Uremic leontiasis ossea inducing respiratory failure in a patient with stage 5 chronic kidney disease



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Uremic leontiasis ossea inducing respiratory failure in a patient with stage 5 chronic kidney disease
Uremic leontiasis ossea (ULO) is one of the most severe complications of renal osteodystrophy (RO) caused by chronic kidney disease (CKD) and is characterized by cranial and facial bone thickening. Proper diagnosis and treatment are main factors to avoid severe esthetic and functional disorders.1,2
A 61‑year‑old man with CKD, on hemodialysis therapy for 6 years, was referred to our department because of respiratory failure.
The patient’s medical history revealed a 2‑month hemodialysis episode during his hospitalization in the Department of Gastrology and Hepatology due to hepatorenal syndrome, probably induced by alcoholic hepatitis. Two years later, the patient had an arteriovenous fistula created and started long‑term hemodialysis. In 2014, single‑photon emission computed tomography of the parathyroid glands, performed owing to high levels of total parathormone and phosphorus, revealed high radioisotope marker uptake in the left lower parathyroid gland. The patient did not agree for surgical or pharmacological treatment and, additionally, he very often omitted hemodialysis sessions.
On admission, he had pulmonary edema with saturation of 64%. Physical examination showed constrained head position and facial deformities, such as enlarged facial bones, malocclusion, deformed palate, splayed dentition, and narrowing of the pharynx. Blood test results showed high levels of total calcium (2.58 mmol/l), phosphorus (2.02 mmol/l), parathormone (1168 pg/ml), 25‑hydroxy vitamin D (4.47 ng/ml), and alkaline phosphatase (511 U/l). Chest X‑ray showed cephalization of the pulmonary vessels, peribronchial cuffing, increased heart size, and fluid in the right pleural space.
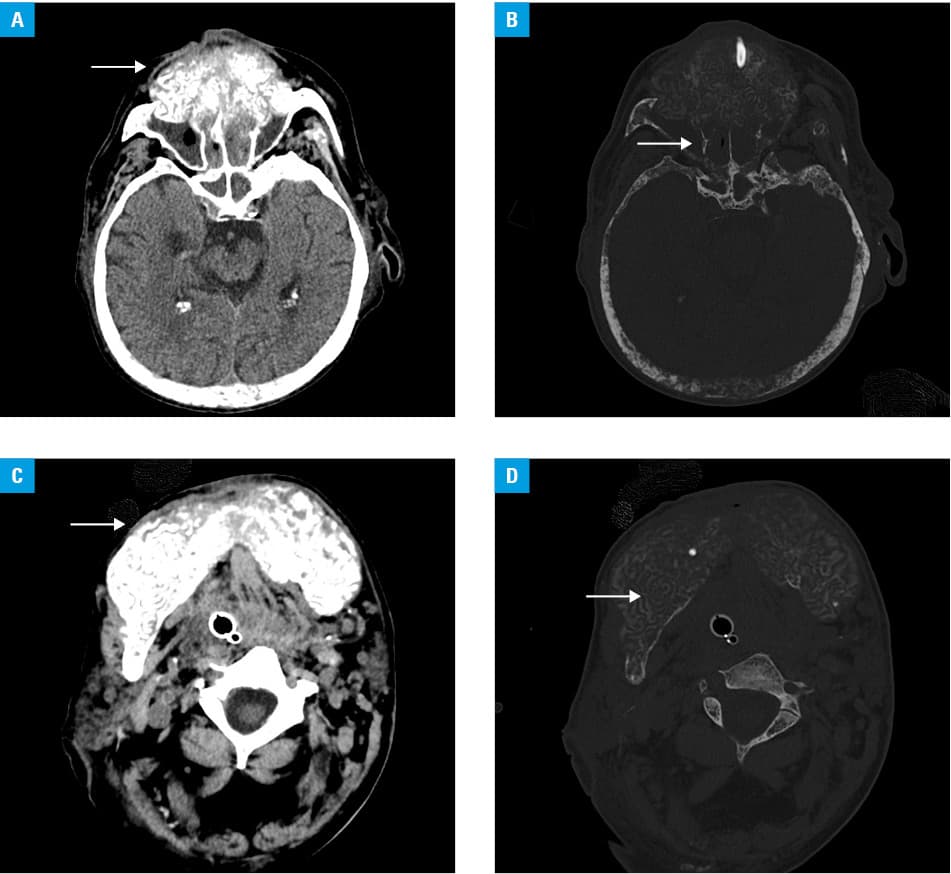
The patient underwent hemodialysis with ultrafiltration of 3500 ml and, because of progressive respiratory failure, he was intubated and transferred to the intensive care unit where sedation, mechanical ventilation, and continuous veno‑venous hemodialysis with ultrafiltration were used. A computed tomography scan of the head demonstrated hypertrophy of the maxilla and the mandible with almost complete obliteration of the maxillary sinuses (Figure 1A and 1B). Symmetric replacement of the osseous matrix of the mandible and the maxilla by expansile soft tissue was found, including tunneling of this soft tissue through the residual osseous matrix (Figure 1C and 1D), which corresponded with a form of RO—ULO. The patient received alfacalcidol at a dose of 1 μg/d, and calcium and phosphorus levels were balanced by total parenteral nutrition.
Because of the changes of the facial skeleton, tracheotomy had to be performed to enable respiration. Finally, when the patient did not require ventilation therapy anymore, he was transferred to the Department of Nephrology. During the hospitalization, the patient could not speak and eat because of RO changes, thus percutaneous endoscopic gastrostomy was performed. Additionally, he underwent intermittent hemodialysis. However, progressive pneumonia and cachexia led to cardiac arrest and the patient died after 16 days of treatment.
Differential diagnosis of ULO should include fibrous dysplasia, cherubism, giant cell tumor, Paget disease, gigantism, hyperparathyroidism, and RO.
According to the available data, leontiasis ossea is a very rare manifestation of widening of the interdental spaces, flattening of the nares and nasal bridge, and jaw enlargement. Soft tissue tunneling through the residual osseous matrix remains a key imaging finding.3
Early treatment of secondary hyperparathyroidism, regular hemodialysis therapy,4 and maxillofacial surgery may be the proper treatment strategy in patients with ULO.
- Donoso‑Hofer F, Gunther‑Wood M, Romero‑Romano P, et al. Uremic leontiasis ossea, a rare presentation of severe renal osteodystrophy secondary to hyperparathyroidism. J Stomatol Oral Maxillofac Surg. 2018; 119: 56‑60. | Crossref
- Luchi WM, Vianna JG, Roberto LE, et al. Uremic leontiasis ossea. Endocrine. 2019; 65: 707‑709. | Crossref
- Haroyan H, Bos A, Ginat DT. Uremic leontiasis ossea. Am J of Otolaryngology. 2015; 36: 74‑76. | Crossref
- .Gołasa P, Chowaniec E, Krzanowski M, et al. Cast‑like calcification in the superior vena cava in a young woman with lupus nephritis on hemodialysis. Pol Arch Intern Med. 2019; 129: 712‑713.
ARTICLE INFORMATION