Recurrent postprandial abdominal pain that is out of proportion to physical examination (angina) is the most characteristic symptom of chronic intestinal ischemia. Due to this, patients develop fear of eating which results in alarming weight loss. The remaining symptoms, including refractory diarrhea, are highly unspecific. Altogether, the clinical presentation might mimic other conditions, especially gastrointestinal malignancies. Hence, before reaching the final diagnosis, patients undergo extensive, often invasive, diagnostic evaluation. This includes endoscopic examinations, multiple imaging studies, and various laboratory tests.1-4
We hereby present a case of a 80‑year‑old woman admitted to the emergency unit due to acute exacerbation of recurrent abdominal pain that reportedly occurred for the past year. As the pain occurred postprandially, the patient substantially limited her food intake, which resulted in alarming weight loss of 12 kg in 12 months. She reported refractory diarrhea as well. Prior medical record indicated numerous abdominal ultrasound examinations, gastroscopy and colonoscopy, all of which were performed due to an alarming clinical presentation and were negative for significant pathologies, except for severe atherosclerosis of the abdominal aorta. For this reason, Doppler ultrasound was performed, which indicated hemodynamically significant stenoses of the celiac trunk (TC) and superior mesenteric artery (SMA). These were further confirmed by computed tomography angiography, which additionally revealed stenosis of the inferior mesenteric artery (Figure 1A). The patient did not consent to the proposed endovascular treatment at the time.
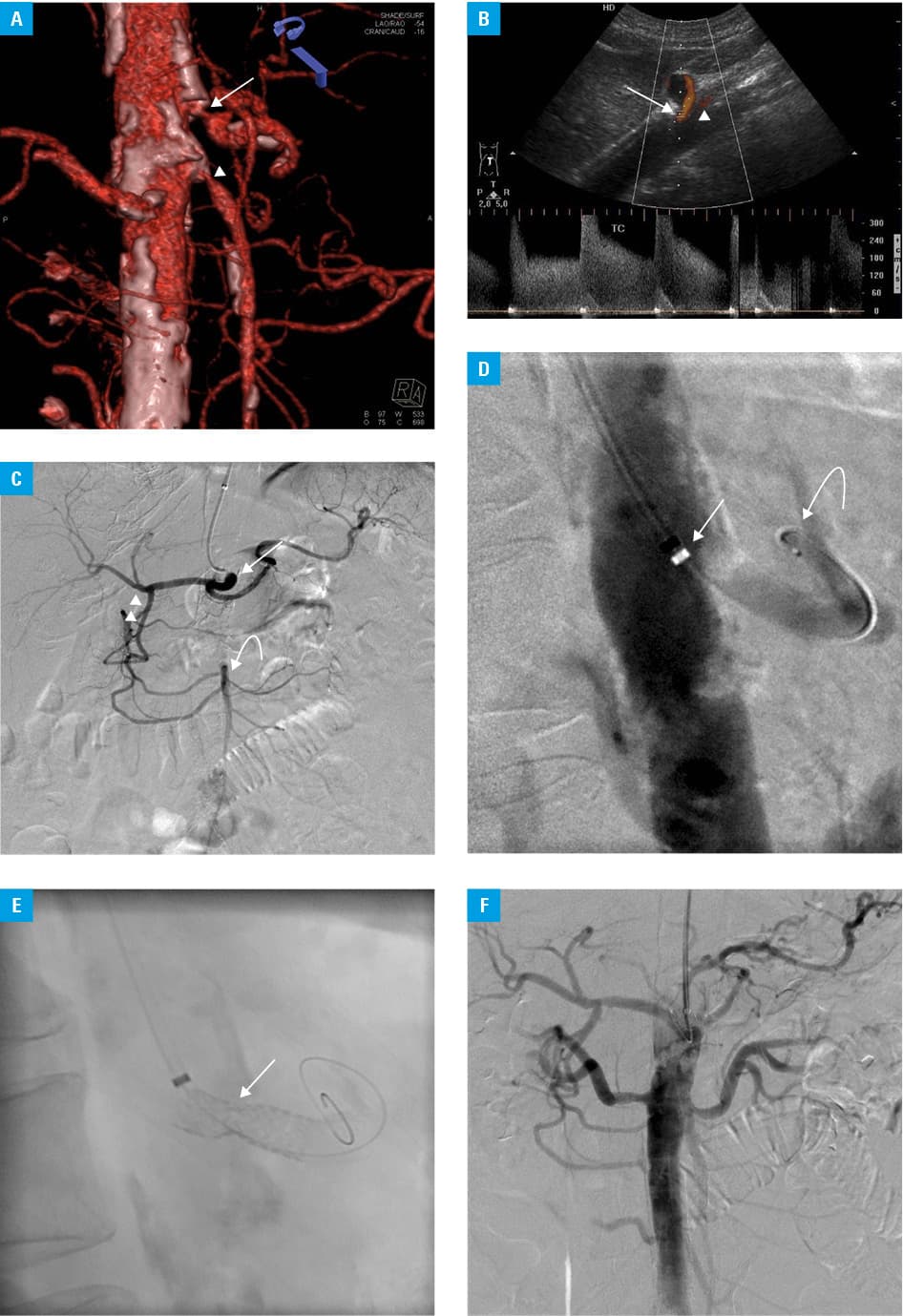
The progressive course of the disease resulted in consecutive hospitalization within 3 months from the previous admission. Repeated Doppler ultrasound showed no flow through the SMA with concomitant critical TC stenosis, which were responsible for the aggravation of symptoms (Figure 1B). The patient was qualified for emergency percutaneous angioplasty of the affected visceral arteries (Figure 1C–1F). Unfortunately, it was impossible to restore physiological splanchnic circulation because of long‑segment occlusion of the SMA. Nonetheless, angioplasty facilitated collateral circulation via the TC. Pain symptoms resolved immediately after the procedure and were not observed following the first (1 hour from the procedure) or any subsequent meals. No complications were observed during 30‑day follow‑up. Control Doppler scan confirmed patency and proper blood flow across the stent.
The presented case depicts diagnostic problems encountered in patients with abdominal angina. Limited knowledge on the entity results in an extended diagnostic workup, which may preclude restoration of the physiologic circulation, or even expose the patient to risky open surgical procedures. Extensive abdominal ultrasound with Doppler evaluation of major abdominal vessels should be included in the diagnostic protocol of each patient with acute abdominal pain and significant weigh loss to exclude possible vessel occlusion (especially in the setting of atherosclerosis). High efficacy and low complication rates compared with a classic surgery, make endovascular treatment a primary choice for patients with chronic intestinal ischemia. Assessment of the long‑lasting efficacy may pose a problem that can be readily resolved by repeated Doppler ultrasound examinations at set time points, which enable detection of patients requiring reintervention.
- Oderich GS, Malgor RD, Ricotta JJ. Open and endovascular revascularization for chronic mesenteric ischemia: tabular review of the literature. Ann Vasc Surg. 2009; 23: 700‑712. | Crossref
- Mateo RB, O’Hara PJ, Hertzer NR, et al. Elective surgical treatment of symptomatic chronic mesenteric occlusive disease: early results and late outcomes. J Vasc Surg. 1999; 29: 821‑831. | Crossref
- Silva JA, White CJ, Collins TJ, et al. Endovascular therapy for chronic mesenteric ischemia. J Am Coll Cardiol. 2006; 47: 944‑950. | Crossref
- Fioole B, van de Rest HJ, Meijer JR, et al. Percutaneous transluminal angioplasty and stenting as first‑choice treatment in patients with chronic mesenteric ischemia. J Vasc Surg. 2010; 51: 386‑391. | Crossref
ARTICLE INFORMATION