Sex differences in the frequency of gastrointestinal symptoms and olfactory or taste disorders in 1942 nonhospitalized patients with coronavirus disease 2019 (COVID-19)
Key words: coronavirus disease 2019, gastrointestinal symptoms, severe acute respiratory syndrome coronavirus 2, smell, taste



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Sex differences in the frequency of gastrointestinal symptoms and olfactory or taste disorders in 1942 nonhospitalized patients with coronavirus disease 2019 (COVID-19)
Introduction: The coronavirus disease 2019 (COVID‑19) is a communicable disease caused by a novel coronavirus.
Objectives: This study aimed to assess self‑reported frequency of gastrointestinal symptoms and olfactory or taste disorders in nonhospitalized patients with COVID‑19 in Poland.
Patients and methods: This cross‑sectional survey was conducted between April 17 and 18, 2020, in 4516 nonhospitalized patients with COVID‑19 in Poland. The questionnaire included 8 questions related to the health status, symptoms of COVID‑19, comorbidities, and smoking status.
Results: Completed questionnaires were obtained from 1942 patients with COVID‑19 with a response rate of 43%. The median age of the respondents was 50 years; 60.2% were women. Among nonhospitalized patients with COVID‑19, 21.3% had hypertension, 4.5% had diabetes, and 3.1% had a chronic respiratory disease. Regular tobacco use was declared by 11.2% of patients with COVID‑19. At least one gastrointestinal symptom was reported by 53.6% of patients. Almost half of patients (47%) with COVID‑19 reported lack of appetite and 24.2% reported diarrhea. Among 1942 interviewed patients, 54.2% reported at least 1 olfactory or taste disorder and 42.5% reported both alterations. Self‑reported olfactory and taste disorders were 49.2% and 47.5%, respectively. Self‑reported frequency of gastrointestinal symptoms and olfactory or taste disorders during COVID‑19 was significantly higher (P <0.001) in women than men.
Conclusions: This study demonstrated that olfactory and taste disorders are frequent symptoms in patients with mild‑to‑moderate COVID‑19. Moreover, our study indicated sex differences in the frequency of gastrointestinal symptoms and olfactory or taste disorders among nonhospitalized patients with COVID‑19.
What's new?
This study used data from a cross‑sectional survey to assess the self‑reported prevalence of gastrointestinal symptoms and olfactory or taste disorders in 1942 nonhospitalized patients with coronavirus disease 2019 (COVID‑19) in Poland. The sample size was relatively large, compared with other available studies. Our findings indicate that more than half of patients with mild COVID‑19 reported gastrointestinal (53.6%) or neurological (olfactory or taste disorders; 54.2%) symptoms. The present findings also indicate that self‑reported frequency of gastrointestinal symptoms and olfactory or taste disorders during the COVID‑19 course was significantly higher in women than in men. This finding suggests that gastrointestinal symptoms and olfactory or taste disorders should be considered as potential clinical manifestations of COVID‑19 in patients with mild to moderate symptoms.
Introduction
Coronavirus disease 2019 (COVID‑19) is a communicable disease caused by severe acute respiratory syndrome coronavirus 2 (SARS‑CoV‑2).1,2 To confirm the diagnosis of COVID‑19, it is required to detect SARS‑CoV‑2 RNA by reverse transcription–polymerase chain reaction (RT‑PCR).3 Most COVID‑19 cases (approximately 80%) manifest only mild to moderate symptoms while in 14% of cases, symptoms are severe (dyspnea, hypoxia, or >50% lung involvement on imaging) and only 5% of COVID‑19 cases are critical (respiratory failure, shock, or multiorgan system dysfunction).2,4,5 Older age and comorbidities such as cardiovascular disease, diabetes, chronic respiratory disease, hypertension, and cancer are risk factors for a severe course of illness, complications, and death from COVID‑19.6,7
The most common COVID‑19 symptoms are fever (83%–99%), cough (59%–82%), and fatigue (44%–70%). Less common reported symptoms include shortness of breath (31%–40%), expectoration of sputum (28%–33%), muscle and joint pain (11%–35%), headaches (10%–15%), rhinitis and sore throat (14%–15%), hemoptysis (<10%), nausea or vomiting (5.8%), and diarrhea (3.8%–4.2%).2,5,8-10 Moreover, it is suggested that the clinical presentation of COVID‑19 may include gastrointestinal symptoms and olfactory or gustatory dysfunctions.11-15 However, data on the frequency of gastrointestinal and neurological manifestation of nonhospitalized patients with mild or asymptomatic COVID‑19 have not been sufficiently documented.
This study aimed to assess self‑reported frequency of gastrointestinal symptoms and olfactory or taste disorders in nonhospitalized patients with COVID‑19 in Poland.
Patients and methods
Study design and population
This cross‑sectional survey was carried out between April 17 and 18, 2020, among 4516 nonhospitalized patients with COVID‑19 in Poland. In Poland, all mild and moderate cases of COVID‑19 may be referred to as institution‑based isolation or home‑based isolation, depending on the physician’s decision. All COVID‑19 cases in home‑based isolation were eligible to be included in the research. As of April 17, 2020, a total of 8379 laboratory‑confirmed COVID‑19 cases were reported in Poland (including severe and fatal cases). The laboratory diagnosis of COVID‑19 was based on the detection of SARS‑CoV‑2 RNA in throat or nasal swabs samples by RT‑PCR. Laboratory testing for COVID‑19 followed the European Centre for Disease Prevention and Control guidelines.3
Detailed contact information for adults of Polish nationality was available for 4516 cases. All patients with COVID‑19 in home‑based isolation were called by phone as part of sanitary and epidemiological supervision. Participation in the study was voluntary. Participants had the right to refuse to participate without giving a reason. The data was encoded anonymously, making it impossible to identify individuals. All procedures followed the ethical standards of the national research committee and the 1964 Helsinki Declaration (and its later amendments).
Study questionnaire
The questionnaire included 8 questions related to the health status, symptoms of COVID‑19, comorbidities, and smoking status. Questions also addressed attitudes toward the potential SARS‑CoV‑2 vaccine.
Self‑reported presence of symptoms of COVID‑19 was based on a positive response to the following: “During your illness, did you have any of the following symptoms: (1) lack of appetite, (2) diarrhea, (3) olfactory disorder, (4) taste disorder?” The presence of comorbidities was based on a positive response to the following: “Do you have any of the following: (1) hypertension, (2) cardiovascular disease, (3) diabetes, (4) chronic respiratory disease, (5) chronic kidney disease?”
Smoking status was based on a positive response to the following: “Do you currently smoke?” Attitude toward potential SARS‑CoV‑2 vaccine was based on the question: “If a SARS‑CoV‑2 coronavirus vaccine becomes available, will you choose to get vaccinated?” (Yes / No).
One of the main goals of the study was to obtain a high response rate. Therefore, the number of questions was limited to those having practical implications for mitigating the early spread of the SARS‑CoV‑2 epidemic in Poland.
Statistical analysis
Data analysis was performed using the procedures available in the Statistica 13 package (TIBCO Software Inc., Palo Alto, California, United States). The distribution of categorical variables was shown by frequencies and proportions along with 95% CI. Categorical variables were compared with the independent samples χ2 test. Statistical significance was based on a P value of less than 0.05.
Results
Completed questionnaires were obtained from 1942 patients with COVID‑19 with a response rate of 43% (41.8% among men and 43.8% among women). The median age of the respondents was 50 years. The group included more women (60.2%) than men (39.8%). Among nonhospitalized patients with COVID‑19, 21.3% had hypertension, 4.5% had diabetes, and 3.1% had a chronic respiratory disease (Table 1). Regular tobacco use was declared by 11.2% of patients with COVID‑19.
Parameter | Overall (n = 1942) | |
Data are presented as number (percentage) unless otherwise indicated. | ||
Age, y, median | 50 | |
Sex | Female | 1169 (60.2) |
Male | 773 (39.8) | |
Comorbidities | ||
Hypertension | 413 (21.3) | |
Cardiovascular disease | 116 (6) | |
Diabetes | 88 (4.5) | |
Chronic respiratory disease | 60 (3.1) | |
Chronic kidney disease | 29 (1.5) | |
Current smokers (n = 1087) | Yes | 122 (11.2) |
No | 965 (88.8) | |
If a coronavirus vaccine becomes available, 72.7% of nonhospitalized patients with COVID‑19 declared willingness to get vaccinated against SARS‑CoV‑2 coronavirus (70.5% among women and 76.6% among men; P = 0.03).
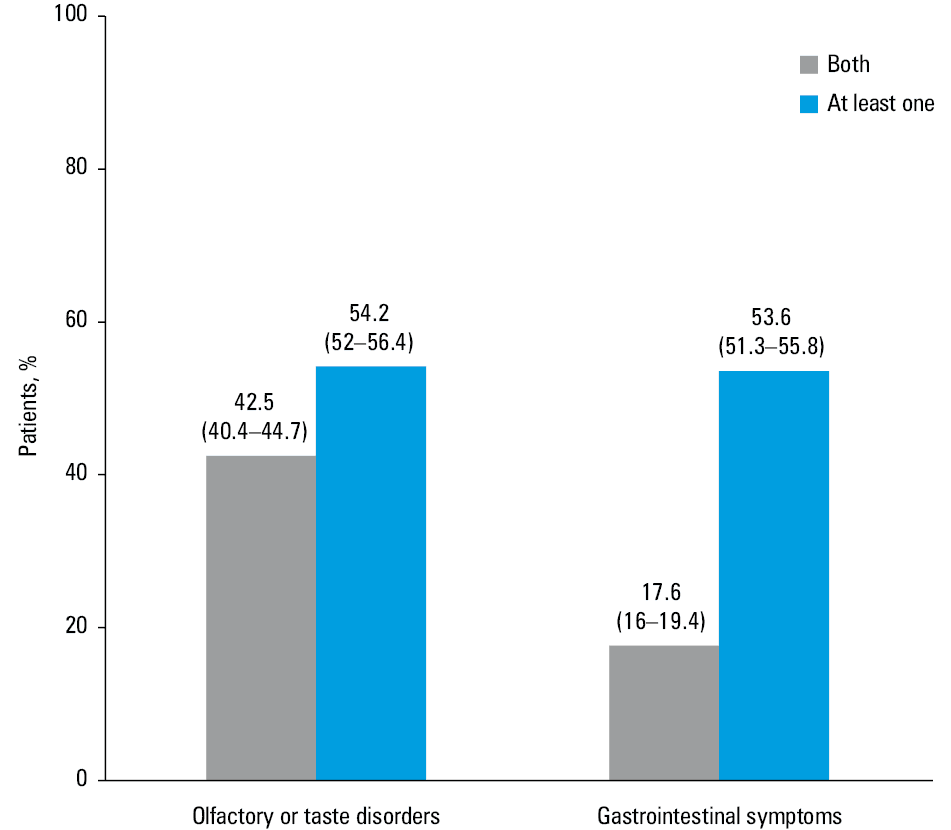
At least one gastrointestinal symptom was reported by 53.6% of patients (Figure 1). Both gastrointestinal symptoms (lack of appetite and diarrhea) were reported by 17.6% of patients with COVID‑19. Almost half of patients (47%) with mild symptoms of COVID‑19 reported lack of appetite and 24.2% reported diarrhea during COVID‑19 course. Among 1942 interviewed patients, 54.2% reported at least 1 olfactory or taste disorder and 42.5% reported both alterations. Self‑reported olfactory and taste disorders were 49.2% and 47.5%, respectively. No gastrointestinal symptoms and olfactory or taste disorders were reported by 31.6% of patients.
There were sex differences in the frequency of gastrointestinal symptoms and olfactory or taste disorders among nonhospitalized patients with COVID‑19 (Table 2). Self‑reported frequency of gastrointestinal symptoms and olfactory or taste disorders during COVID‑19 course was significantly higher among women than men (P <0.001). Details are presented in Table 2.
Symptom | Overall (n = 1942) | Women (n = 1169) | Men (n = 773) | P value | |||
n (%) | 95 CI | n (%) | 95 CI | n (%) | 95 CI | ||
Lack of appetite | 912 (47) | 44.8–49.2 | 637 (54.5) | 51.6–57.3 | 275 (35.6) | 32.3–39 | <0.001 |
Diarrhea | 470 (24.2) | 22.4–26.2 | 311 (26.6) | 24.2–29.2 | 159 (20.6) | 17.9–23.6 | 0.002 |
Olfactory disorder | 956 (49.2) | 47–51.5 | 636 (54.4) | 51.5–57.2 | 320 (41.4) | 38–44.9 | <0.001 |
Taste disorder | 923 (47.5) | 45.3–49.8 | 617 (52.8) | 49.9–55.6 | 306 (39.6) | 36.2–43.1 | <0.001 |
Discussion
This study used data from a cross‑sectional survey to assess the self‑reported frequency of gastrointestinal symptoms and olfactory or taste disorders in 1942 nonhospitalized patients with COVID‑19 in Poland. Our findings indicate that more than half of patients with mild COVID‑19 course reported gastrointestinal symptoms (53.6%) or neurological manifestations (olfactory or taste disorders) (54.2%) of COVID‑19. The present findings also point to sex differences in the frequency of gastrointestinal symptoms and olfactory or taste disorders among nonhospitalized patients with COVID‑19. Self‑reported frequency of gastrointestinal symptoms and olfactory or taste disorders during the course of COVID‑19 was significantly higher among women than men. This finding suggests that gastrointestinal symptoms and olfactory or taste disorders should be considered as potential clinical manifestations of COVID‑19 among patients with mild to moderate symptoms.
We observed a higher proportion of COVID‑19 among women than men. The frequency of smoking (11.2%) among nonhospitalized patients with COVID‑19 was lower compared with the general population (21%).16 However, this study includes only nonhospitalized patients with a mild course of COVID‑19.
The majority of currently available data on gastrointestinal symptoms in COVID‑19 was derived from hospitalized patients. Among 138 hospitalized patients with COVID‑19 in Wuhan, China, 39.9% reported anorexia / lack of appetite and 10.1% had diarrhea.9 Another study carried out among 651 patients in China, showed that 11.4% of hospitalized patients presented with at least 1 gastrointestinal symptom.12 A multicenter cohort study across 9 hospitals in the United States showed that 61.3% patients reported at least 1 gastrointestinal symptom, wherein 34.8% of patients reported anorexia and 33.7% reported diarrhea.11 To the best of our knowledge, this study is one of the few studies conducted in nonhospitalized patients with COVID‑19. Our findings indicate that more than half of nonhospitalized patients with COVID‑19 (53.6%) reported at least 1 gastrointestinal symptom, wherein 47% reported lack of appetite and 24.2%, diarrhea. The frequency of gastrointestinal symptoms in our study is higher than in studies from China but comparable to those observed in the United States.
Moreover, it is suggested that a significant proportion of patients with COVID‑19 may report olfactory or gustatory dysfunctions.13-15 In a multicenter PCR‑based case‑control study in Spain, out of 79 patients enrolled, 35.4% reported a smell disorder and 31.6% reported a taste disorder.17 A study carried out in Wuhan, China in 214 patients with COVID‑19 showed that 5.6% of those reported taste impairment and 5.1%, smell impairment.15 A higher frequency of olfactory and gustatory dysfunctions was observed in a multicenter European study by Lechien et al.13 Among 417 patients with mild‑to‑moderate COVID‑19, olfactory dysfunction was reported by 85.6% of patients and gustatory dysfunctions by 88%.13 In our study, 49.2% of patients reported an olfactory disorder and 47.5% reported a taste disorder. Our findings are in line with the study by Lechien et al13 and indicate that olfactory and taste disorders are frequent symptoms in European patients with COVID‑19.
Our findings indicate that the frequency of gastrointestinal symptoms and olfactory or taste disorders during COVID‑19 is higher among women than men. This phenomenon may be explained by the sex differences in human olfaction.18 Oliveira‑Pinto et al18 showed that women have more neurons and gial cells in the olfactory bulbs than males. Moreover, the impact of hormonal modulation on the gustatory system should be considered.19 Further studies may be required to address nonrespiratory symptoms among patients with COVID‑19 and sex differences in the frequency of gastrointestinal symptoms and olfactory or taste disorders in COVID‑19.
This study has several limitations. The presence of symptoms of COVID‑19 was self‑reported and was not confirmed by a physician. Secondly, the list of COVID‑19 symptoms was limited to 4 key questions. However, most of the currently available studies on COVID‑19 are based on electronic health records of patients with COVID‑19. Third, this study was carried out among nonhospitalized patients so the results cannot be generalized to the whole population of patients with COVID‑19. We cannot exclude selection bias. Nevertheless, our study is one of the first cross‑sectional surveys focusing on nonrespiratory symptoms of COVID‑19. Moreover, the sample size is relatively high compared with other currently published studies.
In conclusion, this study demonstrated that olfactory and taste disorders are frequent symptoms in patients with mild‑to‑moderate COVID‑19. Moreover, our study indicates sex differences in the frequency of gastrointestinal symptoms and olfactory or taste disorders among nonhospitalized patients with COVID‑19. This study suggests that nonrespiratory symptoms should be considered as potential clinical manifestations of COVID‑19 during the diagnostic workup.
- Lu R, Zhao X, Li J, et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: implications for virus origins and receptor binding. Lancet. 2020; 395: 565‑574.
- Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020; 395: 497‑506. | Crossref
- European Centre for Disease Prevention and Control (ECDC). Case definition and European surveillance for COVID‑19, as of 2 March 2020. https://www.ecdc.europa.eu/en/case‑definition‑and‑european‑surveillance‑human‑infection‑novel‑coronavirus‑2019‑ncov. Accessed April 28, 2020.
- Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID‑19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020 Feb 24. [Epub ahead of print]. | Crossref
- Guan WJ, Ni ZY, Hu Y, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020; 382: 1708‑1720.
ARTICLE INFORMATION