Gallstone ileus concurrent with cholelithiasis in a patient with stage 5 chronic kidney disease



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Gallstone ileus concurrent with cholelithiasis in a patient with stage 5 chronic kidney disease
Gallstone ileus—a mechanical bowel obstruction caused by the displacement of a gallstone from the bile ducts or the gallbladder via the biliary enteric fistula to the gastrointestinal tract—accounts for 1% to 4% of all cases of ileus and represents an uncommon complication of cholelithiasis.1,2 It occurs in 0.3% to 0.5% of all patients with gallstones, more frequently in the elderly population and women.2,3 Symptoms are nonspecific, common to all types of ileus. Characteristic patient complaints include nausea, vomiting, constipation as well as abdominal distension and pain. Imaging is the basic method used to establish the diagnosis. The treatment of choice is a surgery using an open, a laparoscopic, or a less common endoscopic approach.1,4
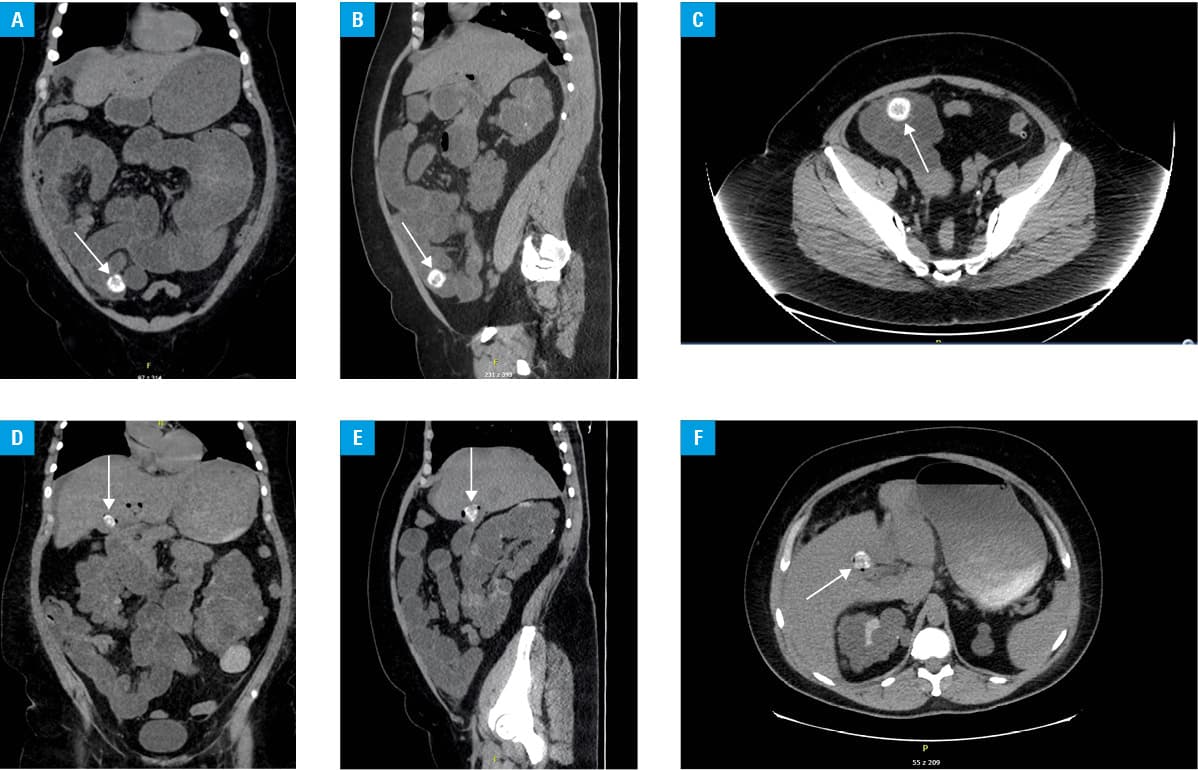
Here, we present the case of a 48‑year‑old obese woman with chronic stage G4 / G5 kidney disease due to polycystic kidney disease, with comorbidities including hypertension, diverticulosis, epilepsy, and a history of thyroidectomy secondary to thyroid cancer. She was admitted to the nephrology department because of exacerbated renal failure and migrating abdominal pain. The patient underwent hemodialysis treatment owing to a high urea level, hyperkalemia, and oliguria. As the abdominal pain did not resolve, became diffuse, was accompanied by bloating and then fecal vomiting, urgent ultrasonography was performed and followed by computed tomography. Imaging revealed features typical of bowel obstruction: computed tomography showed dilated loops of the small bowel, air‑fluid levels, and a round, calcified concretion of 25 mm in diameter in the ileum (Figure 1A–1C). Another, similar in size, concretion was detected in the gallbladder and accompanied by the presence of air in the biliary system (Figure 1D–1F). Based on that, the diagnosis of gallstone ileus was established. The patient was transferred to the surgical ward and underwent urgent surgery due to progressive symptoms of ileus. During the procedure, the gallbladder turned out to be necrotic and a cholecystoduodenal fistula was found. Laparotomy with concretion removal, cholecystoduodenal fistula closure, and cholecystectomy were performed. The postoperative course was complicated by the features of biliary fistula and relaparotomy with the Kehr T‑tube insertion was necessary. After both procedures, the patient’s condition was severe and she was transferred to the intensive care unit for treatment and surveillance. There, she finally recovered after several weeks.
This case is an example of a very rare type of gallstone ileus causing abdominal pain that could mimic the symptoms of uremia in a patient with end‑stage kidney disease and a history unremarkable for gallstones. Metabolic ileus due to uremia or hyperkalemia was a more obvious reason of the presented symptoms. However, numerous other causes were also possible, such as adhesions after surgeries, hernias, fecaliths, intussusception, volvulus, and opioid overdose. This example points to the significance of broad differential diagnosis and considering less obvious diseases and conditions especially in patients with multiple comorbidities. A very interesting example of an atypical localization of gallstones was reported by Ohira et al,5 who described an impacted stone at the Vater ampulla. That patient suffered from epigastric pain resembling the symptom of pancreatitis. Retrograde cholangiopancreatography was performed and demonstrated an enlarged Vater ampulla with gallstone deposition.5 Both cases show that establishing the diagnosis of such a frequent condition as gallstones may be tricky and cholelithiasis may lead to unexpected complications.
- Jakubauskas M, Luksaite R, Sileikis A, et al. Gallstone ileus: management and clinical outcomes. Medicina. 2019; 55: 598‑607. | Crossref
- Nuno‑Guzman CM, Marin‑Contreras ME, Figueroa‑Sanchez M, Corona JL. Gallstone ileus clinical presentation, diagnostic and treatment approach. World J Gastrointest Surg. 2016; 8: 65‑76. | Crossref
- Morosin T, De Robles MSB, Putnis S. Gallstone ileus: an unusual cause of intestinal obstruction. Cureus. 2020; 12: e7284‑e7290. | Crossref
- Inukai K. Gallstone ileus: a review. BMJ Open Gastroenterol. 2019; 6: e000344‑e000347. | Crossref
- Ohira T, Miyazato K, Arakaki S, et al. A gallstone impaction at the ampulla of Vater. Pol Arch Intern Med. 2018; 128: 779. | Crossref
ARTICLE INFORMATION