Defining right ventricular dysfunction by echocardiography in normotensive patients with pulmonary embolism
Key words: echocardiography, prognosis, pulmonary embolism, right ventricular dysfunction



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Defining right ventricular dysfunction by echocardiography in normotensive patients with pulmonary embolism
Introduction: Although the prognostic value of various echocardiographic parameters of right ventricular dysfunction (RVD) was reported in normotensive patients with acute pulmonary embolism (PE), there is no generally accepted definition of RVD.
Objectives: The aim of the study was to compare echocardiographic parameters for the prediction of an adverse 30‑day outcome and create an optimal definition of RVD.
Patients and methods: Echocardiographic parameters including the right ventricular to left ventricular diameter ratio (RV to LV ratio) and tricuspid annular plane systolic excursion (TAPSE) to predict PE‑related mortality, hemodynamic collapse, or rescue thrombolysis within the first 30 days were directly compared in 490 normotensive patients with PE.
Results: An adverse outcome (AO) was present in 31 patients (6.3%); 8 of them (1.6%) died due to PE. Systolic blood pressure, RV to LV ratio, and TAPSE were independent predictors of AO. The receiver operator characteristic yielded an area under the curve of 0.737 (0.654–0.819; P <0.001) for the RV to LV ratio and 0.75 (0.672–0.828; P <0.001) for TAPSE with regard to an AO. The hazard ratio for AO was 2.5 for the RV to LV ratio of more than 1 (95% CI, 1.2–5.7; P <0.03) and 3.8 for TAPSE of less than 16 mm (95% CI, 1.74–8.11; P = 0.001). A combined RVD criterion (TAPSE <16 mm and RV to LV ratio >1) was present in 60 patients (12%), and showed a positive predictive value of 23.3% with a high negative predictive value of 95.6% regarding an AO (HR, 6.5; 95% CI, 3.2–13.3; P <0.001).
Conclusions: Defining RVD on echocardiography by the RV to LV ratio of more than 1 combined with TAPSE of less than 16 mm identified patients with an increased risk of 30‑day PE‑related mortality, hemodynamic collapse, or rescue thrombolysis, while patients without this sign had a very good 30‑day prognosis.
What's new?
Although it is generally accepted that right ventricular dysfunction (RVD) is of prognostic value in normotensive patients with acute pulmonary embolism (PE), there is no generally accepted RVD definition. We compared directly prognostic value of echocardiographic parameters of 490 normotensive patients with PE. Our data indicated that defining RVD by echocardiography as a combination of the right to left ventricular diameter ratio of more than 1 with a tricuspid annulus plane systolic excursion (TAPSE) of less than 16 mm optimally identified patients with an increased risk of 30‑day PE‑related mortality, hemodynamic collapse, or rescue thrombolysis. In daily practice, right to left ventricular diameter ratio and TAPSE are easy to measure even at the bedside. Thus, we think that defining RVD on echocardiography as described above should be used for risk stratification in normotensive patients with PE. This may contribute to better tailored management in this group of patients.
Introduction
Echocardiography proved to be very useful in the management of patients with acute dyspnea or chest pain.1,2 Visualization of typical echocardiographic abnormalities, including the 60/60 sign, or detection of right heart thrombi in a patient with suspected acute pulmonary embolism (PE) confirms the diagnosis, even at the bedside.3-7 Moreover, echocardiography helps to assess prognosis and guide therapeutic decision making.1,8,9 It is well known that right ventricular (RV) dysfunction (RVD) is a predictor of an increased risk of hemodynamic decompensation in normotensive patients with PE.10-12 Various echocardiographic parameters including RV enlargement and hypokinesis, flattening of intraventricular septum, elevated velocity of tricuspid valve regurgitation, decreased contractility of the RV assessed with tricuspid annular plane systolic excursion (TAPSE) have been reported to be of prognostic value.13 However, it was underlined that a uniform echocardiographic definition of RVD has not been established.14 Of the wide range of echocardiographic parameters, an increased RV to left ventricular (LV) end‑diastolic diameter ratio (RV to LV ratio) and a decreased TAPSE are most frequently used for prognostic assessment.10,11 However, their optimal cutoff values were not validated in previous studies, and the potential superiority of either parameter is still the subject of debate.14 Moreover, a novel echocardiographic prognostic parameter, the ratio of tricuspid regurgitation peak gradient (TRPG) to TAPSE (TRPG to TAPSE ratio), has recently been proposed as a promising index for risk stratification in normotensive patients with PE.15 Therefore, we aimed to compare echocardiographic parameters for the prediction of adverse 30‑day outcome in normotensive patients with acute pulmonary embolism, and to develop an optimal definition of RVD.
Patients and methods
This study is a post hoc analysis of pooled prospective multicenter observational cohorts of patients with acute PE. We prospectively included consecutive patients who were diagnosed with acute PE in 3 cooperating European centers in Poland and Germany. Inclusion criteria were as follows: acute pulmonary embolism confirmed by contrast‑enhanced multidetector computed tomography (CT) with thromboemboli in at least segmental arteries or by high probability ventilation‑perfusion lung scan, hemodynamic stability on admission with systemic systolic blood pressure of at least 90 mm Hg without any circulatory support, and informed consent. Exclusion criteria included known pulmonary hypertension and lack of informed consent. All patents underwent standard transthoracic echocardiography on admission, performed as soon as possible, preferably within 48 hours after the diagnosis. Patients were treated following the guidelines of the European Society of Cardiology,1 and the therapy was not influenced by the study protocol. We included only patients who were normotensive on admission and had not participated in previous studies on the prognostic value of echocardiography.11,16-18 All patients initially received standard anticoagulation therapy, mostly with a weight‑adjusted dose of subcutaneous low‑molecular‑weight heparin, or intravenous unfractionated heparin, or a non–vitamin K antagonist oral anticoagulant (NOAC). Thrombolytic, interventional, or surgical treatment was administered when hemodynamic deterioration occurred. During the hospital stay, a NOAC or oral vitamin K antagonist (target international normalized ratio, 2–3) was initiated, unless contraindicated. The study was conducted in accordance with the amended Declaration of Helsinki; the study protocol was approved by the local independent ethics committees of each participating site and all patients gave informed consent.
Echocardiography
Transthoracic echocardiography for the assessment of RVD was performed by an experienced echocardiographer as soon possible after the admission. Examinations were digitally recorded and reviewed if necessary. In the apical 4‑chamber view, LV and RV end‑diastolic diameters were measured at the level of the mitral and tricuspid valve tips, and the presence of RV hypokinesis was assessed. Right ventricular hypokinesis was assessed qualitatively and quantitatively by the echocardiographer and was diagnosed when RV free wall contraction was markedly decreased when compared with healthy individuals. Interventricular septum flattening was assessed qualitatively in the short‑axis parasternal view and was defined when the septum caused a D‑shaped short‑axis LV cavity profile predominantly during systole.
TAPSE was measured in the M‑mode presentation. Tricuspid valve regurgitation was qualitatively assessed with color Doppler imaging and TRPG was calculated by the simplified Bernoulli formula using tricuspid regurgitant flow peak velocity. The examination was completed by measurement of the inferior vena cava at late expiration. The TRPG to TAPSE ratio was also calculated.
Adverse clinical outcome
After the discharge, patients were followed in an outpatient clinic or were contacted by phone. None of the patients was lost to follow‑up. An adverse 30‑day clinical outcome was defined as at least one of the following: PE‑related death, rescue thrombolysis, or hemodynamic collapse (which was defined as cardiopulmonary resuscitation; or systolic blood pressure <90 mm Hg for at least 15 minutes with signs of end‑organ hypoperfusion; or a need for intravenous catecholamine administration). Death was determined to be PE‑related if it was confirmed at autopsy or if it followed a clinically severe PE episode, either immediately or shortly after an objectively confirmed recurrent event, or when sudden death occurred in the absence of a definitive alternative diagnosis.
Statistical analysis
Data with normal distribution were expressed as mean (SD) and those without normal distribution were expressed as median with range. The t test or Mann–Whitney test were used for comparisons between 2 groups, while the χ2 test was used to compare discrete variables (with Yates correction when needed). The receiver operating characteristic (ROC) analysis was used to determine the area under the curve (AUC) of significant echocardiographic parameters in univariable analysis. AUCs of echocardiographic parameters were assessed and curves were compared pairwise according to the DeLong test. Binary cutoff values of echocardiographic parameters were determined with the Youden index and were used for subsequent calculations. Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated. The impact of echocardiographic parameters on an adverse clinical outcome was evaluated using the multivariable Cox proportional‑hazards regression. All parameters found to be significant in univariable analysis were used in multivariable analysis, with forward stepwise selection with a 0.1 level for staying in the model. All tests were 2‑tailed. Data were considered significant at P value of less than 0.05. The STATISTICA data analysis software system (StatSoft, Inc. 2011, version 10, www.statsoft.com) and MedCalc software (version 11.0.0.0) were used for statistical calculations.
Results
Prospective cohorts of patients with PE who were normotensive at admission were merged in a collaborative database. The study population included 490 patients (287 patients from Warsaw, Poland; 138 patients from Mainz, Germany; 65 patients from Białystok, Poland). An adverse 30‑day clinical outcome occurred in 31 patients (6.3%), including 8 PE‑related deaths, 20 cases of rescue thrombolysis / embolectomy, and 3 patients who experienced hemodynamic deterioration requiring intravenous inotropes. Patients who had an adverse outcome had significantly lower systolic blood pressure compared with those with favorable clinical course. There were no significant differences in heart rate, age, and comorbidities between groups. Patient clinical characteristics are presented in Table 1.
Parameter | All patients (n = 490) | Patients with an adverse outcome (n = 31) | Patients with a favorable course (n = 459) | P value | |
Data are presented as mean (SD) unless otherwise indicated.
Abbreviations: CHF, chronic heart failure; COPD, chronic obstructive pulmonary disease; HR, heart rate; PE, pulmonary embolism | |||||
Sex, n (%) | Female | 229 (46.7) | 12 (38.7) | 217 (47.3) | 0.23 |
Male | 261 (53.3) | 19 (61.3) | 242 (52.7) | ||
Age, y | 64 (18) | 67 (19) | 64 (18) | 0.29 | |
HR, bpm | 89 (19) | 95 (20) | 88 (19) | 0.07 | |
Systemic blood pressure, mm Hg | 134 (21) | 123 (18) | 135 (21) | 0.003 | |
Comorbidities (COPD, CHF, malignancy), n (%) | 170 (35) | 10 (32) | 160 (35) | 0.46 | |
Echocardiography
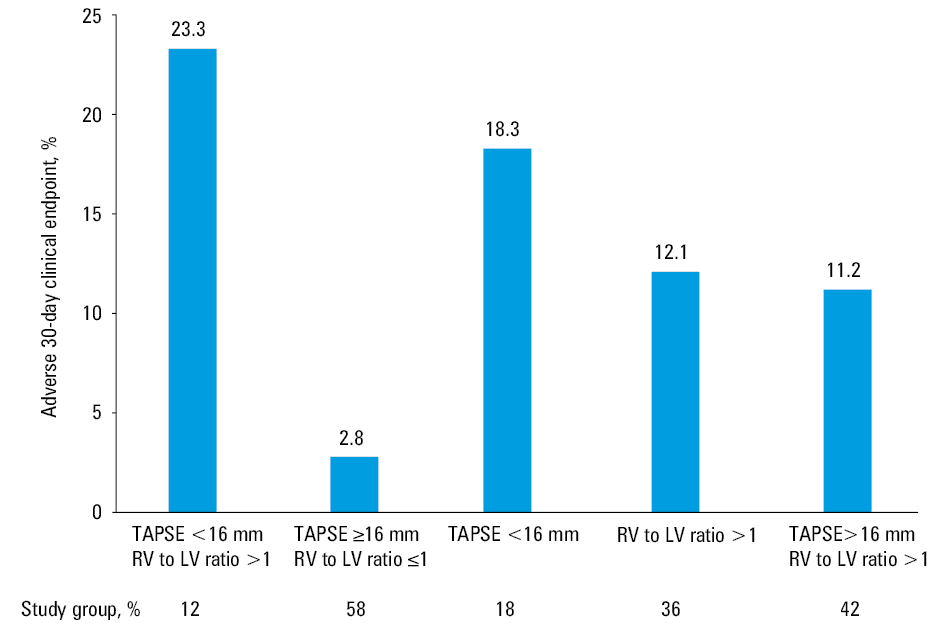
Transthoracic echocardiogram was recommended within 48 hours of PE diagnosis; however, it was performed within 24 hours in 364 patients, and within 72 hours in 52 patients. Those who had an adverse 30‑day outcome presented with more pronounced signs of RVD (Table 2). Figure 1 shows the frequency of 30‑day clinical outcome according to the different echocardiographic parameters of RVD. Patients with an adverse 30‑day outcome had a higher RV to LV ratio (1.2 [0.7–1.7] vs 0.9 [0.5–2.5]; P <0.001) and a lower TAPSE (16 [11–25] vs 21 [5–39] mm; P <0.001) compared to patients with a favorable outcome.
Parameter | All patients (n = 490) | Patients with an adverse outcome (n = 31) | Patients with a favorable course (n = 459) | P value |
Data are presented as mean (SD) or median (range) unless otherwise indicated.
Abbreviations: IVC, inferior vena cava; IVS, interventricular septum; LV, left ventricle; RV, right ventricle; TAPSE, tricuspid annular plane systolic excursion; TRPG, tricuspid regurgitation peak gradient; others, see Table 1 | ||||
RV, mm | 41 (8) | 46 (8) | 41 (8) | <0.001 |
LV, mm | 43 (7) | 41 (6) | 43 (7) | 0.12 |
RV to LV ratio | 0.9 (0.5–2.5) | 1.2 (0.7–1.7) | 0.9 (0.5–2.5) | <0.001 |
TRPG, mm Hg | 33 (8–126) | 38 (16–90) | 33 (8–126) | <0.01 |
TAPSE, mm | 20 (5–39) | 16 (11–25) | 21 (5–39) | <0.001 |
TRPG / TAPSE, mm Hg/mm | 1.6 (0.3–8.3) | 2.4 (0.8–5.2) | 1.6 (0.3–8.3) | <0.001 |
IVS flattening, n (%) | 119 (24) | 15 (48) | 104 (23) | 0.002 |
RV hypokinesis, n (%) | 106 (22) | 11 (35) | 95 (21) | <0.05 |
IVC, mm | 17 (7–32) | 20 (7–27) | 17 (8–32) | 0.1 |
Abbreviations: see Table 2
The Cox regression analysis including clinical data (admission systolic blood pressure and heart rate) and echocardiographic parameters (as presented in Table 2) identified only systolic blood pressure, RV to LV ratio and TAPSE as independent predictors of an adverse outcome (Table 3). Other echocardiographic parameters including the TRPG to TAPSE ratio were not significant in multivariable analysis.
Parameter | HR | 95 CI | P value |
Adjusted for: age, heart rate, right ventricle, tricuspid regurgitation peak gradient, ratio of tricuspid regurgitation peak gradient to tricuspid annular plane systolic excursion, interventricular septum flattening, and right ventricular hypokinesis.
Abbreviations: HR, hazard ratio; SBP, systolic blood pressure; others, see Table 2 | |||
SBP per 1 mm Hg increase | 0.98 | 0.96–0.99 | 0.03 |
RV to LV ratio per 0.1 increase | 1.21 | 1.11–1.33 | <0.001 |
TAPSE per 1mm increase | 0.86 | 0.8–0.92 | <0.001 |
The AUC of the RV to LV ratio and TAPSE with regard to the combined clinical outcome were 0.737 (0.654–0.819; P <0.001) and 0.750 (0.672–0.828; P <0.001), respectively (Figure 2). Comparison by the DeLong test revealed no differences in the AUC of TAPSE and RV to LV ratio (P = 0.89).
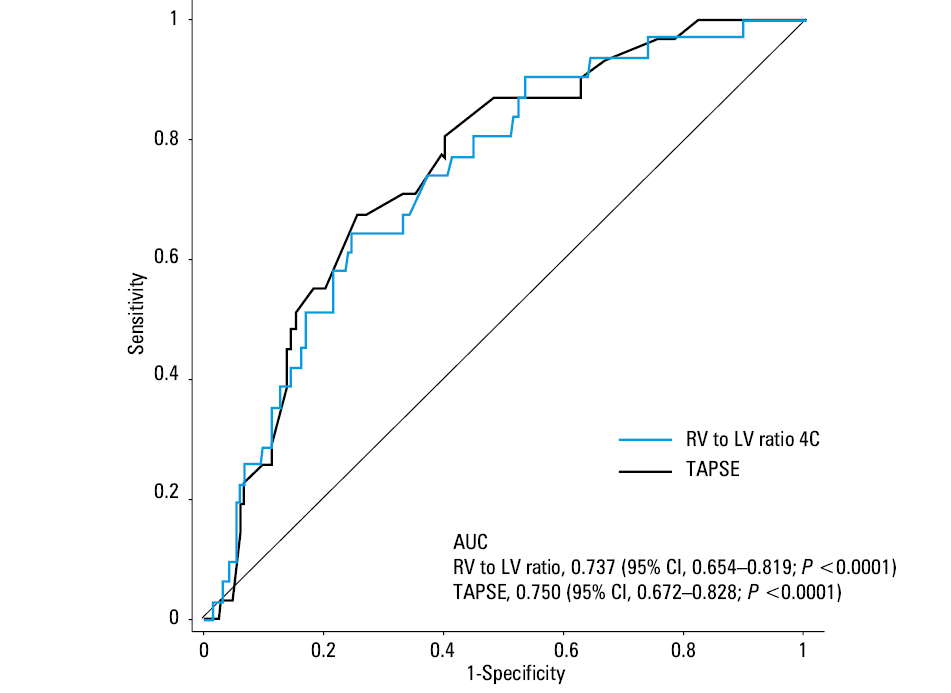
Abbreviations: AUC, area under the curve
Based on the Youden index quantification, the optimal cutoff values were 17 mm for TAPSE (Youden index, 0.423) and 1.07 for the RV to LV ratio (Youden index, 0.397). Due to the fact that they were similar to the previously defined values, cutoffs of TAPSE of less than 16 mm and the RV to LV ratio higher than 1 were used for further analysis. The hazard ratio for reaching an adverse 30‑day outcome was 2.53 for the RV to LV ratio of more than 1 (95% CI, 1.2–5.7; P <0.03) and 3.76 for TAPSE of less than 16 mm (95% CI, 1.74–8.11; P = 0.001). Since both parameters were included in the multivariable model and independently predicted an adverse 30‑day outcome, we assessed the predictive value of coexistence of both criteria. The combined echocardiographic criterion (TAPSE <16 mm and the RV to LV ratio >1) was present in 60 patients (12%) and was associated with a satisfactory PPV and high NPV of 23.3% and 95.6%, respectively, and a hazard ratio of 6.5 (95% CI, 3.2–13.3; P <0.001) (Table 4).
Discussion
We performed a post‑hoc analysis of a large pooled European multicenter cohort to identify the best combination of echocardiographic parameters for risk stratification of normotensive patients with acute PE. The main study findings can be summarized as follows: 1) the RV to LV ratio and TAPSE were found as independent predictors for an adverse 30‑day clinical outcome, and 2) the coexistence of TAPSE of less than 16 mm with the RV to LV ratio of more than 1 identifies patients at higher risk for an adverse outcome.
According to the current guidelines, echocardiographic examination is not mandatory as part of the routine diagnostic workup in hemodynamically stable patients with suspected PE.1,19,20 However, although short‑term prognosis in acute PE predominantly depends on the hemodynamic characteristics and extent of RVD and RV failure, it is generally accepted that RVD detected on echocardiography or CT identifies patients at risk of hemodynamic deterioration despite anticoagulation.21,22 Importantly, RVD also affects the prognosis in patients classified as low risk by the Pulmonary Embolism Severity Index.12 In contrast, hemodynamically stable patients with preserved RV function have a favorable prognosis and are potential candidates for short‑term hospitalization or ambulatory treatment.1 Mortality rates observed in various cohorts of normotensive patients with PE and RVD diagnosed by different echocardiographic criteria varied from 4.3% to 16.4%.13,23 Although systematic reviews and meta‑analyses have suggested that RVD on echocardiography is associated with an elevated risk of short‑term mortality, its overall positive predictive value for PE‑related death was reported to be less than 10%.13 However, this is partly related to the fact that various echocardiographic RVD criteria were proposed.11,13 Moreover, echocardiographic criteria for defining acute RVD are poorly standardized and may vary widely between hospitals, ultrasound laboratories, and even examiners. It should be noted that the RV has a complex morphology and mechanism of contraction. Moreover, the RV is difficult to visualize in its entirety in any single 2‑dimensional echocardiographic view.24,25 Thus, despite a wide set of data supporting the use of echocardiography for risk stratification of normotensive patients with PE, its practical application can be challenging. An increased RV to LV ratio and a decreased TAPSE are related to PE severity26 and are the most frequently used parameters for prognostic assessment.10,11,20 Importantly, a RV to LV ratio of more than 0.9 was the predominant RVD criterion in the largest randomized study on fibrinolysis for patients with intermediate risk PE. In this study, death or hemodynamic decompensation within 7 days occurred in 5.6% of anticoagulated patients.8 Our previous study suggested that TAPSE of less than 16 mm is useful for risk stratification in normotensive patients with PE, and similar TAPSE cutoff values were reported by others.10,11 This large European multicenter prospective cohort study including 490 patients with PE managed according to the current ESC guidelines confirms the significant prognostic value of both echocardiographic parameters. TAPSE and the RV to LV ratio have almost identical AUC in the ROC analysis for the prediction of an adverse 30‑day outcome, indicating their similar prognostic value. Moreover, a multivariable Cox regression analysis including both TAPSE and the RV to LV ratio indicates their additive and independent prognostic value. Of note, the TRPG to TAPSE ratio was also a significant prognostic variable; however, due to strong collinearity with TAPSE, it was found nonsignificant in the multivariable analysis as a factor of lower predictive value. A total of 60 patients (12%) presented with TAPSE of less than 16 mm and the RV to LV ratio of more than 1. An adverse 30‑day outcome occurred in 23% of these patients (Figure 2). The positive predictive value was lower for TAPSE of less than 16 mm (18.3%) and the RV to LV ratio of more than 1 (12.1%) alone. This definition of RVD, combining TAPSE and the RV to LV ratio, was associated with a HR of 6.5 (95% CI, 3.2–13.3; P <0.001) for an adverse 30‑day outcome and a high NPV of 95.6%. Importantly, both TAPSE and the RV to LV ratio are easy to measure, even at the bedside, and are widely available without the need for an advanced echocardiographic technology. Moreover, Doppler tissue imaging‑derived tricuspid annular systolic velocity, a novel parameter of RV function, was recently reported to be inferior to TAPSE for risk assessment in normotensive patients with PE.27
Clinical implications
The RV to LV ratio and TAPSE may help in the management of normotensive patients with PE by identifying patients at risk of hemodynamic deterioration. The combination of a TAPSE of less than 16 mm with a RV to LV ratio of more than 1 was present in 16% of study patients, was associated with a satisfactory PPV of 23%, and allowed to detect almost half of patients who experienced an adverse clinical course despite anticoagulation. Although it is not possible to propose any therapeutic implications from our study, we suggest that patients with RVD according to our new definition should be at least closely monitored.
Study limitations
This is a post‑hoc analysis of a prospective observational study. Our results should ideally be validated in an external population with acute PE. We tried to perform echocardiography as soon as possible after admission, but echocardiography was delayed in some patients. A transthoracic echocardiogram is recommended within 48 hours of PE diagnosis; however, it was performed within 24 hours in 364 patients, and within 72 hours in 52 patients. We found no differences in frequency of adverse outcome between patients in whom TTE was performed within 24 hours and patients who underwent echocardiography later.
Conclusions
Our data indicate that TAPSE and the RV to LV ratio are useful echocardiographic parameters for risk stratification of normotensive patients with PE. The combination of a RV to LV ratio higher than 1 and TAPSE of less than 16 mm identifies patients with an increased risk of adverse 30‑day outcome, while patients without this echocardiographic sign have a very good 30‑day prognosis.
- Konstantinides SV, Torbicki A, Agnelli G, et al. 2014 ESC Guidelines on the diagnosis and management of acute pulmonary embolism. Eur Heart J. 2014; 35: 3033‑3080. | Crossref
- Neskovic AN, Skinner H, Price S, et al. Focus cardiac ultrasound core curriculum and core syllabus of the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. 2018; 19: 475‑481. | Crossref
- Barrios D, Rosa‑Salazar V, Jimenez D, et al. Right heart thrombi in pulmonary embolism. Eur Respir J. 2016; 48: 1377‑1385. | Crossref
- Torbicki A, Kurzyna M, Ciurzynski M, et al. Proximal pulmonary emboli modify right ventricular ejection pattern. Eur Respir J. 1999; 13: 616‑621. | Crossref
- Fields JM, Davis J, Girson L, et al. Transthoracic echocardiography for diagnosing pulmonary embolism: a systematic review and meta‑analysis. J Am Soc Echocardiogr. 2017; 30: 714‑723.e4. | Crossref
ARTICLE INFORMATION