Nonalcoholic fatty liver disease and the risk of metabolic comorbidities: how to manage in clinical practice
Key words: arterial hypertension, dyslipidemia, nonalcoholic fatty liver disease, type 2 diabetes



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Nonalcoholic fatty liver disease and the risk of metabolic comorbidities: how to manage in clinical practice
Nonalcoholic fatty liver disease (NAFLD) is a clinical condition that encompasses various forms of liver damage not caused by chronic alcohol consumption. In the absence of other etiologies, it ranges from steatosis to nonalcoholic steatohepatitis and cirrhosis. The prevalence of NAFLD has considerably increased over the last years owing to the current lifestyle (unhealthy diet and sedentarism). Besides, it is associated with metabolic risk factors such as obesity, arterial hypertension, dyslipidemia, and type 2 diabetes. Given the poor prognosis of patients with advanced NAFLD, a practical therapeutic approach is necessary to halt its natural history. However, no licensed drugs have been approved for this purpose to date. Nowadays, we are in a race to find the first drug able to stop the incidence of NAFLD and reverse the disease in patients at more advanced stages. Meanwhile, the management of the NAFLD metabolic overload, including weight loss, cardiovascular protection, insulin sensitization, and lipid reduction, is the only strategy to improve hepatic and extrahepatic outcomes. In this review, we aimed to describe the management of the main metabolic disorders related to NAFLD, such as type 2 diabetes, arterial hypertension, and dyslipidemia.
Introduction
Nonalcoholic fatty liver disease (NAFLD) is a clinicopathological syndrome associated with metabolic syndrome, defined as a cluster of 3 of the following features: increased waist circumference, abnormal fasting glucose levels or type 2 diabetes (T2D), arterial hypertension, hypertriglyceridemia, and low levels of high‑density lipoprotein (HDL) cholesterol.1 A recent meta‑analysis involving 8.5 million individuals from 22 countries has shown that more than 80% of patients with NAFLD were obese, 72% had dyslipidemia, and 44% had T2D.2 This association is due to the overlapping of NAFLD pathogenetic mechanisms with those of metabolic syndrome, including genetic predisposition, insulin resistance (IR), oxidative stress, chronic and systemic microinflammation, and reduced adiponectin levels.3 Owing to this strong association, patients who present with metabolic syndrome need to be examined for the risk of NAFLD and, vice versa, patients with NAFLD should be evaluated for all components of metabolic syndrome.4
Physicians face the challenge of the early diagnosis and intervention in NAFLD, and there are few pharmacological agents with proven efficacy. It is necessary to proactively assess the presence of cardiovascular disease in patients with NAFLD, regardless of the presence or absence of classic risk factors.5 The management of the metabolic overload of NAFLD, including weight loss, cardiovascular protection, insulin sensitization, and lipid reduction, is currently the only strategy to improve hepatic and extrahepatic outcomes. In this review, we aimed to characterize the management of the main metabolic disorders associated with NAFLD, such as T2D, arterial hypertension, and dyslipidemia.
The first step to manage nonalcoholic fatty liver disease
Lifestyle interventions
The most critical intervention is to endorse a healthy lifestyle that promotes weight loss and control of cardiovascular risk factors (see figure 1).6,7 The European and American guidelines emphasize the importance of modifying lifestyle in the absence of approved pharmacological agents for the treatment of NAFLD.5,8,9 A single randomized controlled trial examined the effect of lifestyle intervention using a combination of diet and exercise (200 min/week).10 After 48 weeks of intervention, a weight reduction greater than 7% led to a significant improvement in the NAFLD Activity Score (NAS). Vilar‑Gomez et al11 reported similar results, with the highest rates of NAS reduction and fibrosis regression in patients who achieved weight loss greater than 10%. Based on these studies, at the early stages of NAFLD, recommending a loss of 5% to 7% of body weight might be sufficient.
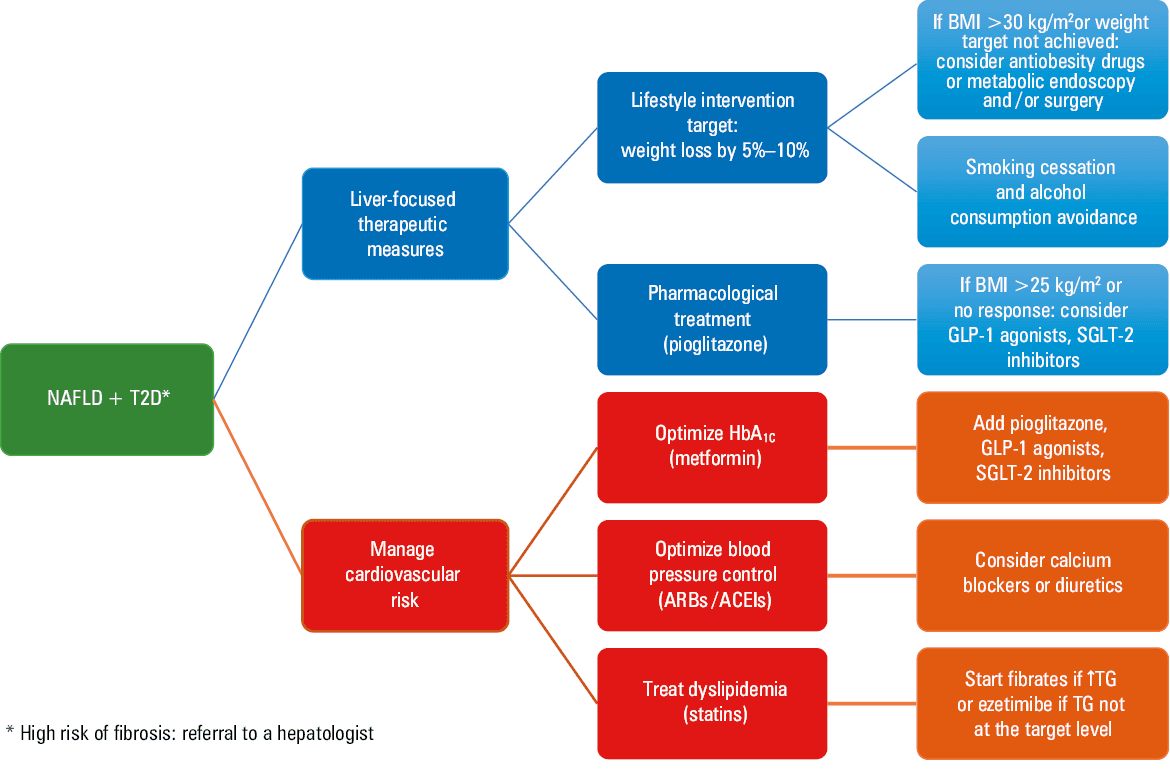
Abbreviations: ACEI, angiotensin converting enzyme inhibitor; ARB, angiotensin II receptor blocker; BMI, body mass index; GLP‑1, glucagon‑like peptide 1; HbA1C, hemoglobin A1C; NAFLD, nonalcoholic fatty liver disease; NASH, nonalcoholic steatohepatitis; SGLT‑2, sodium‑glucose cotransporter 2; TG, triglyceride; T2D, type 2 diabetes
In the case of T2D, pharmacological treatment should be started as an adjunct to recommending reduction of body weight greater than 7%.5,8,12 Besides, interventions that improve metabolic abnormalities in patients with T2D have been proven to be beneficial in NAFLD (figure 2). Furthermore, it should be considered that smoking is associated with advanced liver fibrosis mediated by an increase in IR. Therefore, smoking cessation is essential to reduce the effect of cardiovascular risk factors enhanced by this condition.5,8 Concerning alcohol consumption, although the effect of some degree of regular alcohol consumption over lifetime is controversial,13,14 alcohol intake should be discouraged in patients with NAFLD and T2D.8 Recently, Xu et al15 demonstrated that low‑to‑moderate alcohol consumption was associated with an increased risk of T2D in patients with NAFLD.
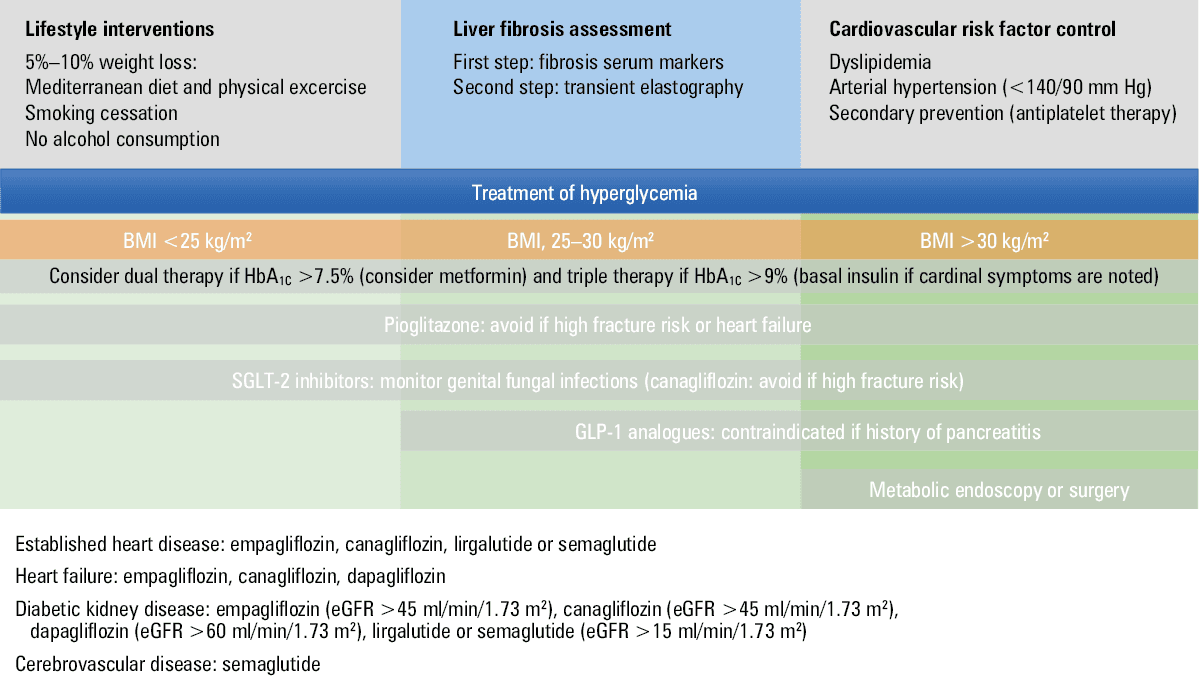
Abbreviations: eGFR, estimated glomerular filtration rate; others, see figure 1
The European Society of Cardiology and the European Society of Hypertension guidelines for the management of arterial hypertension suggest that a healthy lifestyle may be sufficient to delay or prevent the need for drug therapy in patients with grade 1 arterial hypertension.16 The recommendations about the lifestyle associated with blood pressure (BP) reduction include weight loss, regular physical activity, smoking cessation, and dietary interventions.16 Weight loss and the maintenance of an optimal body mass index (BMI) (approximately 20–25 kg/m2)17 are recommended to prevent hypertension, reduce BP, and improve the efficacy of medication in hypertensive patients.16 Epidemiological studies have shown that the treatment and prevention of hypertension may be enhanced by regular aerobic physical activity, which also reduces cardiovascular risk and mortality.17 A growing body of evidence has suggested that hypertensive patients should be advised to participate in at least 30‑minute moderate‑intensity aerobic exercise sessions (walking, jogging, cycling, or swimming) on 5 to 7 days per week.17 Regarding dietary changes, hypertensive patients should be recommended to follow a healthy, balanced diet containing vegetables, legumes, fresh fruit, low‑fat dairy products, whole grains, fish, and unsaturated fatty acids (especially olive oil) and promoting a low consumption of red meat and saturated fatty acids.18,19 The Mediterranean diet, which includes many of these nutrients,18,19 significantly reduces blood pressure20 and has similar beneficial effects on blood glucose and lipid levels.
Physical exercise
Regardless of weight loss, physical exercise reduces IR and metabolic risk factors in patients with NAFLD.9,21 The intensity and duration of physical exercise necessary to significantly reduce liver fat have not been defined yet. Guidelines recommend patients to do moderate aerobic exercise for 150 to 250 minutes per week,22 although better results may be achieved with exercising longer than 250 minutes per week.21 Similarly, resistance or high‑intensity interval training (3 series of 10 repetitions at 70% to 80% of the maximum amount of weight that a person can possibly lift during a single repetition, with 1 minute of recovery between series) are also beneficial for patients with NAFLD.23
Dietary treatment
Reduced caloric intake and improved macronutrient composition may prevent NAFLD progression, independently of weight loss.24 Dietary adherence is an essential determinant of weight loss sustainability. Therefore, in the dietary treatment of NAFLD, it is important to provide practical highlights customizing the diet to the individual’s taste. Some studies have identified dietary habits that may promote NAFLD directly by modulating hepatic triglyceride accumulation and antioxidant activity and, indirectly, by affecting insulin sensitivity and postprandial triglyceride metabolism.25 The Western diet, which is generally characterized by a high consumption of carbohydrates, simple sugars, saturated fats, trans fats, animal proteins (red meat), processed food, and low fiber intake, is associated with NAFLD development and progression.26
Dietary advice should include caloric restriction and adherence to the macronutrient composition typical of the Mediterranean diet.5,24 The Mediterranean diet is a dietary pattern supported by probably the greatest body of evidence of long‑term cardiometabolic benefits.18,24 However, the number of randomized trials examining the effect of the Mediterranean diet on liver histology is limited.24 Long‑term trials on standardized nutritional interventions, evaluating the effect on fibrosis, are necessary.5,24 In NAFLD, carbohydrate intake should include whole grains, unprocessed cereals, and low–glycemic index foods24; fat intake should aim at high monounsaturated fatty acid and omega‑3 polyunsaturated fatty acid consumption; protein intake should favor vegetable protein, seafood, egg, and white meat consumption. The intake of prebiotic fiber and probiotic‑enriched products may be recommended to promote a reduced caloric intake and favorable microbiota, respectively.24 Information on dietary treatment in NAFLD is summarized in figure 3.24
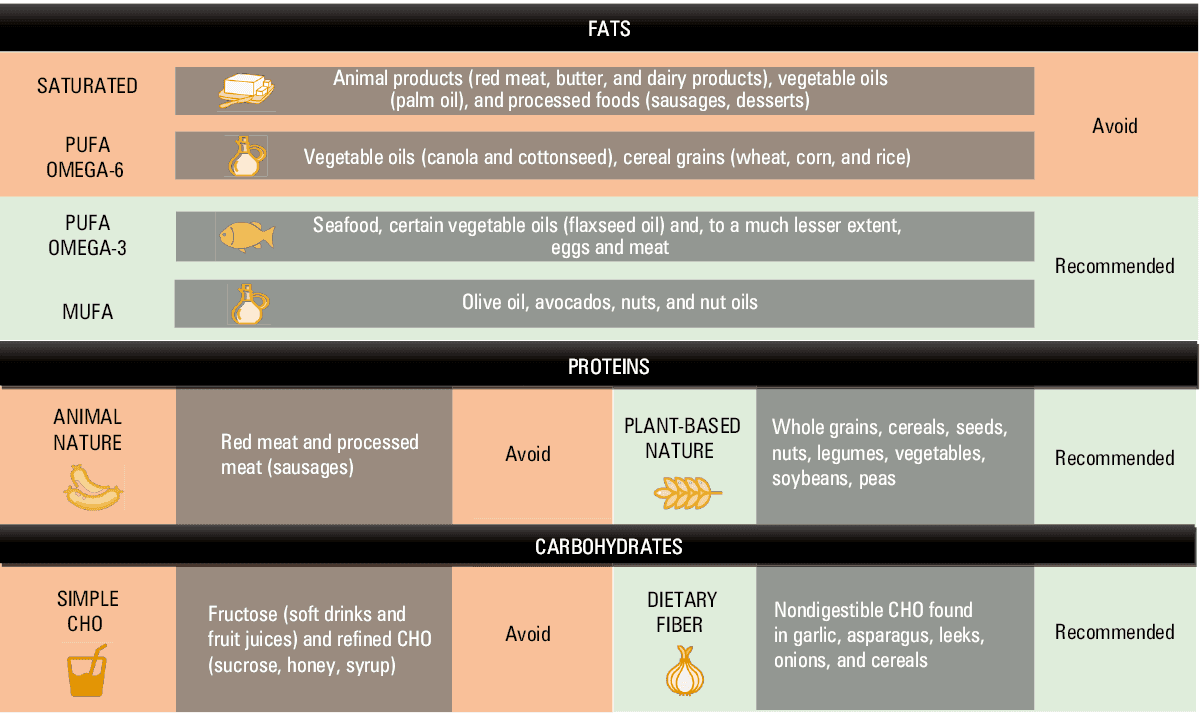
Abbreviations: CHO, carbohydrates; MUFA, monounsaturated fatty acid; PUFA, polyunsaturated fatty acid
Specific management of type 2 diabetes in nonalcoholic fatty liver disease
The coexistence of NAFLD and T2D is dangerous, because it seems to favor quick progression towards more aggressive liver conditions such as nonalcoholic steatohepatitis (NASH), cirrhosis, and hepatocellular carcinoma,5,6 especially in patients with other metabolic comorbidities (arterial hypertension, dyslipidemia, and obesity).5 However, unfortunately, patients and clinicians are unaware of the potentially serious NASH.8 It has been reported that up to 66% of patients with T2D or obesity who are older than 50 years of age have NASH21 and it seems to be an additional independent risk factor for cardiovascular disease.7,8,21 Moreover, patients with T2D and NAFLD have more micro- and / or macrovascular complications in relation to worse glycemic control and atherogenic dyslipidemia. In high‑risk patients, referral to a hepatologist is required in order to rule out other causes of liver disease, perform liver biopsy if necessary, and maintain closer follow‑up.5,6,8
How to assess diabetes in nonalcoholic fatty liver disease
The diagnosis of T2D is established based on the abnormal levels of the following parameters: fasting plasma glucose level ≥126 mg/dl (7 mmol/l), 2‑hour plasma glucose level during a 75‑g oral glucose tolerance test ≥200 mg/dl (11.1 mmol/l), or hemoglobin A1C level (HbA1C) ≥6.5% (48 mmol/mol).27 The HbA1C criteria cannot be used in patients with sickle cell disease, glucose‑6‑phosphate dehydrogenase deficiency, recent blood loss or transfusion, HIV, in pregnancy, and in those undergoing hemodialysis or receiving erythropoietin therapy. Patients with the classic symptoms of hyperglycemia and a random plasma glucose level ≥200 mg/dl (11.1 mmol/l) do not need to meet any further criteria to be diagnosed with T2D.
Referral to an endocrinologist is recommended if the patient is considered to be a candidate for bariatric surgery, has advanced micro- or macrovascular complications, and HbA1C target levels have not been achieved following intensified oral antidiabetic treatment at the primary care level.5,27 The target level of HbA1C is individually established in view of comorbidities, life expectancy, risk of hypoglycemia, and micro- and macrovascular complications.27 In general, a target level of HbA1C <7% is appropriate, but the target level <8% may be appropriate for patients with a history of severe hypoglycemia, limited life expectancy, or significant comorbid conditions.
Pharmacological treatment
Pharmacological treatment should always be considered in T2D and NAFLD, especially if lifestyle recommendations are unsuccessful or challenging to maintain.8 In patients with T2D, glycemic control is essential to prevent NAFLD progression. For now, no drug has been approved by international agencies for the treatment of NAFLD, although there are antidiabetic drugs with proven histological efficacy (table 1). In a systematic review of 11 international guidelines for the treatment of NAFLD, the initiation of pharmacotherapy was recommended when the patient presented with NASH or risk factors for a rapid progression of NAFLD, such as the coexistence with T2D.22 The effect of various antidiabetics on NAFLD was compared in a recent systematic review.28 Pioglitazone and glucagon‑like peptide‑1 (GLP‑1) analogues are antidiabetic drugs having the best effect on liver histology,5,28 and sodium‑glucose cotransporter 2 (SGLT‑2) inhibitors have also been proven to be beneficial, although drug efficacy may be mediated, at least in part, by weight loss.6 Among the pharmacological agents for the treatment of T2D, neither insulin, metformin, sulfonylureas, dipeptidyl peptidase–4 (DPP‑4) inhibitors, nor acarbose are believed to significantly improve NASH or liver fibrosis, although reduced steatosis has been reported in small studies.28
Antidiabetic agent | Steatosis | Inflammation | Fibrosis |
- Marchesini G, Bugianesi E, Forlani G, et al. Nonalcoholic fatty liver, steatohepatitis, and the metabolic syndrome. Hepatology. 2003; 37: 917‑923. | Crossref
- Younossi ZM, Koenig AB, Abdelatif D, et al. Global epidemiology of nonalcoholic fatty liver disease – meta‑analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016; 64: 73‑84. | Crossref
- Abenavoli L, Milic N, Renzo L Di, et al. Metabolic aspects of adult patients with nonalcoholic fatty liver disease. WJG. 2016; 22: 7006‑7016. | Crossref
- Ampuero J, Aller R, Gallego‑Durán R, et al. Significant fibrosis predicts new‑onset diabetes mellitus and arterial hypertension in patients with NASH. J Hepatology. 2020; 73: 17‑25. | Crossref
- European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO). EASL‑EASD‑EASO Clinical Practice Guidelines for the management of non‑alcoholic fatty liver disease. J Hepatol. 2016; 64: 1388‑1402. | Crossref
ARTICLE INFORMATION