Parietal cell antibodies: evolution of plasma vitamin B12 during oral supplementation to differentiate true and false positives for pernicious anemia



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Parietal cell antibodies: evolution of plasma vitamin B12 during oral supplementation to differentiate true and false positives for pernicious anemia
Introduction
The Schilling test is not currently available, so the diagnosis of pernicious anemia (PA) is based on the presence of autoimmune atrophic gastritis and intrinsic factor autoantibodies (IFAs) and / or parietal cell autoantibodies (PCAs).1 However, typical autoimmune gastritis can be absent in the early stage of PA and the invasive nature of upper endoscopy limits its use in the elderly patients.2 Plasma gastrin may therefore be used as an indirect marker of fundal atrophy.3
Intrinsic factor autoantibodies have high specificity (98%–100%) for PA, but they are not as sensitive (37%).4 Conversely, PCAs have a high sensitivity (80%) for PA, but are less specific (50%–90%).5,6 So, the isolated presence of PCAs in patients with vitamin B12 deficiency does not allow to confirm the diagnosis of PA.
Despite the absence of active absorption of vitamin B12, oral daily supplementation of 500 to 2000 µg of cyanocobalamin allows for the correction of vitamin B12 deficiency in PA via passive diffusion through enterocytes.7 In the absence of PA, weekly supplementation of vitamin B12 is sufficient.8 This led to a hypothesis that patients with false‑positivity for PCAs would experience a faster correction of plasma vitamin B12 under oral daily supplementation.
Our objective was to compare changes of plasma vitamin B12 levels during oral supplementation between patients with PCAs without PA, those with PCAs and PA, and those with IFAs.
Patients and methods
This study was approved by the bioethical committee of Angers University Hospital (no. 2019/91).
We retrospectively analyzed the medical records of patients presenting with vitamin B12 deficiency and IFA and / or PCA followed between January 2015 and December 2018 in the Department of Internal Medicine of Angers University Hospital. Patients with supplementation doses other than 1000 µg daily oral cyanocobalamin were excluded.
Vitamin B12 deficiency was defined as plasma vitamin B12 levels of 200 ng/l or lower, or between 201 and 350 ng/l with an elevation of plasma homocysteine (≥13 µmol/l in women, ≥15 µmol/l in men, in the absence of folate deficiency or renal failure with creatinine clearance <30 ml/min/1.73 m2).9,10 Plasma vitamin B12 assays were normally prescribed at regular time points but, as patients may have delayed some control assays, we kept real time delays for analyses. Intrinsic factor autoantibodies were tested by an immunodot assay (Biermer atrophic gastritis dot, Alphadia, Wavre, Belgium). Parietal cell autoantibodies were tested by an immunodot assay (Biermer atrophic gastritis dot, Alphadia) and by indirect immunofluorescence on the rat stomach tissue (Biosystems, Barcelona, Spain). Plasma gastrin was used as an indirect marker of fundal atrophy in patients who could not undergo gastroscopy.3,11 Gastrin levels were considered elevated if they were higher than 120 pg/ml or higher than 610 pg/ml in patients treated with proton‑pump inhibitors.3,11
Three groups were formed: IFA (presence of IFAs), PCA‑PA (PCAs without IFAs with histological autoimmune gastritis2 or with elevated gastrin level) and PCA‑noPA (PCAs without IFAs, autoimmune gastritis, nor elevated gastrin level).
The qualitative data were compared by the Fisher exact test. The quantitative data were presented with median (interquartile range [IQR]). The normality of the distribution was tested by means of the d’Agostino–Pearson test. The data were not normally distributed and were therefore compared by Mann–Whitney or Kruskall–Wallis tests. To summarize the evolution of plasma vitamin B12 over time, the best fitting model was linear regression compared to semilog line and composite (binding saturation) models with the least squares method (Supplementary material, Table S1). We performed a runs test to verify that the line fit by linear regression did not differ from the data distribution. Slopes were compared with the F test. The alpha risk was set at 5%. The analyses were carried out using the Graphpad Prism software, version 6.01 (GraphPad Software, Inc., La Jolla, California, United States).
Results
Out of 49 patients followed for PA in our department during the study period, we included 26 patients receiving the same dose of vitamin B12 supplementation (1000 µg of oral cyanocobalamine daily) and fulfilling the inclusion and exclusion criteria. The IFA, PCA‑PA, and PCA‑noPA groups included 6, 14, and 6 patients, respectively, with a median follow‑up of 19 (13–24) months.
The population of the 3 groups is described in Supplementary material, Table S2. The 3 groups were similar in terms of follow‑up time, and clinical and biological consequences of vitamin B12 deficiency. The confounding causes of vitamin B12 deficiency or increase are detailed in Suplementary material, Table S2. Proton‑pump inhibitors were used in 8 patients (3, 3, and 2 in the IFA, PCA‑PA, and PCA‑noPA groups, respectively). No patient was vegan or vegetarian. Helicobacter pylori was found in 2 patients in the PCA‑PA group and in 1 patient in the PCA‑noPA group. One patient presented chronic liver disease in the PCA‑noPA group, but no other causes of elevated vitamin B12 were identified in the studied population (no myeloid blood malignancy, solid cancer, or mild‑to‑severe chronic renal failure).
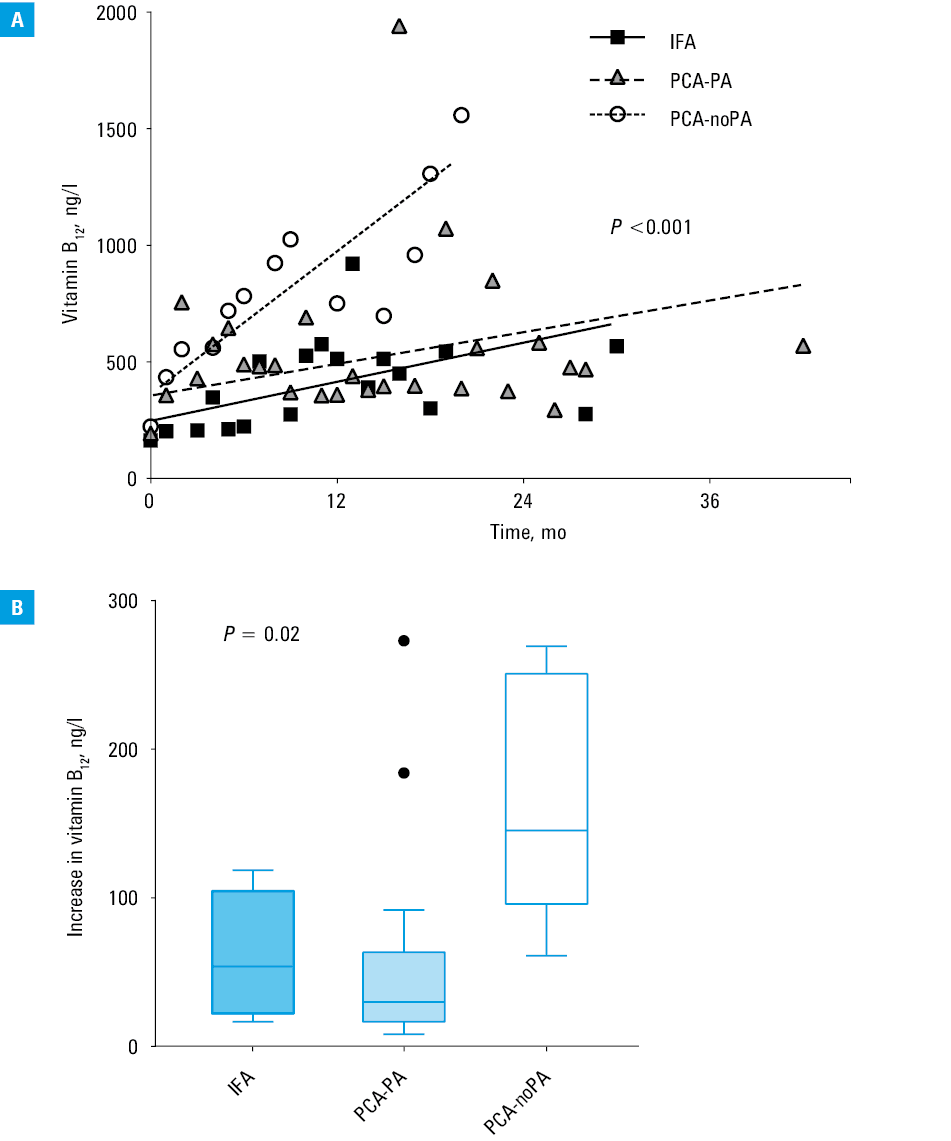
The slopes from regression lines for plasma vitamin B12 evolution differed between the PCA‑noPA group and the 2 other groups: patients with PA showed a slower increase of the plasma vitamin B12 concentration after oral supplementation than patients with false‑positive PCA (P <0.001, Figure 1A). The absolute increase in plasma vitamin B12 from the baseline level after 3 months of supplementation also differed (P = 0.02, Figure 1B).
Discussion
We did not observe any differences according to the presence or absence of IFAs in patients with PA. Similarly to Amarapurkar et al,11 our results showed that it is probably the same disease with different immunological profiles. Conversely, the evolution of plasma vitamin B12 during daily oral supplementation of 1000 µg of cyanocobalamin was much faster in patients with false‑positivity for PCA. This could be explained by the persistence of active absorption mechanisms of vitamin B12 in patients without PA, as the cyanocobalamin is directly absorbable (not bound to vitamin B12-binding proteins from food). Interestingly, this difference was significant after 3 months of supplementation and this simple marker could provide a diagnostic help, especially in patients unable to undergo gastroscopy. Indeed, patients with PA had a median increase of vitamin B12 level of around 50 ng/l (IFA and PCA‑PA groups) whereas patients with false‑positive PCA had a median increase of around 150 ng/l after 3 months of vitamin B12 supplementation.
Our choice to only include patients with a supplementation dose of 1000 µg of cyanocobalamin per day was based on clinical practice: in case of parietal cell antibodies, the common strategy would be to treat as PA to avoid delayed deficiency correction.
Different methods were used to make the diagnosis of PA, according to the ability of patients to undergo gastroscopy. As a consequence, a histological proof of autoimmune gastritis was not obtained in all patients, which is commonly encountered in daily practice. The difficulty to make the diagnosis in some elderly patients underlines the need for additional tests helping to make the diagnosis, similarly as the proposed vitamin B12 evolution under supplementation.
The main limitation of our study was the small sample size of subgroups. However, PA is a rare disease9,12 and our sample size was reasonably comparable to the number of patients with PA in prior studies.11,12 We initially planned to exclude patients with different dosages of vitamin B12 supplementation other than 1000 µg per day and patients with intramuscular supplementation in order to apply a rigorous methodology even if this has led to a small sample size. Finally, the difference between false‑positive PCA and the other patients was large enough to be statistically significant despite the small sample size.
The evolution of plasma vitamin B12 had the best fit with the linear model to limit the least squares. However, we may not exclude that the curves in groups IFA and PCA‑PA would follow a semi‑log model with more patients.
In conclusion, the evolution of plasma vitamin B12 during oral supplementation could help to differentiate between PA and other causes of vitamin B12 deficiency. This may be useful in patients in whom the diagnosis cannot be confirmed, and especially in cases of isolated PCA without histological evidence of autoimmune gastritis.
- Neumann WL, Coss E, Rugge M, Genta RM. Autoimmune atrophic gastritis – pathogenesis, pathology and management. Nat Rev Gastroenterol Hepatol. 2013; 10: 529‑541.
- Coati I. Autoimmune gastritis: pathologist’s viewpoint. World J Gastroenterol. 2015; 21: 12179.
- Miceli E, Padula D, Lenti MV, et al. A laboratory score in the diagnosis of autoimmune atrophic gastritis: a prospective study. J Clin Gastroenterol. 2015; 49: e1‑e5.
- Lahner E, Norman GL, Severi C, et al. Reassessment of intrinsic factor and parietal cell autoantibodies in atrophic gastritis with respect to cobalamin deficiency. Am J Gastroenterol. 2009; 104: 2071‑2079.
- Rusak E, Chobot A, Krzywicka A, Wenzlau J. Anti‑parietal cell antibodies – diagnostic significance. Adv Med Sci. 2016; 61: 175‑179.
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION