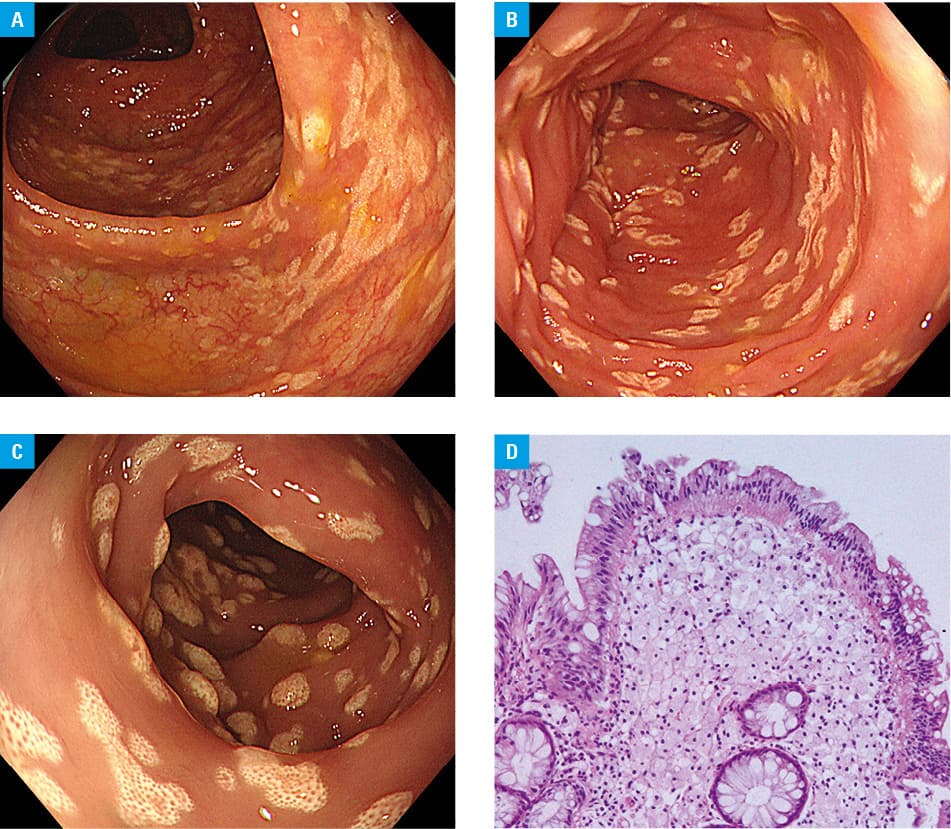
A 32‑year‑old woman with a history of endoscopic mucosal resection for colon adenoma 2 years earlier visited our hospital for examination of incidentally elevated tumor markers (CA19‑9, 43.5 U/ml). Considering the risk of colorectal cancer, we performed colonoscopy. It showed small, flat, smooth‑surfaced, yellowish‑white plaques diffusely distributed in the entire colon (Figure 1A–1C). Histopathological evaluation of biopsy specimens of the colorectal lesions showed numerous foamy histiocytes in the lamina propria, indicative of xanthoma (Figure 1D). The foamy histiocytes were absent in the submucosa.
Gastrointestinal xanthomas are rare non‑neoplastic lesions characterized by the accumulation of foam cells in the lamina propria.1 Originally termed “Lipoidinseln,” these lesions have more recently been called xanthelasma or xanthoma.2 Gastrointestinal xanthomas are smooth, yellowish‑white, tumor‑like benign lesions that are commonly seen in association with dyslipidemia, chemotherapy or radiotherapy, and infections in immunosuppressed patients. Gastrointestinal xanthomas most frequently occur in the stomach, and the incidence of upper gastrointestinal xanthomas was reported to be only 0.23%.3 The incidence of colorectal xanthoma is, thus, expected to be even lower. Several studies have reported that, in most cases, colorectal xanthomas occurred in the rectosigmoid,4,5 and previous minute mucosal injury was suggested to account for the pathogenesis.
In the described case, diffuse xanthomas were observed throughout the colon. No xanthomas were seen on previous colonoscopy, and the patient had no significant medical history, eg, remarkable for hyperlipidemia. Although the specific mechanism of diffuse xanthoma formation in our case remains unclear, it might be related to mechanical irritation associated with previous colonoscopy.
- Vimala R, Ananthalakshmi V, Murthy M, et al. Xanthelasma of esophagus and stomach. Indian J Gastroenterol. 2000; 19: 135.
- Hirokawa M, Takenaka R, Takahashi A, et al. Esophageal xanthoma: report of two cases and a review of the literature. J Gastroenterol Hepatol. 2003; 18: 1105‑1108. | Crossref
- Gencosmanoglu R, Sen‑Oran E, Kurtkaya‑Yapicier O, Tozun N. Xanthelasmas of the upper gastrointestinal tract. J Gastroenterol. 2004; 39: 215‑219. | Crossref
- Nakasono M, Hirokawa M, Muguruma N, et al. Colorectal xanthomas with polypoid lesion: report of 25 cases. APMIS. 2004; 112: 3‑10. | Crossref
- Díaz Del Arco C, Álvarez Sánchez Á, Fernández Aceñero MJ. Non‑gastric gastrointestinal xanthomas: case series and literature review. J Gastrointestin Liver Dis. 2016; 25: 389‑394. | Crossref
ARTICLE INFORMATION