Age-related differences in vitamin D status in Polish centenarians compared with 65-year-olds
Key words: 1, 25-dihydroxycholecalciferol, 25-hydroxycholecalciferol, centenarians, parathyroid hormone, vitamin D



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Age-related differences in vitamin D status in Polish centenarians compared with 65-year-olds
Introduction: Vitamin D status is known to change with age. However, little is known about vitamin D status in centenarians.
Objectives: The aim of the study was to assess vitamin D status and correlations among the levels of parathyroid hormone (PTH), 25‑hydroxycholecalciferol (25[OH]D), 1,25‑dihydroxycholecalciferol (1,25[OH]D), calcium, inorganic phosphorus, and alkaline phosphatase (ALP) activity in centenarians.
Patients and methods: The study group included 97 participants: 81 women and 16 men (median [interquartile range (IQR)] age, 101.4 [100.5–102.16] years). Centenarians were visited at their homes where examinations were conducted and blood samples collected. The control group consisted of 57 elderly subjects: 35 women and 22 men (median [IQR] age, 65.9 [65.3–66.5] years). The concentrations of PTH, 25(OH)D, and 1,25(OH)D were measured in frozen plasma samples, and calcium, phosphorus, and ALP levels, in serum samples.
Results: The median calcium level was 8.88 mg/dl in centenarians versus 9.52 mg/dl in 65‑year‑old subjects (P <0.01); ALP, 223 IU versus 190 IU (P = 0.01); phosphorus, 3.01 mg/dl versus 3.23 mg/dl (P = 0.13); PTH, 45.59 pg/ml versus 29.27 pg/ml (P <0.01); 25(OH)D, 7.39 ng/ml versus 19.81 ng/ml (P <0.01); 1,25(OH)D, 57.5 pmol/l versus 78.6 pmol/l (P <0.01). Only centenarians demonstrated correlations among the measured laboratory parameters.
Conclusions: Considering lower 25(OH)D, 1,25(OH)D, and calcium concentrations in the majority of centenarians, as well as the negative correlation between vitamin D active metabolites and PTH, vitamin D and calcium should be systematically supplemented in the oldest of the elderly.
What's new?
Centenarians are one of the fastest growing populations among the elderly. However, cases of extreme longevity are still underrepresented in the majority of studies. At the same time, this group represents a model of a successful aging process. Considering the uniqueness of this study group, it is impossible to provide observational, prospective data. Despite the small number of subjects, our study is representative for Polish centenarians, and its comparison with the younger group, performed at the beginning of the aging process in the elderly, let us find significant differences between these 2 aging periods. Our study also provides information on vitamin D status in extreme longevity, and such data regarding the Polish population have not been published yet. Likewise, the evaluation of calcium–phosphorus homeostasis and its correlations with the vitamin D concentration have not been studied in this population so far.
Introduction
The process of aging involves interdependent, complex involutional mechanisms at the cellular, organ, and systemic levels. It is still debated whether advanced age should be regarded as a continuation of the lifespan or a distinct stage of life. With advancing age, people appear to change their health status perception, and “geriatric giants” (a term coined by Bernard Isaacs in 1965 to encompass age‑related impairments) contribute to more serious health consequences than in younger individuals.1-3 The population of geriatric patients is significantly influenced by the elderly persons (aged 80 years and older). They represented 2% of the Polish population in 2000, and the fraction increased to 4.4% in 2019.4 Furthermore, the Population Division of the United Nations forecasted that the global number of centenarians could exceed 20 million in 2100.5 The centenarian population exemplifies successful aging. Conversely, it also represents a group with advanced signs and symptoms of aging, often coexisting with an increased prevalence of disability and a wide range of deficiencies.6 Vitamin D deficiency or insufficiency is one of the most commonly observed disorders.
Vitamin D status was widely studied in the last decade. Recent epidemiological research has shown that the concentration of 25‑hydroxyvitamin D may have an impact on various diseases and mortality.7-9
The main cause of aging‑associated vitamin D deficiency is low vitamin D production. The skin concentration of 7‑dehydrocholesterol decreases with age.10 Specifically, for each decade past the age of 40 years, there is approximately a 10% to 15% decrease in the 7‑dehydrocholesterol level. Additionally, about a 35% decrease in intestinal calcium absorption is observed in those older than 70 years.11 This decrease is even greater in women because of reduced fractional calcium absorption and estrogen changes after menopause with increased urinary calcium loss.12 Other causes of aging‑associated vitamin D deficiency are related to poor vitamin D and calcium supply as well as Poland’s latitude (49° N to 54° N). The amount of sunlight sufficient for vitamin D production in the skin is available only between May and September. Apart from that, with advancing age, comorbidities should be considered, renal and liver insufficiency in particular.
Additionally, the impact of vitamin D deficiency on “geriatric giants” is influenced by muscle strength reduction, which may lead to an increased number of falls. Furthermore, the development of secondary hyperparathyroidism results in calcium imbalance and high bone turnover as well as accelerates age‑related bone loss and leads to osteoporotic fractures.13
In all populations, regardless of age, vitamin D status is determined by measuring the total serum 25‑hydroxycholecalciferol (25[OH]D) concentration. However, the recommended 25(OH)D concentration for the oldest of the elderly has been an issue of debate.
The relationship among vitamin D status, the musculoskeletal system condition, and physical performance could be the subject of a separate article. In this study, we focused on vitamin D status in individuals presenting extreme longevity. The primary aim of the study was to assess vitamin D status and evaluate correlations among parathyroid hormone (PTH), 25(OH)D, 1,25(OH)D, calcium, phosphorus, and alkaline phosphatase (ALP) levels in Polish centenarians. Another study objective was to compare the results obtained for centenarians and 65‑year‑old study subjects.
Patients and methods
We used the Polish Centenarians (POLSTU) study, a multidisciplinary program of successful aging, in which 346 subjects over 100 years of age were visited. Biological material was collected from 285 of them. In 97 subjects, a sufficient amount of frozen plasma was taken to conduct vitamin D studies. The bioethics committee of the Central Clinical Hospital of the Ministry of the Interior and Administration in Warsaw (Poland) approved the study. The centenarians or their relatives provided written informed consent to participate in the study.
The study included 2 groups of individuals. The first group consisted of 97 centenarians in whom plasma samples were obtained and subsequently frozen. It included 81 women and 16 men aged 99.9 to 108 years, at a median age of 101.4 years. The other group was a control group of 57 subjects at the age of 65 years: 35 women and 22 men, at a median age of 65.9 years. The exclusion criteria were as follows: severe endocrinopathy or chronic digestive system diseases with malabsorption, advanced heart failure (New York Heart Association class IV), respiratory failure, and severe liver or kidney failure.
All centenarians were visited at their homes in cities, towns, and rural areas, where blood samples were collected. The 65‑year‑olds in the control group were examined and blood samples were obtained in outpatient clinics. The study subjects were examined throughout the year. The methods applied in this study included taking a medical history, performing detailed physical examination, and collecting a blood sample. The baseline characteristics of the study participants are presented in Table 1. Laboratory tests included measuring serum levels of calcium, magnesium, inorganic phosphorus, and ALP activity. Thawed plasma was used to measure the levels of PTH (electrochemiluminescence assay with a range of 15–65 pg/ml), 25(OH)D (enzyme‑linked immunosorbent assay [ELISA] with a range of 47.7–144 nmol/l or 19.08–57.6 ng/ml), and 1,25‑dihydroxycholecalciferol (1,25[OH]D; ELISA with a range of 39–193 pmol/l). Plasma samples were assayed for total 25(OH)D and 1,25(OH)D concentrations using a commercially available ELISA kit (Immunodiagnostic Systems, Ltd., Boldon Colliery, United Kingdom).
Characteristic | Centenarians | 65‑year‑olds | |
a Reference range, 0.6–1.3 mg/dl
b Reference range, 120–160 g/l
c Reference range, 6–8 g/dl
d Reference range, 70–99 mg/dl
Abbreviations: IQR, interquartile range | |||
Male / female sex, n | 81/16 | 35/22 | |
Age, y, median (IQR) | 101.4 (100.5–102.16) | 65.9 (65.3–66.5) | |
Place of living, % | City | 70.7 | 100 |
Town | 12.9 | 0 | |
Village | 16.4 | 0 | |
Body mass, kg, mean (SD) | 51.2 (6) | 70.3 (12) | |
Height, cm, mean (SD) | 148 (7) | 164 (16) | |
Creatinine, mg/dl, mean (SD)a | Men | 0.95 (0.36) | 0.93 (0.21) |
Women | 1.34 (0.53) | 1.07 (0.33) | |
Hemoglobin, g/l, mean (SD)b | 119.7 (15.9) | 137.7 (9.2) | |
Protein, g/dl, mean (SD)c | 6.7 (0.7) | 7.2 (0.3) | |
Glucose, mg/dl, mean (SD)d | 89.7 (36.1) | 97.6 (26.1) | |
Statistical analysis
Laboratory parameter values were expressed as median and interquartile range. Centenarians and controls were compared using the nonparametric Mann–Whitney test. The association between laboratory parameters was assessed with the Pearson correlation coefficient. Study data were analyzed using the R 3.6.1 software (R Core Team, Vienna, Austria).
Results
The median concentrations of calcium and magnesium were significantly lower in centenarians compared with 65‑year‑olds, whereas the ALP activity was significantly higher (calcium, 8.88 mg/dl vs 9.52 mg/dl, P <0.01; magnesium, 1.96 mg/dl vs 2.08 mg/dl, P <0.01; ALP, 223 IU vs 196 IU, P = 0.01). Although the phosphorus concentration was lower in centenarians, the difference was nonsignificant (3.01 mg/dl vs 3.23 mg/dl; P = 0.13). The PTH concentration was significantly higher in centenarians (45.59 pg/ml vs 29.27 pg/ml; P <0.01). However, in contrast, the concentrations of 25(OH)D and 1,25(OH)D were significantly lower (25[OH]D, 7.39 ng/ml vs 19.81 ng/ml, P <0.01; 1,25[OH]D, 57.5 pmol/l vs 78.60 pmol/l, P <0.01). Detailed data are presented in Table 2.
Parameter | Centenarians (n = 97) | 65‑year‑olds (n = 57) | P valuea |
Data are presented as median (interquartile range).
a Mann–Whitney test
b Reference range, 8.08–10.04 mg/dl
c Reference range, 2.5–4.8 mg/dl
d Reference range, 1.8–2.9 mg/dl
e Reference range, 23–290 IU
f Reference range, 15–65 pg/ml
g Reference range, 19.08–57.6 ng/ml or 47.7–144 nmol/l
h Reference range, 39–193 pmol/l
Abbreviations: 1,25(OH)D, 1,25‑dihydroxycholecalciferol; 25(OH)D, 25‑hydroxycholecalciferol; ALP, alkaline phosphatase; PTH, parathyroid hormone | |||
Calciumb, mg/dl | 8.88 (8.35–9.36) | 9.52 (9.22–9.72) | <0.01 |
Inorganic phosphorusc, mg/dl | 3.01 (2.8–3.38) | 3.23 (2.89–3.43) | 0.13 |
Magnesiumd, mg/dl | 1.96 (1.76–2.18) | 2.08 (1.98–2.24) | <0.01 |
ALPe, IU | 223 (184–267) | 190 (151–239) | 0.01 |
PTHf, pg/ml | 45.59 (29.86–65.07) | 29.27 (23.88–42.2) | <0.01 |
25(OH)Dg, ng/ml, nmol/l | 7.39 (5.47–12.36),
18.45 (13.7–30.8) | 19.81 (15.41–24.45),
49.45 (38.47–61.05) | <0.01 |
1,25(OH)Dh, pmol/l | 57.5 (37.4–75.5) | 78.6 (63–116.75) | <0.01 |
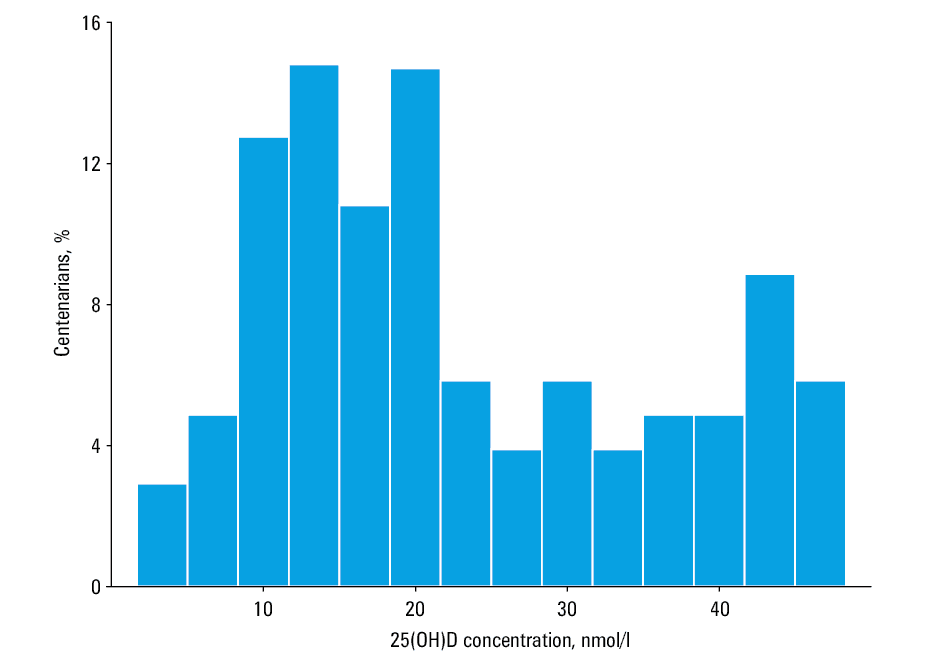
It was found that, in the majority of centenarians (87%), the concentration of 25(OH)D was below the laboratory reference range (Figure 1). Although 13% of centenarians had 25(OH)D concentration within normal limits, in all of them it was distributed in the lower quarter of the reference range. In comparison, 48% of the 65‑year‑old study subjects had a 25(OH)D concentration below the laboratory reference range (Figure 2).
- Morley JE. A brief history of geriatrics. J Gerontol A Biol Sci Med Sci. 2004; 59: 1132‑1152. | Crossref
- Morley JE. The new geriatric giants. Clin Geriatr Med. 2017; 33: 11‑12. | Crossref
- Puvill T, Lindenberg J, Gussekloo J, et al. Associations of various health‑ratings with geriatric giants, mortality and life satisfaction in older people. PLOS One. 2016; 11: 1‑13. | Crossref
- Statistics Poland. Population. Size and structure and vital statistics in Poland by territorial division in 2019. As of 30th June. https://stat.gov.pl/obszary‑tematyczne/ludnosc/ludnosc/ludnosc‑stan‑i‑struktura‑w‑przekroju‑terytorialnym‑stan‑w‑dniu‑30‑06‑2019,6,26.html. Accessed May 15, 2020.
- Robine JM, Cubaynes S. Worldwide demography of centenarians. Mech Ageing Dev. 2017; 165: 59‑67. | Crossref
ARTICLE INFORMATION