located in peripheral vessels and half of them occur in proximal arteries.29,30 However, the thrombus size does not seem to influence mortality, although the proximal incidental PE location appears to adversely impact the outcome.31,32
Patients with cancer are routinely subjected to chest CT scans to evaluate the magnitude of the malignancy and the response to treatment or to screen for metastases. With such a widespread use of the diagnostic tool, the detection of incidental PE became progressively common. Unsuspected emboli are found in 4% of patients overall, in 17% of patients over age 80 years, and in 24% of asymptomatic trauma patients.3 Moreover, 50% to 60% of consecutive autopsied patients were found to have incidental PE when the pulmonary vessels were carefully examined.33
It is uncertain whether incidental PE may be related to malignancy and all patients with cancer are predisposed to PE. Ritchie et al34 found no significant difference in the prevalence of incidental PE among patients with a history of cancer and those without cancer. However, incidental PE in cancer patients may be just the tip of the iceberg.
Cancer increases the risk of VTE, which includes DVT and PE, but patients with metastatic cancer are at a higher risk than those with limited active cancer, who are also at a higher risk than those with cancer in remission.28 Furthermore, the association of cancer and VTE increases 3‑fold the risk of death compared with cancer but no VTE.32,34 Apart from that, thrombotic events and VTE were the second leading causes of death in cancer patients accounting for 9.2% of all deaths in cancer patients receiving chemotherapy.35
The frequency of incidental PE on all CT images is 1.1%. Especially in cancer, it varies from 2.6% in more advanced CT scan machines to 3.6% in SDCT by 64‑slice MDCT.36 It is remarkable that subsegmental incidental PE is detected more often, as the use of more advanced CT scan machines increases.8,36
A meta‑analysis by Van der Hulle et al37 included 926 patients with cancer and incidental PE. A total of 42 (4.5%) did not receive any anticoagulants due to a high risk of bleeding or other relevant prognostic factors. In this group of patients, a higher risk of major bleeding, recurrent VTE, and 6‑month mortality were reported in 6.4%, 12%, and 47% of patients, respectively.
A cohort study by O’Connell et al38 showed that 70 symptomatic cancer patients with diagnosed incidental PE on routine staging scans had poorer survival (mean 8 months) as compared with 137 (mean 12 months) age- and stage‑matched control subjects. In patients with malignancy, the risk of recurrent VTE is significant even in those on anticoagulant therapy. Patients with SSPE also seem to have a higher risk of recurrent VTE than patients with proximal PE.39
Sun et al40 reported that anticoagulant therapy was significantly associated with increasing survival in patients with lung cancer and incidental PE compared with patients who did not receive anticoagulant therapy. Those who did not receive therapy had a median survival of 6.1 months compared with 30.9 months in patients who did.
Based on retrospective studies, there is a general consensus that the prognosis of incidental PE in cancer is similar to that of symptomatic PE regarding the risk of recurrent VTE and mortality. These evidences reinforce anticoagulant therapy importance in patients with incidental PE and cancer.36
The European Society of Cardiology and American Society of Clinical Oncology (informal consensus, moderate strength of recommendation) recommend that for cancer patients with incidental PE, the management should be the same as for symptomatic PE if it involves segmental or more proximal vessels, multiple subsegmental vessels, or a single subsegmental vessel in association with DVT.41,42
Treatment of isolated subsegmental pulmonary embolism
Anticoagulation therapy clearly improves survival in patients with symptomatic PE, but the risk of recurrent nonfatal VTE is near 5% to 10% during the first‑year after the diagnosis.1 Carrier et al,43 in their systematic review, reported the rate of fatal major bleeding events of 0.2% (95% CI, 0.1%–0.3%), with a case‑fatality rate of 11.3% (95% CI, 7.5%–15.9%). These rates of major bleeding episodes are associated with vitamin K antagonists. It is questionable whether these same risks are suitable for patients taking direct oral anticoagulants, which have a significantly better safety profile.37
However, there is a dilemma whether all patients with ISSPE should be anticoagulated or not. There are limited data to guide the appropriate management of ISSPE. In a recent systemic review, Yoo et al44 reported that there are no randomized controlled trials to assess the effectiveness and safety of anticoagulation therapy versus control in patients with ISSPE or even incidental SSPE.
Previous retrospective data are conflicting whether it may be safe to withhold anticoagulation in patients with ISSPE. However, likely due to ethical reasons and questionable outcomes, most patients diagnosed with PE are still anticoagulated, regardless of their clinical presentation and thrombus size or location.44
Bariteau et al19 reported in a systematic review that there is no clear inference about risk‑benefit ratio of anticoagulation for SSPE. That is due to lack of precision of uncontrolled outcome studies regarding VTE recurrence or death rates in patients who were not anticoagulated.
The risk of recurrent venous thrombotic disease and mortality seems to be similar for incidental PE and SSPE clinically suspected SSPE, if untreated. Donato et al18 found in a cohort study that in patients with untreated SSPE, recurrence and mortality were 0% at 3‑month follow‑up. These results are similar to those demonstrated by Moores et al,45 1.4% and 0.5%, respectively. However, patients with SSPE are far more likely to experience complications due to anticoagulation than adverse outcomes from the embolism itself.18 Thus, every year, 3% of anticoagulated patients experience a major bleeding episode that requires medical care (cerebral hemorrhage, gastrointestinal bleeding, or bleeding following trauma).1,2,37,41
A study evaluating the accuracy of the enzyme‑linked immunosorbent assay (ELISA) D‑dimer test for the exclusion of PE in patients with suspected PE has reported that sensitivity of the measurement is not sufficient (76%) in patients with SSPE on pulmonary angiography,46 inferring that most patients with suspected PE and negative D‑dimer might have undiagnosed SSPE. Therefore, the combination of a negative ELISA D‑dimer test result and a non‑high pretest probability can efficiently and safely rule out PE without the use of CTPA. These “undiagnosed” SSPEs are likely untreated without any adverse outcome.5,47
To avoid unnecessary radiation exposure and overdiagnosis, the YEARS algorithm has been proposed by using a validated D‑dimer threshold of 500 ng/ml in presence, and 1000 ng/ml in absence of 3 items of the Wells clinical decision rule (clinical signs of deep vein thrombosis, hemoptysis, “PE as the most likely diagnosis”). This new algorithm proposal safely ruled out acute PE in patients with clinically suspected PE and a low risk of VTE at 3‑month follow‑up (0.61%, 95% CI 0.36–0.96) and a resultant 14% absolute reduction of CTPA compared with the standard algorithm with the conventional Wells rule and a fixed D‑dimer threshold of less than 500 ng/ml.48
However, a lower prevalence of ISSPE was reported according to the YEARS algorithm compared with a traditional algorithm (absolute difference, 6.2%; 95% CI, 1.4–10; odds ratio, 0.58; 95 CI, 0.37–0.90) as a consequence of lower sensitivity of YEARS for small PE due to the higher D‑dimer threshold. Nevertheless, this reduction was not associated with a higher risk of recurrent VTE among untreated patients during 3‑month follow‑up.49
Of note, a strong correlation between plasma D‑dimer levels and thrombus location was previously described, namely, ISSPE is associated with a lower median D‑dimer level than more proximal PE.50,51 Furthermore, the accuracy of a D‑dimer measurement to exclude PE depends fundamentally on the PE location. Thus, the D‑dimer measurement can miss subsegmental PE. It is, however, unclear whether these small PE really need anticoagulant treatment.50
Another important point for discussion is the cardiopulmonary condition that influences the outcome of patients with PE. A study conducted by Hull et al52 compared 117 patients with poor cardiopulmonary reserve and 627 patients with good reserve. All patients had low or moderate probability V / Q lung scans and no proven DVT of the lower limbs. Recurrent VTE was reported in 12 patients (10%) in the poor cardiopulmonary reserve group and in 12 (2%) in the good reserve one.
Kroegel and Reissig53 highlighted that a fatal outcome of PE is 4- to 7‑fold more likely in patients with preexisting cardiopulmonary disease than healthy individuals. Furthermore, it is important to consider some factors that might influence the decision to anticoagulate or not, including patient preference, unprovoked clot, severe symptoms, and presence of active malignancy.54
Clinicians have a tendency to anticoagulate all patients with PE, regardless of thrombus size and clinical repercussion. However, it is important to consider that anticoagulant therapeutic is not without risks, and serious undesirable intracranial and gastrointestinal bleeding complications can occur. These issues should be addressed with all patients with PE who receive anticoagulation. However, for patients with ISSPE—especially those who are at a high risk of bleeding—clinical surveillance should be considered instead of treatment (after excluding simultaneous DVT). In such cases, patient preferences should be an important element of the shared decision‑making process.2,55
There are some conditions with an increased risk of recurrent VTE that favor anticoagulant treatment in patients with SSPE: hospitalization or reduced mobility due to other reasons; active cancer (metastatic or in chemotherapy); no reversible risk factor for VTE, such as recent surgery; poor cardiopulmonary reserve, or significant symptoms that cannot be attributed to another condition.2,10,55
On the other hand, if the SSPE is a single injury (ISSPE), DVT is not present, and the patient has no symptoms related to PE, anticoagulant therapy can be postponed.2,7,55
The European Society of Cardiology guidelines41 do not supply specific management recommendations about ISSPE, other than suggesting to confirm the image findings with an experienced radiologist. On the other hand, the American College of Chest Physicians guidelines suggest close follow‑up of anticoagulant therapy in patients with SSPE in specific conditions such as: 1) no DVT excluded by serial doppler ultrasonography imaging of the lower limbs; 2) high risk of bleeding (intracranial hemorrhage, recent surgery, or trauma); 3) no high risk factors for recurrent or progressive VTE (such as hospitalized patients, reduced mobility, and malignancy); and 4) good cardiopulmonary reserve (evidence grade 2C).55
The American College of Emergency Physicians issued a “Clinical Policy” on the management of PE and DVT that included the following statement: “given the lack of evidence, anticoagulation treatment decisions for patients with SSPE without associated DVT should be guided by individual patient risk profiles and preferences.”56
Conclusions
There is no consistent consensus from randomized controlled trials for the decision on whether to treat or not patients with SSPE and ISSPE (and no DVT), and a case‑by‑case decision making is therefore recommended, especially when the patient is included in the decision‑making. However, in patients with malignancy, small PE seems to be associated with VTE recurrence and adversely impact survival.
The American Society of Clinical Oncology (informal consensus, moderate strength recommendation) recommends that in patients with cancer and incidental PE, the management should be the same as in symptomatic PE. The American College of Chest Physicians guidelines suggest clinical surveillance of anticoagulant therapy in low‑risk patients with SSPE in specific conditions such as: no DVT excluded by serial doppler ultrasonography imaging of the lower limbs; high risk of bleeding; no high‑risk factors for recurrent or progressive VTE. The American College of Emergency Physicians suggest that given lack of evidence, anticoagulation treatment decisions for patients with SSPE without associated DVT should be guided by individual patient risk profiles and preferences.
And also it is prudent that all interpretation of reliable diagnosis for SSPE should only be performed if multiple experienced radiologists agree on the presence of an embolism to avoid unnecessary anticoagulation.
- Tapson VF. Acute pulmonary embolism. N Engl J Med. 2008; 358: 1037‑1052. | Crossref
- Carrier M, Righini M, Wells PS, et al. Subsegmental pulmonary embolism diagnosed by computed tomography: incidence and clinical implications. A systematic review and meta‐analysis of the management outcome studies. J Thromb Haemost. 2010; 8:1716‑1722. | Crossref
- Wiener RS, Schwartz LM, Woloshin S. Time trends in pulmonary embolism in the United States: evidence of overdiagnosis. Arch Intern Med. 2011; 171: 831‑837. | Crossref
- Dobler CC. Overdiagnosis of pulmonary embolism: definition, causes and implications. Breathe. 2019; 15: 46‑53. | Crossref
- Perrier A, Roy PM, Sanchez O, et al. Multidetector‑row computed tomography in suspected pulmonary embolism. N Engl J Med. 2005; 352: 1760‑1768. | Crossref
ARTICLE INFORMATION