Catheter ablation (CA) is a routinely performed procedure in patients with paroxysmal and persistent atrial fibrillation (AF). It has a high rate of success and a relatively low risk of dangerous complications, which are reported to occur in 5% to 7% of patients.1 A rarely observed complication is an intramural atrial hematoma (IAH); however, its exact prevalence, risk factors, and recommended treatment schemes have not been determined. Here, we present our approach to a case of CA‑related IAH.
A 52‑year‑old female underwent pulmonary vein isolation (PVI) for highly symptomatic (the European Heart Rhythm Association score III) paroxysmal AF, which was diagnosed 5 months prior to the procedure. Her medical history included a quadricuspid aortic valve, moderate aortic regurgitation, hypertension, and osteoarthritis. Standard preprocedural transesophageal echocardiography ruled out thrombus within the heart chambers. Left atrium was slightly enlarged with the diameter of 4.5 cm. Circumferential point‑by‑point radiofrequency ablation with the use of a contact force control cool‑tip catheter 35W (ThermoCool SF Biosense Webster, Irvine, California, United States) was performed. The maximal ablation index in the region where hematoma occurred was 420, while maximal contact force was 32 g. Neither sudden impedance spikes nor steam‑pops were observed during the procedure. Heparin (11 500 IU) was administered during the procedure. In total, 77 radiofrequency applications were performed with a total application time of 32 minutes and 28 seconds. Postprocedural transthoracic echocardiography presented no significant pericardial effusion. The patient was discharged home in generally good condition.
Eight days after the procedure, the patient was readmitted due to nonspecific chest pain radiating to the interscapular region, dyspnea, nonproductive cough, and a decreased tolerance of exertion. Transthoracic echocardiography showed IAH on the inferior part of the lateral and posterior wall of the left atrium (Figure 1A) with pericardial effusion, with maximum thickness of 1 cm. Computed tomography (CT) confirmed this diagnosis and showed left inferior pulmonary vein narrowing, which was not occluded (Figure 1C). IAH should be differentiated with atrial thrombus. However, thrombus was ruled out due to the presence of atrial wall rupture, a typical finding in IAH. The department’s Heart Team was consulted and a conservative approach was agreed upon due to the patient’s stable condition. Control transthoracic echocardiography (Figure 1B) and CT (Figure 1D) were performed after a month and showed IAH with a maximal diameter of 26 mm (short heart axis). The subsequent 2‑month follow‑up CT showed IAH with a maximal diameter of 17 mm (short heart axis).
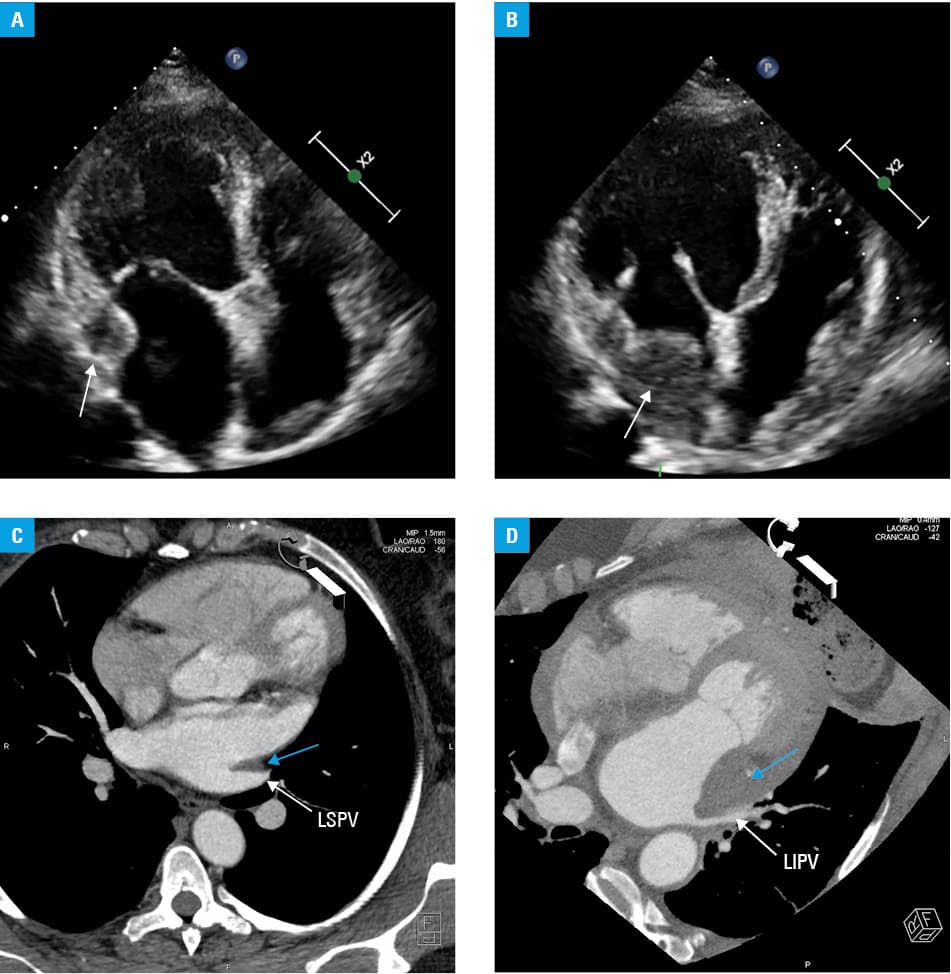
Abbreviations: LIPV, left inferior pulmonary vein; LSPV, left superior pulmonary vein
IAH is an extremely rare event, but it is a possibly fatal complication of CA.2 Currently, there are no guidelines regarding the treatment of this condition. Previous case reports present management depending on the patient’s clinical condition.3,4 The 2 main approaches are surgical intervention or close clinical surveillance. Fukuhara et al2 suggested that most patients require surgery, even if no hemodynamic collapse occurred. However, in another publication, Fukuhara et al5 described IAH resolutions in patients who did not undergo a surgical intervention. Similarly, the presented case demonstrates a successful conservative approach. Therefore, careful consideration should be made before selecting the treatment approach in patients with CA‑related IAH.
- Kirchhof P, Benussi S, Kotecha D, et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J. 2016; 37: 2893‑2962. | Crossref
- Fukuhara S, Dimitrova KR, Geller CM, et al. Left atrial dissection: an almost unknown entity. Interact Cardiovasc Thorac Surg. 2015; 20: 96‑100. | Crossref
- Sah R, Epstein LM, Kwong RY. Images in cardiovascular medicine. Intramural atrial hematoma after catheter ablation for atrial tachyarrhythmias. Circulation. 2007; 115: e446‑447. | Crossref
- Echahidi N, Philippon F, O’Hara G, Champagne J. Life‑threatening left atrial wall hematoma secondary to a pulmonary vein laceration: an unusual complication of catheter ablation for atrial fibrillation. J Cardiovasc Electrophysiol. 2008; 19: 556‑558. | Crossref
- Fukuhara S, Dimitrova KR, Geller CM, et al. Left atrial dissection: etiology and treatment. Ann Thorac Surg. 2013; 95: 1557‑1562. | Crossref
ARTICLE INFORMATION