Usefulness of the 2MACE score as a predictor of long-term all-cause mortality in patients with atrial fibrillation
Key words: atrial fibrillation, mortality, score



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Usefulness of the 2MACE score as a predictor of long-term all-cause mortality in patients with atrial fibrillation
Introduction: 2MACE is a risk assessment score designed to stratify cardiovascular risk in patients with atrial fibrillation (AF). Early detection of increased cardiovascular risk is of vital importance in this population, as it helps reduce mortality and morbidity rates.
Objectives: This study aimed to assess the utility of the 2MACE score in predicting long‑term mortality in patients with AF.
Patients and methods: This was a post hoc analysis of a prospective observational cohort study including consecutive patients with nonvalvular AF, who were followed for a median duration of 81 months.
Results: The final analysis included 1351 patients (men, 53.1%; median [interquartile range] age, 71 [62–80] years). During the follow‑up, 142 patients (10.5%) died. Deceased patients were more often classified as high risk according to the 2MACE score than survivors (80.3% vs 53.2%; P <0.0001). The receiver operator characteristic curve analysis demonstrated that the 2MACE score had a good predictive value for long‑term all‑cause mortality (area under the curve, 0.73; 95% CI, 0.69–0.78). The mortality rate was significantly increased in patients with a 2MACE score of 3 or higher (hazard ratio, 3.40; 95% CI, 2.33–5.49).
Conclusions: The 2MACE score is a good predictor of long‑term all‑cause mortality in patients with AF. A progressive increase in the mortality rate was observed with an increasing 2MACE score.
What's new?
This is the first study using the 2MACE score to assess long‑term all‑cause mortality in a real‑world cohort of consecutive patients with nonvalvular atrial fibrillation. In this post hoc analysis of a prospective observational study, more than 50% of patients were classified as having high cardiovascular risk. The 2MACE score was shown to be a good predictor of long‑term all‑cause mortality. Moreover, the mortality rate increased with an increase in the 2MACE score.
Introduction
Cardiovascular risk reduction is one of the pivotal issues in the management of patients with atrial fibrillation (AF). Arrhythmia‑related thromboembolic risk, including the risk of stroke and peripheral thromboembolism, remains a significant concern in this population.1 Most current guidelines and risk prediction scores focus on thromboembolic risk stratification. Nevertheless, studies show that the occurrence, progression, and outcomes of AF are strongly associated with cardiovascular risk factors and that AF itself may contribute to the development of other cardiovascular diseases possibly affecting mortality.2,3 Therefore, early detection of increased cardiovascular risk might be highly beneficial in this group of patients.
In 2016, Pastori et al4 developed a risk score for predicting major adverse cardiovascular events in patients with AF. The 2MACE score includes metabolic syndrome, age of 75 years or older, myocardial infarction or revascularization, congestive heart failure (HF), and thromboembolism.4 Several subsequent studies confirmed the usefulness of the score for the prediction of major cardiovascular events and mortality.5-7 The current study aimed to investigate the utility of the 2MACE score for predicting long‑term all‑cause mortality in patients with nonvalvular AF.
Methods
This post hoc analysis of a prospective observational cohort study included consecutive patients with nonvalvular AF. We identified patients diagnosed with AF between January 1, 2010, and December 31, 2019. Atrial fibrillation and concomitant diseases were diagnosed de novo according to the current guidelines or were identified based on medical records.1,2 Before enrollment, all patients provided written informed consent for participation in the study. Inclusion criteria were the previous diagnosis of nonvalvular AF, age of 18 years or older, and written informed consent to be included in the study. Patients without sufficient medical records to calculate the baseline risk score or those who did not provide informed consent were excluded. The study was approved by the local Ethics Committee, and its protocol conformed to the ethical guidelines of the 2013 Declaration of Helsinki. All patients were followed for all‑cause mortality for up to 120 months. The final date of the follow‑up was January 31, 2020. In our study, death was treated as one of the censoring events. Data on mortality were obtained from hospital and outpatient records as well as from the PESEL register (Common Electronic System of Population Register in Poland), which contains the date of death.
On enrollment, all patients had their medical history reviewed and underwent screening for cardiovascular risk factors. Based on the obtained information, the 2MACE and CHA2DS2-VASc scores were calculated.4,8,9 The definitions used for score calculations were taken from respective validation studies.4,8,9 Concomitant diseases were diagnosed according to the current guidelines. Arterial hypertension was defined as repeatedly elevated blood pressure (>140/90 mm Hg measured as described in the guidelines) or the use of antihypertensive drugs. Diabetes was defined as casual plasma glucose levels higher than 200 mg/dl (11.1 mmol/l) or fasting plasma glucose levels higher than 126 mg/dl (7 mmol/l) or 2‑hour plasma glucose levels higher than 200 mg/dl (11.1 mmol/l) during an oral glucose tolerance test or as the use of antidiabetic drugs. Heart failure was defined as the presence of signs and symptoms typical of HF or as reduced ejection fraction (<40%). Chronic kidney disease was defined as an estimated glomerular filtration rate of less than 60 ml/min/1.73 m2 or the presence of albuminuria.
In the 2MACE score, 2 points were assigned for metabolic syndrome (diagnosed according to the modified National Cholesterol Education Program Expert Panel and Adult Treatment Panel III criteria)10 and age of 75 years or older, while 1 point was assigned for a history of stroke or transient ischemic attack, a history of myocardial infarction or revascularization, congestive HF (left ventricular ejection fraction ≤40%), and a history of thromboembolism.4 Elevated cardiovascular risk was diagnosed when a patient scored 3 points or higher.
In the CHA2DS2-VASc score, 2 points were assigned for an age of 75 years or older and a history of stroke, transient ischemic attack, or thromboembolism. One point was given for HF (defined as moderate to severe systolic left ventricular dysfunction, left ventricular ejection fraction of 40% or lower, or recent decompensated HF requiring hospitalization), hypertension, diabetes mellitus, vascular disease (defined as a history of myocardial infarction, complex aortic plaque, or peripheral artery disease), age 65 to 74 years, and female sex.9
Statistical analysis
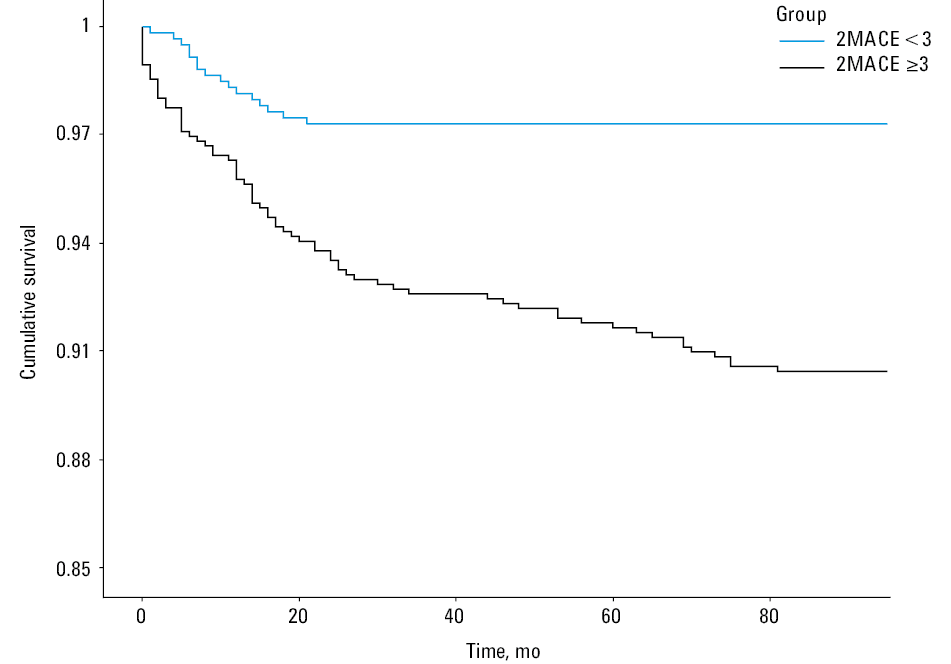
Data were tested for normality using the Kolmogorov–Smirnov test. Continuous variables were presented as mean (SD) and median (interquartile range [IQR]), if not normally distributed. Data were compared using the Mann–Whitney test or t test. Categorical variables were compared using the χ2 or Fisher exact test. Cox proportional hazard regression models were used to assess the association between the 2MACE score and all‑cause mortality. The survival analysis was performed using the Kaplan–Meier estimation to assess survival in patients with a 2MACE score of 3 points or higher in comparison with the remaining study population. The predictive value of the scores was assessed using the area under the receiver operator characteristic (ROC) curve analysis. A P value of less than 0.05 was considered significant. All statistical analyses were performed using SPSS version 26 for macOS (SPSS, Inc., Chicago, Illinois, United States).
Results
We enrolled 1437 patients, of whom 86 were lost to follow‑up. The final sample size included 1351 patients (men, 53.1%; median [IQR] age, 71 [62–80] years). Arterial hypertension was reported in 75.1% of patients, and a history of myocardial infarction, in 41.8%. Paroxysmal AF was present in 51.7% of cases. Patients were followed for a median (IQR) duration of 81 (71–85) months. During the follow‑up, 142 patients (10.5%) died. Deceased patients were older (mean [SD], 81.5 [10.2] years vs 69 [12.3] years; P <0.001) and more often had a history of myocardial infarction (P <0.001), hypertension (P <0.001), diabetes mellitus (P = 0.02), chronic kidney disease (P <0.001), HF (P <0.001), and dyslipidemia (P = 0.01), as compared with survivors. Patients who died were also more often classified as high risk according to the 2MACE score (80.3% vs 53.2%; P <0.001). Details are shown in Table 1.
Parameter | All patients (n =1351) | Survivors (n = 1209) | Deceased patients (n = 142) | P valuea |
Data are presented as number (percentage) of patients unless otherwise indicated.
a Survivors vs deceased patients
Abbreviations: ACEI, angiotensin‑converting enzyme inhibitor; ARB, angiotensin receptor blocker; IQR, interquartile range | ||||
Male sex | 718 (53.1) | 648 (53.6) | 70 (49.3) | 0.37 |
Age, y, median (IQR) | 71 (62–80) | 70 (61–79) | 84 (77–88) | <0.001 |
Body mass index, kg/m2, median (IQR) | 28 (25–31.1) | 28 (25.1–31.2) | 27.3 (23–30) | 0.03 |
Coronary artery disease | 565 (41.8) | 478 (39.5) | 87 (61.3) | <0.001 |
Myocardial infarction | 111 (8.2) | 87 (7.2) | 24 (16.9) | <0.001 |
Stroke | 188 (13.9) | 166 (13.7) | 22 (15.5) | 0.61 |
Arterial hypertension | 1014 (75.1) | 890 (73.6) | 124 (87.3) | <0.001 |
Diabetes mellitus | 333 (24.6) | 286 (23.7) | 47 (33.1) | 0.02 |
Thyroid disease | 171 (12.7) | 155 (12.8) | 16 (11.3) | 0.69 |
Chronic kidney disease | 263 (19.5) | 212 (17.5) | 51 (35.9) | <0.001 |
Chronic obstructive pulmonary disease | 122 (9) | 114 (9.4) | 8 (5.6) | 0.16 |
Heart failure | 703 (52) | 605 (50) | 98 (69) | <0.001 |
Dyslipidemia | 266 (19.7) | 250 (20.7) | 16 (11.3) | 0.01 |
Metabolic syndrome | 681 (50.4) | 649 (53.7) | 32 (22.5) | <0.001 |
Paroxysmal atrial fibrillation | 699 (51.7) | 633 (52.4) | 66 (46.5) | 0.21 |
Persistent atrial fibrillation | 328 (24.3) | 298 (26.4) | 30 (21.1) | 0.41 |
Permanent atrial fibrillation | 324 (24) | 278 (23) | 46 (32.4) | 0.02 |
2MACE score ≥3 | 757 (56) | 643 (53.2) | 114 (80.3) | <0.001 |
2MACE score, median (IQR) | 3 (2–4) | 3 (2–3) | 4 (3–5) | <0.0001 |
CHA2DS2-VASc score, median (IQR) | 4 (2–5) | 3 (2–5) | 5 (4–6) | <0.001 |
Treatment | ||||
Oral anticoagulants | 1109 (82.1) | 987 (81.6) | 122 (85.9) | 0.25 |
Antiplatelets | 280 (20.7) | 245 (20.3) | 35 (24.6) | 0.23 |
ACEIs or ARBs | 830 (61.4) | 742 (61.4) | 88 (62) | 0.93 |
Statins | 644 (47.7) | 583 (48.2) | 61 (43) | 0.25 |
Cause‑specific mortality | ||||
All‑cause mortality | 142 (10.5) | – | 142 (100) | – |
Cardiovascular mortality | 78 (5.8) | – | 78 (54.9) | – |
Cancer‑related mortality | 39 (2.9) | – | 39 (27.5) | – |
Other | 25 (1.9) | – | 25 (17.6) | – |
The median values of the risk scores calculated at baseline were as follows: 3 (IQR, 2–4) for 2MACE and 4 (IQR, 2–5) for CHA2DS2-VASc. A total of 757 patients (56%) were classified as the high‑risk group (≥3 points) according to the 2MACE score. Patients with a 2MACE score of 3 or higher, classified as having high cardiovascular risk, had a higher prevalence of all factors included in the score as well as a higher prevalence of thyroid disease (P = 0.02), chronic kidney disease (P <0.001), and dyslipidemia (P <0.001), as compared with the remaining patients. The comparison of survival between patients with a 2MACE score of 3 or higher and the remaining population is shown in Figure 1.
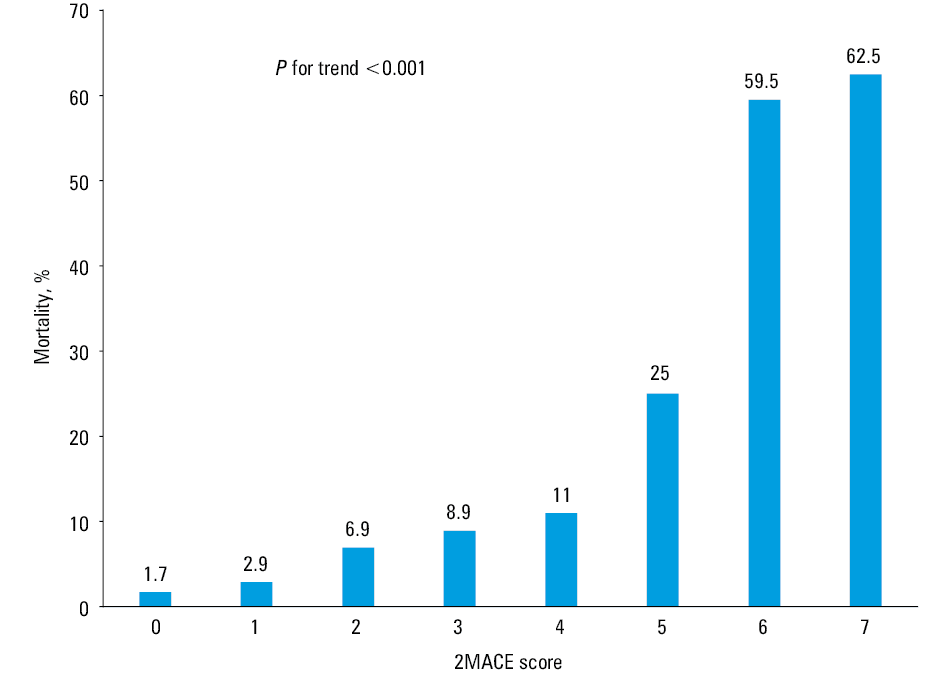
Long‑term all‑cause mortality rates significantly increased with an increasing 2MACE score (Figure 2). Data on the cause‑specific mortality are shown in Table 1.
The ROC curve analysis demonstrated that the 2MACE score had a good predictive value for all‑cause mortality in patients with AF (area under the curve, 0.73; 95% CI, 0.69–0.78). The comparison of the ROC curves showed that the CHA2DS2-VASc score was not inferior to the 2MACE score in the prediction of all‑cause mortality in this cohort (P = 0.8). All‑cause mortality was increased for patients with a 2MACE score of 3 or higher (hazard ratio, 3.4; 95% CI, 2.33–5.49). Our analysis showed that the 2MACE score was more likely to predict mortality than the CHA2DS2-VASc score (odds ratio [OR], 1.65; 95% CI, 1.41–1.93 vs OR, 1.22; 95% CI, 1.08–1.38).
Discussion
The present study is one of the few real‑world studies to assess all‑cause mortality in AF patients according to the 2MACE score. It showed that AF patients with elevated cardiovascular risk assessed with the 2MACE score have a higher risk of all‑cause mortality, as compared with the remaining AF population (15.1% vs 4.7%; P <0.001).
Several studies have shown that patients with AF are at increased risk of mortality and cardiovascular morbidity.11-13 This is in line with our research, which revealed a mortality rate of 10.5% during the follow‑up.
Currently, there are no risk scores for the assessment of mortality specifically in patients with AF. Risk assessment in this population is based on the evaluation of thromboembolic risk (CHADS2, CHA2DS2-VASc),8,9 bleeding risk (HAS‑BLED),14 composite clinical outcomes (TIMI‑AF),15 the effectiveness of antithrombotic therapy (SAMe‑TT2R2),16 or success of the ablation procedure (APPLE).17 Nevertheless, the above scores, especially CHA2DS2-VASc, have been widely tested for the prediction of mortality in various populations, including patients with AF, stroke, HF, or coronary artery disease.18-20 The CHA2DS2-VASc score might also be predictive of AF in specific populations.21 The use of the 2MACE score for predicting mortality in AF patients was investigated in a previous study.6 Additionally, its usefulness for the classification of cardiovascular risk was shown before in our study on a subgroup of patients with AF and obstructive sleep apnea.22
Rivera‑Caravaca et al6 assessed mortality using the 2MACE score in 2 different cohorts of patients who were followed for a median duration of 7.2 years (693 patients) and 1.01 years (1937 patients). The receiver operating characteristic curve analysis showed that, in both cohorts, the predictive value of the 2MACE score was significantly higher than that of the CHA2DS2-VASc score.
Our present study in 1351 patients followed for a median duration of 81 months adds to the current knowledge on the predictive value of the 2MACE score. It is especially important considering that the current guidelines of both American and European societies show that lifestyle changes, treatment of underlying cardiovascular conditions, and therefore a reduction of cardiovascular risk are vital for improving the life expectancy, quality of life, autonomy, and social functioning of patients with AF.23,24 The implementation of the simple 2MACE score may facilitate risk stratification and prognosis assessment. Especially given the fact that continuous education of physicians treating patients with AF is necessary.25
Our study has several limitations. First, the data were collected prospectively but our results should be regarded as an exploratory post hoc analysis because the risk was assessed retrospectively. Moreover, due to the geographic location and local racial and ethnic distribution, most of our participants were White, which precludes the generalization of the results to populations of other races and ethnicities.
In conclusion, the 2MACE score is a good predictor of long‑term all‑cause mortality in patients with AF. A progressive increase in mortality was observed with an increasing 2MACE score. However, further studies are needed to assess whether aggressive cardiovascular risk reduction in this population is associated with improved prognosis.
- Pistoia F, Sacco S, Tiseo C, et al. The epidemiology of atrial fibrillation and stroke. Cardiol Clin. 2016; 34: 255‑268. | Crossref
- Allan V, Honarbakhsh S, Casas JP, et al. Are cardiovascular risk factors also associated with the incidence of atrial fibrillation? A systematic review and field synopsis of 23 factors in 32 population‑based cohorts of 20 million participants. Thromb Haemost. 2017; 117: 837‑850. | Crossref
- Mahajan R, Pathak RK, Thiyagarajah A, et al. Risk factor management and atrial fibrillation clinics: saving the best for last? Heart Lung Circ. 2017; 26: 990‑997. | Crossref
- Pastori D, Farcomeni A, Poli D, et al. Cardiovascular risk stratification in patients with non‑valvular atrial fibrillation: the 2MACE score. Intern Emerg Med. 2016; 11: 199‑204. | Crossref
- Pastori D, Rivera‑Caravaca JM, Esteve‑Pastor MA, et al. Comparison of the 2MACE and TIMI‑AF scores for composite clinical outcomes in anticoagulated atrial fibrillation patients. Circ J. 2018; 82: 1286‑1292. | Crossref
ARTICLE INFORMATION