Acute kidney injury, its definition, and treatment in adults: guidelines and reality
Key words: acute kidney injury, creatinine, glomerular filtration rate, renal replacement therapy



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Acute kidney injury, its definition, and treatment in adults: guidelines and reality
In the last decades, a lot of research has been done to improve our understanding of acute kidney injury (AKI) as well to standardize its diagnostic criteria. As a result of many years of work of intensivists and nephrologists, consensus definitions were established, finally unified in 2012 by the Kidney Disease: Improving Global Outcomes (KDIGO) group. These criteria refer to the time of AKI development and are based on serum creatinine level increase and / or urine output decrease. Acute kidney injury is defined as an increase in serum creatinine levels by at least 0.3 mg/dl within 48 hours or 1.5‑fold the baseline, which is known or presumed to have occurred within the preceding 7 days, or—according to the urine output criterion—urine volume less than 0.5 ml/kg/hour for at least 6 hours. The present review covers issues discussed during the KDIGO controversy conference, devoted to AKI. Here, we attempted to answer 3 main questions: Is the KDIGO definition of AKI valuable in clinical research and global epidemiology? Is it helpful in everyday clinical practice? Is it useful in the treatment of critically ill patients with AKI?
Introduction
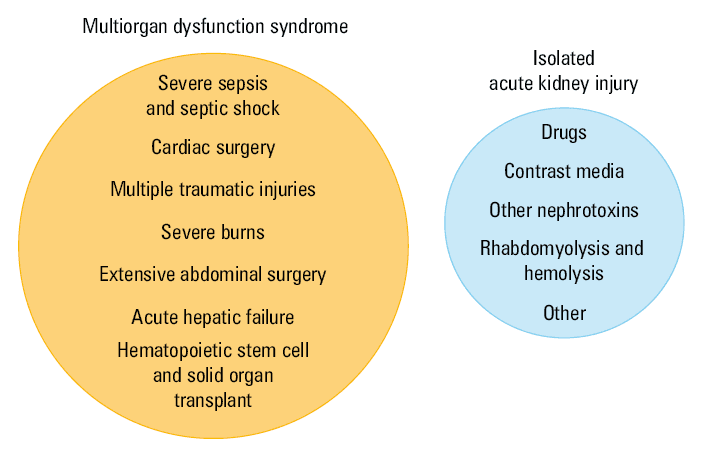
Over the past decades, there has been a significant increase in the incidence of acute kidney injury (AKI),1 especially in the older population (>65 years). The number of AKI cases in the hospitalized population have more than doubled; it also concerns AKI requiring dialysis.2 At the same time, in high‑income countries, we have witnessed a profound change in the disease spectrum (Figure 1). It is a consequence of the spectacular progress in medicine, leading to a considerable life extension. In high‑income countries, AKI develops in up to 20% of hospitalized patients, which is approximately 50% of adult patients receiving intensive care, and in 1 in 4 pediatric patients receiving intensive care.3,4 In adults, it has become a disease of the older, who, with many comorbidities and chronic degenerative organ changes, are much more vulnerable to acute insults. Many of them have already had some form of chronic kidney disease (CKD), called “AKI on CKD.” Patients who survive extensive, high‑risk cardiovascular or abdominal surgery, extensive trauma, or burns and those after hematopoietic stem cell or solid organ transplant often develop sepsis and other complications. In many of them, AKI occurs as a late event, often as a manifestation of multiorgan dysfunction syndrome. Therefore, in the 1970s and 1980s, patients with severe AKI were treated mainly in general wards. Today, most of them are referred to intensive care units (ICUs). Such a change in the spectrum of AKI must have influenced patients’ survival; that is why mortality in severe AKI remains very high, despite several treatment improvements. In patients requiring renal replacement therapy (RRT), the overall 90‑day mortality ranges between 44% and 60%.5-7 Moreover, those who survive the hospitalization period are at risk of developing long‑term complications associated with a substantial cost burden. Recent studies have consistently shown that, in both adults and children, AKI and its stage is a strong, independent risk factor for CKD development.8,9 The mechanisms of progression from AKI to CKD have been partially elucidated in experimental studies. They include maladaptive repair and endothelial injury, which result in nephron and capillary dropout, interstitial fibrosis, and the progressive decline of glomerular filtration rate (GFR).10-12 In those with already existing CKD, AKI may significantly accelerate its progression to the end‑stage disease. Patients who recover from AKI also remain at higher risk of developing hypertension and cardiovascular events.10,13,14
In the last decades, much research has been conducted to improve our understanding of AKI as well to standardize its definition and diagnostic criteria. It was necessary, since there had been more than 35 definitions in use, based on various serum creatinine levels or its clearances obtained using different methods, precluding any data or study comparisons in the field. The first consensus definition of AKI, the Risk, Injury, Failure, Loss of kidney function, and End‑stage kidney disease (RIFLE) criteria, were published in 2003, as a joint work of intensivists and nephrologists,15 subsequently changed by the same group to the Acute Kidney Injury Network (AKIN) criteria 3 years later,16 and finally unified by the Kidney Disease: Improving Global Outcomes (KDIGO) group and published in 201217 (Table 1). The KDIGO criteria, or classification, refer to the time of AKI development and are based on serum creatinine level increase and / or urine output decrease. It is defined as an increase in serum creatinine levels at least by 0.3 mg/dl within 48 hours or 1.5‑fold the baseline, which is known or presumed to have occurred within the preceding 7 days, or—according to the urine output criterion—as urine volume below 0.5 ml/kg/hour for at least 6 hours.
Stage | Serum creatinine levels | Urine output |
Abbreviations: RRT, renal replacement therapy | ||
1 | 1.5–1.9‑fold higher than baseline or increase ≥0.3 mg/dl | <0.5 ml/kg/hr for 6–12 hrs |
2 | 2–2.9‑fold higher than baseline | <0.5 ml/kg/hr for ≥12 hrs |
3 | 3‑fold higher than baseline or increase ≥4 mg/dl, or initiation of RRT | <0.3 ml/kg/hr for ≥24 hrs or anuria for ≥12 hrs |
The KDIGO definition has been developed to achieve several objectives: to unify terminology, to facilitate research and comparability among studies, to raise the awareness of AKI among general practitioners and non‑nephrologists, to enable its earlier detection and, possibly, prevention, and, ultimately, to improve patient outcomes. Let us have a quick look at how it has fulfilled these goals.
Question 1: is the KDIGO definition of acute kidney injury valuable in clinical research and global epidemiology?
The answer is equivocal. From 2012, when it was introduced, the classification has been evaluated and validated in several studies and claimed by many as useful in comparing outcomes between AKI studies and interventions.18-22 The adoption of the KDIGO staging system also allowed for the standardization of entry criteria and endpoints in the clinical trials of AKI, although there have been numerous studies that used classification systems other than the KDIGO criteria.23-28
However, the question remains as to whether it is a reliable tool for the estimation of AKI global epidemiology? This issue has been a matter of a heated debate. Probably, the highest controversy is related to the possibility of diagnosing AKI based on the increase in serum creatinine levels ≥0.3 mg/dl within 48 hours. It was criticized by many as a too small alteration to eliminate laboratory errors or physiologic fluctuations, which may misclassify healthy patients as well as patients with CKD and baseline serum creatinine levels ≥1.5 mg/dl,29 in whom such small increases may represent normal daily variations. Another limitation of the KDIGO definition is the determination of a baseline creatinine level when the true value is unknown. None of the proposed methods seems to be reliable, and all of them may be the source of substantial errors. The incorporation of RRT initiation as a possible definition of stage 3 disease is maybe even more unfavorable, since this criterion is subjective.
The diuresis criterion, although reported to increase early AKI detection rates, has raised many doubts. Urine output is easy and inexpensive to determine, but it can be significantly changed by the use of diuretics, fluid therapy, and hemodynamic status. Therefore, it may increase diagnostic false‑positive rates. Of note, in patients who have undergone major surgical procedures, oliguria may be an appropriate physiological response to stress related to surgery. Also, the proposed threshold is controversial. As rightly pointed out by Erdbruegger and Okusa,30 in a 70‑kg adult man, diuresis ≤0.5 ml/kg/hour for 6 hours would represent a urine volume as high as 840 ml/d, which seems to be an adequate response to limited fluid intake. Last but not least, what about nonoliguric AKI?
However, in our opinion, the greatest uncertainty about the value of the KDIGO classification in clinical research is the fact that the definition does not differentiate between 2 extreme forms of AKI: the functional one, formerly called prerenal azotemia, and structural tubular injury. Prerenal kidney injury is not clearly defined by the KDIGO classification and seems often to be a neglected issue. Unfortunately, this may be a serious obstacle in the accurate estimation of AKI global epidemiology and should be overcome.
Many shortcomings of the KDIGO definition result from the fact that it is based on serum creatinine levels, which are imperfect biomarkers of AKI, being affected by numerous factors. In their excellent review, Thomas et al31 delineated as many as 14 various acute or chronic factors that may alter serum creatinine levels, making it difficult to establish an accurate diagnosis. The serum creatinine level is a functional marker, and its rise does not necessarily represent kidney injury. There are numerous examples of hemodynamically driven, transient serum creatinine elevations, like in patients with prerenal azotemia and hepatorenal or cardiorenal syndrome. In a number of these clinical situations, the kidney is not injured, and its response to reduced intravascular volume is homeostatic, thus, absolutely normal and can be life‑saving. However, tubular damage can occur in some situations, but it is insufficient to considerably change serum creatinine levels in the volume‑overloaded patient. The incorporation of structural biomarkers that directly indicate tubular damage could improve the diagnostic value of the AKI definition.
Several recent cardiologic studies have advocated the need to redefine AKI, which is often replaced in cardiology with the term “worsening renal function (WRF)” in patients with acute heart failure (HF), linking biochemical changes with clinical status.32-36 Worsening renal function that has occurred in the setting of acute HF is classified into 2 categories, ie, true and pseudo‑worsening renal function, by the extension of the RIFLE / AKIN criteria and combining them with the presence or absence of worsening HF.13,14,33,36 True WRF is diagnosed in patients with the simultaneous presence of worsening HF, defined as the deterioration or no improvement of HF that requires intensified therapy during the first 3 days of hospitalization. Those who demonstrate only isolated alterations in creatinine levels or eGFR are classified as having pseudo‑WRF. The rationale behind this distinction is that not every increase in serum creatinine levels in acute HF indicates kidney injury or dysfunction with unfavorable consequences, and an increase in creatinine levels with simultaneous effective decongestion and hemoconcentration is often related to better outcomes.33-35 Recently, Sokolski et al36 investigated the definition of true WRF in relation to clinical characteristics and outcomes in patients with acute HF. They found that while 14% of patients developed WRF during hospitalization, a change in creatinine or eGFR was associated with unfavorable clinical settings only in 4%. In the remaining 10%, the clinical course was uneventful and did not differ from that observed in patients without WRF. It may be of interest to compare WRF with the AKI definition proposed by the KDIGO group.
Unfortunately, despite extensive research, the uphill battle to find reliable structural biomarkers of AKI may last longer than we expect, provided they can ever be found. Therefore, we agree that the AKI definition endorsed by the KDIGO guidelines, with serum creatinine levels as the main parameter, remains the best option for clinical research. However, we should be aware of its weakness in the estimation of AKI global epidemiology, since it may be a potent source of mainly false‑positive results.
Considering epidemiological studies, one cannot forget that many of them use large administrative databases based on the International Classification of Diseases, Tenth Revision (ICD‑10) coding, which neither accounts for the current AKI definition nor distinguishes between various AKI stages. Moreover, as stressed by several researchers, changes in discharge coding practices, driven by reimbursement systems, may, in part, explain the dramatic rises in the incidence of AKI observed in some countries over the past 2 decades.37-39 The International Classification of Diseases, Eleventh Revision is on its way and is expected to replace ICD‑10 on January 1, 2022. It will be integrated with the KDIGO classification, including the current definition and differentiation between AKI stages. If and to what extent it will improve AKI identification remains unclear.
Question 2: is the KDIGO definition of acute kidney injury helpful in everyday clinical practice?
We do not think so. There are at least 3 crucial questions, which a clinician facing a patient with an abrupt worsening of kidney function should ask. Is the patient in a life‑threatening condition? What is (are) the most probable cause(s) of AKI? How should they manage the patient? The KDIGO definition leaves us without any answer to these issues. The reason for that is its complete lack of the clinical context, which can vary a lot, with entirely different forms of worsened kidney function such as hemodynamic AKI, blockage of urine flow, and a decrease in renal secretion due to tubular damage.
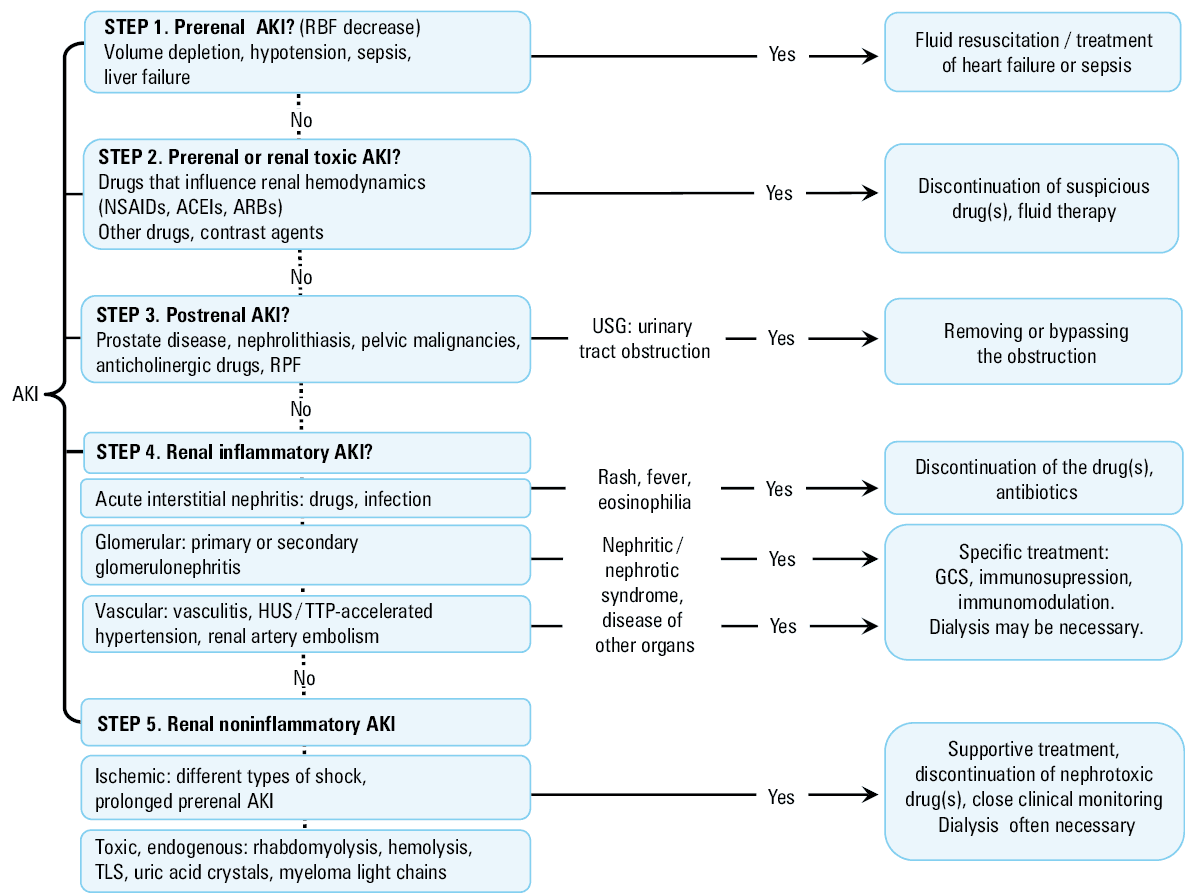
For this reason, in our practice, we prefer to use the old pathophysiological classification, which categorizes the causes of AKI into 3 groups: prerenal (renal hypoperfusion), postrenal (obstruction of the urinary tract), and intrinsic (structural damage to the kidney), which can be related to ischemia, nephrotoxins, or inflammatory processes. The strengths of this old approach lie in what remains the weakness of the RIFLE, AKIN, and KDIGO classifications, namely, limited complexity, memorability, and the relation to the etiology and pathophysiology of the condition. It determines the appropriate diagnostic steps and provides us with vital therapeutic suggestions. Therefore, when keeping in mind that this old classification simplifies a highly complex clinical syndrome and, in many cases, the pathogenesis of AKI is multifactorial, we still recommend its use to our students and trainees.
Although we do not find the KDIGO criteria much helpful in the everyday care of patients with AKI, we do recognize that there are some positive consequences of introducing them to clinical practice. Most importantly, it raised the awareness of AKI among physicians. The adoption of the consensus definition has enabled us to build electronic AKI alerts, similar to other healthcare information technology systems, coupled with hospital‑wide AKI guidelines and educational programs, warning clinicians of possible AKI and supporting them in implementing appropriate nephroprotective measures. These include the discontinuation of nephrotoxic agents, avoidance of diuretics and radiocontrast media, ensuring an adequate volume status, hemodynamic management in patients with hypotension, monitoring urine output and serum creatinine levels, as well as additional diagnostic workup (ie, urinalysis, kidney ultrasound). In numerous alert systems, when the patient is diagnosed with AKI, a request for nephrology consultation is automatically generated. Finally, these systems may identify candidates for appropriate outpatient follow‑up and monitoring for long‑term renal recovery after AKI. It remains unclear whether these systems will meet the expectations. The results of some studies, mostly from the United Kingdom, are inconsistent, with some of them showing an improvement in the care of patients with AKI, and others demonstrating no substantial benefit, the increased use of resources, and higher hospitalization rates.40-42
Question 3: is the KDIGO definition of acute kidney injury helpful in the treatment of critically ill patients with acute kidney injury?
In the treatment of critically ill patients, the clinical context matters most. The presence of sepsis, failure of other organs, and malnutrition may dramatically influence the outcome. The sequence of clinical events is also essential. In the case when AKI develops late, after ICU admission, as a manifestation of multiple organ failure, the prognosis seems to be much worse. Since these patients are often in a highly catabolic state, the development of metabolic disorders may rapidly progress and be accompanied by severe acidosis and hyperkalemia, while extensive fluid resuscitation and parenteral nutrition pose a risk of severe fluid overload. Of note, in critically ill patients, the severity of AKI can be underestimated due to dilution of serum creatinine by fluid accumulation, increased or decreased creatinine production, and loss of muscle mass, and may delay therapeutic decisions.
In ICU practice, the severity of renal failure is often evaluated by combining the functional parameters of the kidneys and other organs. In their recently published systematic review, da Hora Passos et al24 evaluated the criteria used to determine the severity and progression of kidney injury in multicenter randomized clinical trials conducted in ICUs, with mortality regarded as a primary outcome. Out of 46 studies, only 7 (15.2%) included mean or median serum creatinine levels. The Sequential Organ Failure Assessment (SOFA) renal score was the most commonly used system to define and quantify the frequency of AKI (43.5% of studies), while the RIFLE / AKIN / KDIGO criteria were used only in 5 trials (10.9%). The authors stated that their findings may raise concerns about the evidence‑based use of these classification systems in the clinical management of critically ill patients.
Initiation of renal replacement therapy
Classic indications for dialysis in AKI are well known; they are based mainly on the development of refractory to diuretics, life‑threatening fluid overload and severe solute imbalances, accompanied by hyperkalemia and acidosis. However, in the absence of these clearly urgent indications, the decision when to initiate RRT in critically ill patients with AKI is often much more difficult and—despite a remarkable progress in intensive care medicine during the last decades—remains a subject of controversy. Notably, although RRT is inevitable and life‑saving in many cases of severe AKI, it may also negatively impact the outcomes of these patients. Dialysis exposes them to (or aggravates the already present) hemodynamic instability with deleterious intradialytic hypotension, anticoagulation‑induced bleeding, vascular access–related bacteremia, and inflammatory stress due to bioincompatibility of an extracorporeal circuit. One of the key untoward effects of RRT is a not entirely predictable change in the pharmacokinetics of various therapeutic agents, especially antibiotics, posing a substantial risk of underdosing them.
The ongoing discussion entitled “early versus late”43-49 seems to be as passionate as a bit pointless, since what is early for one patient may be too late for another one. Recently, as a result of the Acute Disease Quality Initiative (ADQI) 17th Conference on Continuous RRT, an individualized approach based on the demand–capacity balance was proposed.50 According to the consensus, acute RRT should be considered when metabolic and fluid demands exceed the patient’s total kidney capacity. This “watchful waiting” strategy requires a careful ongoing recognition of the clinical context (causes, the clinical course, the AKI trajectory, nonrenal organ dysfunction, the degree of fluid overload, chronic comorbidities, accommodation of nutritional and medication needs and other organ support therapies) by the experienced, optimally multidisciplinary, treatment team.
Recently, the idea of rapid response teams composed of different healthcare professionals (physicians, nurses, and paramedics) was conceived to bring ICU‑level skills such as the intensification of fluid resuscitation, an appropriate antimicrobial therapy in previously unrecognized septic shock, and care outside of the ICU.51 It also appears that this approach may not only reduce the incidence of AKI but also decrease in‑hospital and long‑term mortality. However, an increased workload of active team members has been the major concern about implementing this system in Polish hospitals.51
Key messages for everyday practice
The current approach to AKI includes: 1) identification and treatment of the underlying causes such as volume depletion, hypotension, use of selected drugs, or urinary tract obstruction; 2) removal of any potential insults to minimize additional injury; and 3) supportive measures to maintain optimal fluid, acid–base, and electrolyte balances. In patients with severe AKI, RRT is initiated when these measures fail to provide an adequate and safe control of homeostasis. A stepwise approach for the recognition and management of AKI is presented in Figure 2. The timing of dialysis initiation as well as its optimal dose remains controversial. It should be related to the general condition of the patient, capacity of the cardiovascular system and other organs, as well as observed or predicted dynamics of serum potassium and acid–base alterations. In recent years, a concept of the differentiated and individualized approach has been increasingly appreciated,50 according to which RRT should be considered when metabolic and fluid demands exceed the total kidney capacity.
The prognosis in hospital‑acquired AKI is generally poor and is associated with high in‑hospital and long‑term mortality. However, since AKI is not a single disease yet a complex, heterogeneous syndrome being a collection of entirely different entities, ranging from those relatively benign such as pre- and postrenal AKI to multiorgan failure, the prognosis widely varies among patients. In addition to the cause, the risk of poor outcomes is determined by a variety of clinical factors including patients’ age, underlying CKD, baseline renal function, failure of other organs, sepsis, chronic comorbidities, stage and length of an AKI episode, and the degree of renal recovery.
It is suggested that AKI survivors, especially those who develop AKI in the hospital, should be closely followed up, since they are at substantial risk of relapse and the subsequent development of end‑stage CKD as well as other adverse outcomes including hypertension and cardiovascular disease. According to the 2012 KDIGO guidelines, patients discharged from the hospital with a diagnosis of AKI should be evaluated within 90 days for resolution and new onset or worsening of pre‑existing CKD.17 However, data from multiple healthcare systems have indicated that, despite these recommendations, most patients who survive AKI do not see a nephrologist and many of them do not receive any follow‑up.52-54 Harel et al55 demonstrated that early postdischarge outpatient follow‑up with a nephrologist in patients after AKI requiring RRT was associated with a 24% reduction in mortality during 2 years. Whether postdischarge AKI care will confer a real net benefit needs to be addressed in large clinical trials. Recently, the experience of 2 clinical programs for the care of post‑AKI patients were presented: the Acute Kidney Injury Follow‑up Clinic for adults in Toronto and the AKI Survivor Clinic for children in Cincinnati.56 The authors planned a randomized controlled trial at multiple centers in Toronto to compare AKI Follow‑up Clinic interventions and standard care. The primary outcome of this ongoing trial (ClinicalTrials.gov identifier, NCT02483039) includes major adverse kidney events at 1 year following an AKI episode; the estimated study completion date is December 2022. As the population of AKI survivors is growing, the extension of care on all AKI survivors may be impossible. However, this population is very heterogeneous and it could be reasonable to stratify patients by the risk of AKI development to target those who would most likely benefit from various specific transitional strategies.
- Cerda J, Liu KD, Cruz DN, et al. Promoting kidney function recovery in patients with AKI requiring RRT. Clin J Am Soc Nephrol. 2015; 10: 1859‑1867. | Crossref
- Hsu RK, McCulloch CE, Dudley RA, et al. Temporal changes in incidence of dialysis‑requiring AKI. J Am Soc Nephrol. 2013; 24: 37‑42. | Crossref
- Hoste EAJ, Kellum JA, Selby NM, et al. Global epidemiology and outcomes of acute kidney injury. Nat Rev Nephrol. 2018; 14: 607‑625. | Crossref
- Noble RA, Lucas BJ, Selby NM. Long‑term outcomes in patients with acute kidney injury. Clin J Am Soc Nephrol. 2020; 15: 423‑429. | Crossref
- Uchino S, Kellum JA, Bellomo R, et al. Acute renal failure in critically ill patients: a multinational, multicenter study. JAMA. 2005; 294: 813‑818. | Crossref
ARTICLE INFORMATION