In Poland, cholelithiasis occurs in approximately 7.5 million people, 4‑fold more often in women than men.1 The incidence increases with age and it affects 18% of population up to 40 years old and even 50% of people aged over 60 years.2
In 80% of affected people, the course of the disease is asymptomatic. Larger deposits may block the outflow of bile usually resulting in the appearance of clinical symptoms including biliary colic, in which pain on palpation is found in the right subcostal area.2 A positive Chelmonski and/or Murphy sign is typical. Paravertebral pains or prerenal azotemia occur very rarely. Additional symptoms include nausea, vomiting, heartburn, and stomach bloating.3
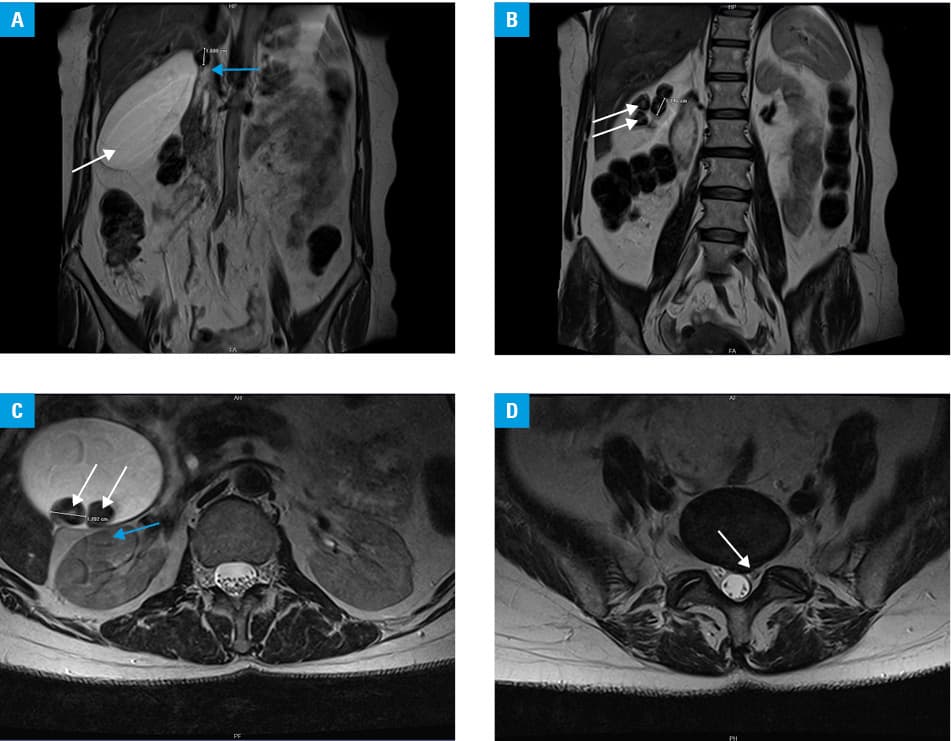
A 54‑year‑old woman reported to the general practitioner because of the right‑sided abdominal pain radiating to the right iliac fossa as well as periodically occurring numbness and tingling in the right lower limb. Due to aforementioned symptoms, she was referred to the neurology department, where magnetic resonance (MR) imaging of the lumbar spine was performed. Based on MR, an incidental central‑to‑left–sided disc bulging at the L5‑S1 level with compression of the left spinal nerve was diagnosed, which was irrelevant in terms of the patient’s complaints. In addition, MR revealed an enlarged gallbladder (hydrops) measuring 140 × 70 × 50 mm with the presence of deposits of up to 17 mm, one of which blocked the neck significantly impeding outflow of the bile (Figure 1A–1D). As the immediate abdominal ultrasound confirmed the diagnosis, the patient was referred for cholecystectomy.
Palpation and detailed history‑taking lie at the basis of differential diagnosis of abdominal pain. Positive Chelmonski sign indicates cholelithiasis or cholecystitis, and ultrasound is the leading imaging modality in search of the underlying cause of abdominal pain. In case of our patient, both procedures were omitted. Diagnostic effectiveness of ultrasound in cholelithiasis exceeds 95%. The image is very characteristic, showing clearly solid hyperechoic structures that change location due to body movements.4,5 In addition, an acoustic shadow is visible behind the deposit, as it reflects the whole or almost whole ultrasonic wave. Symptoms of cholelithiasis might be equivocal and can be easily misinterpreted as other pathologies without proper clinical evaluation including physical examination and palpation of the abdomen. Epigastric pain, being the most representative symptom of cholelithiasis, may also be caused by: recent myocardial infarction, abdominal aortic dissection, pleuritis, pericarditis, gastric and duodenal ulcers, pancreatitis, acute appendicitis.2,5 Lumbar discopathy and degenerative spine disease are considered the most frequent causes of back pain, especially when radiating to the lower limbs. Our patient reported abdominal pain radiating to the right iliac fossa as well as numbness and tingling of the right lower limb, which primarily suggested sciatic neuritis. Because of that, she was referred to neurology department and underwent MR at once, and the basic method of abdominal examination was omitted. The presented case of the 54‑year‑old woman emphasizes how nonspecific and misleading the symptoms of cholecystolithiasis may be, initially mimicking an entirely different entity. Ultrasound together with thorough physical examination allow for nearly unequivocal recognition of clinically apparent gallbladder deposits.
- Idowu BM, Onigbinde SO, Ebie IU, Adeyemi MT. Gallbladder diseases in pregnancy: sonographic findings in an indigenous African population. J Ultrason. 2019; 19: 269‑275. | Crossref
- Greenberger NJ, Paumgartner G. Diseases of the gallbladder and bile ducts. In: Jameson J, Fauci AS, Kasper DL, et al, eds. Harrison’s Principles of Internal Medicine, 20th ed. New York, NY: McGraw‑Hill; 2018: 2422‑2432.
- Hassan K, Khakhiashvili A, Awawdeh M, et al. Unusual presentation of gallstones. Rom J Gastroenterol. 2005; 14: 173‑175.
- Walas MK, Skoczylas K, Gierbliński I. Standards of the Polish Ultrasound Society – update. The liver, gallbladder and bile ducts examinations. J Ultrason. 2012; 12: 428‑445. | Crossref
- Murphy MC, Gibney B, Gillespie C, et al. Gallstones top to toe: what the radiologist needs to know. Insights Imaging. 2020; 11: 13. | Crossref
ARTICLE INFORMATION