Mortality in patients after acute myocardial infarction managed by cardiologists and primary care physicians: a systematic review
Key words: cardiologist, coronary artery disease, general practitioner, mortality, myocardial infarction



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Mortality in patients after acute myocardial infarction managed by cardiologists and primary care physicians: a systematic review
Introduction: Mortality following acute myocardial infarction (AMI) remains high despite of progress in invasive and noninvasive treatments.
Objectives: This study aimed to compare the outcomes of ambulatory treatment provided by cardiologists versus general practitioners (GPs) in post‑AMI patients.
Patients and methods: We conducted a systematic search in 3 electronic databases for interventional and observational studies that reported all‑cause mortality, mortality from cardiovascular causes, stroke, and myocardial infarction at long‑term follow‑up following AMI. We assessed the risk of bias of the included studies using the Risk of Bias in Nonrandomized Studies of Interventions (ROBINS‑I) tool. For randomized trials, we used the revised Cochrane risk of bias tool (RoB 2.0).
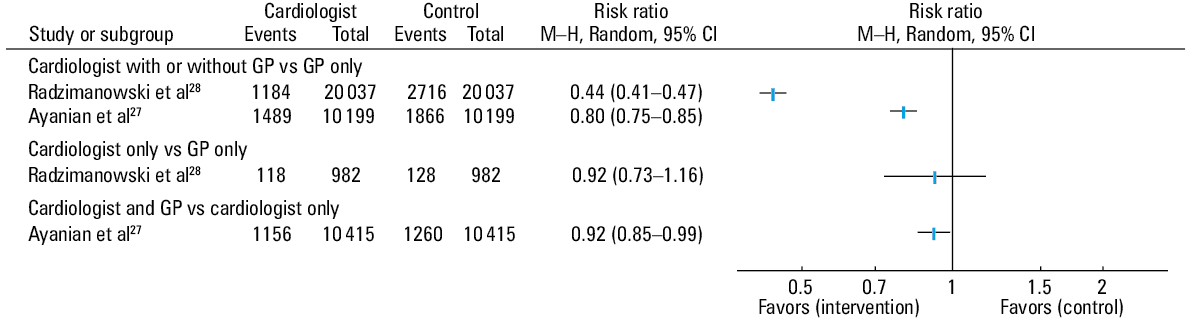
Results: Two nonrandomized studies fulfilled the inclusion criteria. We assessed these studies as having a moderate risk of bias. We did not pool the results owing to significant heterogeneity between the studies. Patients consulted by both a cardiologist and a GP were at lower risk of all‑cause death as compared with patients consulted by a cardiologist only (risk ratio [RR], 0.92; 95% CI, 0.85–0.99). Patients consulted by a cardiologist with or without GP consultation were at lower risk of all‑cause death compared with those consulted by a GP only in both studies (RR, 0.8; 95% CI, 0.75–0.85 and RR, 0.44; 95% CI, 0.41–0.47).
Conclusions: Patients after AMI consulted by both a cardiologist and a GP may be at lower risk of death compared with patients consulted by a GP or a cardiologist only. However, these findings are based on moderate‑quality nonrandomized studies. We found no evidence on the relation between the specialization of the physician and the risk of cardiovascular death, stroke, or myocardial infarction in AMI survivors.
What's new?
Our systematic search showed that patients after acute myocardial infarction consulted by both a cardiologist and a general practitioner may be at lower risk of death compared with patients consulted by a general practitioner or a cardiologist only. Of note, these findings are based on moderate‑quality nonrandomized studies. In this study, we found no evidence on the relation between the specialty of the physician and the risk of cardiovascular death, stroke, or myocardial infarction in acute myocardial infarction survivors.
Introduction
The management of patients with acute myocardial infarction (AMI) has changed significantly over the last few decades, also in the areas of reperfusion therapy and pharmacological treatment. This has led to a significant reduction in both short- and long‑term mortality in most countries.1-9 However, postdischarge mortality rates remain high. In Norway, for example, the 1‑year mortality rate in patients who survive the first 28 days after an AMI event exceeds 10%.5 Researchers have identified several system- and patient‑related factors associated with an increased cardiovascular risk following a patient’s discharge from the hospital These include insufficient risk factor control, insufficient and delayed cardiac rehabilitation, suboptimal pharmacotherapy, delayed complete myocardial revascularization, and comorbidities.4,10 However, the absence of cardiac consultations during the postdischarge period is among the key factors for increased risk. For example, referring a patient with systolic heart failure (often after AMI) after discharge to a cardiologist is associated with a 19% reduction in 1‑year all‑cause mortality (odds ratio [OR], 0.81; 95% CI, 0.68–0.95).11
The evidence regarding mortality rates in patients after AMI suggests that those treated by cardiologists during hospitalization are at lower mortality risk than patients treated by internists or general practitioners (GPs).12,13 In addition, data from the United States have shown that patients hospitalized for AMI and heart failure in areas with a low density of cardiologists were at a slightly higher 30‑day and 1‑year mortality risk.14 As a consequence, we undertook a systematic review of studies comparing morbidity and mortality in post‑AMI patients treated by cardiologists or primary care physicians following patients’ discharge from the hospital.
Methods
We performed an electronic search of the MEDLINE, EMBASE, and the Cochrane Central Register of Controlled Trials database from its inception to July 4, 2019, based on a search strategy specifically developed for this study. We used both subject headings (MeSH and EMTREE) and free text search terms. The following keywords were entered: “cardiologist” with synonyms, “general practitioner” with synonyms and “Myocardial Infarction” with synonyms (for the search strategy, see Supplementary material, Appendix S1). We did not apply any restrictions in terms of publication date or language. Our full search strategy was published online together with the study protocol in the PROSPERO database.15 We manually searched for references of the included studies, relevant review articles, and meta‑analyses for any potentially overlooked studies.
We included experimental, quasi‑experimental, and observational studies, all of which were published as full‑text articles that evaluated all‑cause mortality and cardiovascular outcomes in post‑AMI adult subjects (over 18 years of age) following their discharge from the hospital. To be included in the review, these studies had to analyze patients treated by specialists in cardiology (or physicians undergoing training in cardiology) or by physicians working in primary care (family physicians or general internists), separately. Studies that did not exclude patients with stable coronary artery disease (CAD) were included if they provided information about the subgroups of post‑AMI patients and patients with stable CAD, separately. If the outcomes of a study group were reported in more than one publication, we selected and included in our present analysis the publication that reported the longest follow‑up. If a study was reported in 2 separate articles, we selected and included in the present review the article that analyzed the largest population. Our analysis encompassed a long timeframe (at least 30 days after AMI).
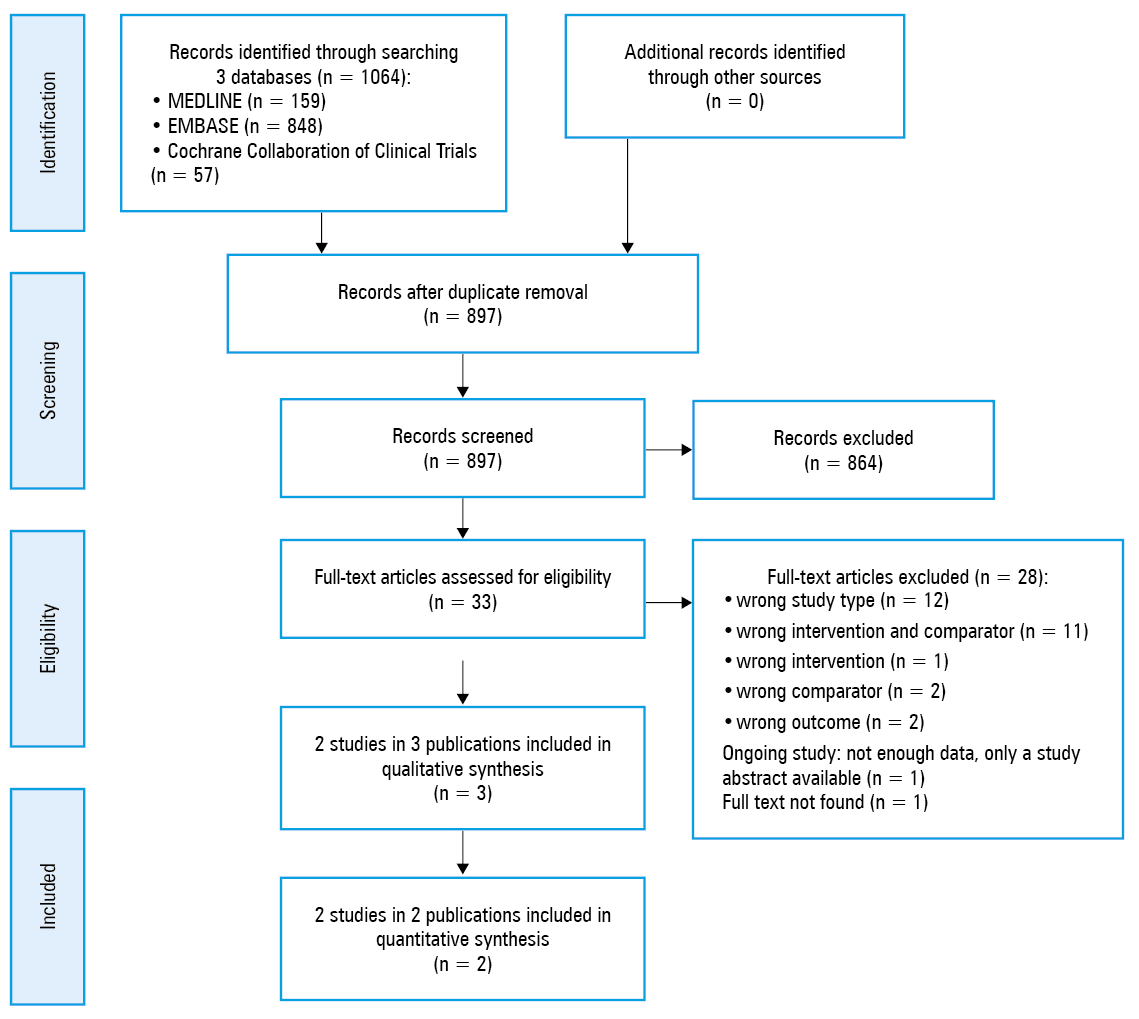
After performing 2 calibration exercises, we screened titles and abstracts in 2 pairs (JP + KJ and DS + WS) using the Rayyan QCRI application.16 We followed a similar procedure for full‑text screening: after 2 calibration exercises, the first author of this study (JP) looked through all the texts in pairs with other researchers (DS, KJ, and WS). All the reviewers (JP, DS, KJ, and WS) independently collected data from primary studies, whereas 2 researchers (JP and DS) evaluated bias using the Risk of Bias in Nonrandomized Studies of Interventions (ROBINS‑I) tool. The collected data comprised, among others, the names of the authors, the year and country of publication, the study purpose, elements of the PICO strategy, conflicts of interest, and funding. We resolved any discrepancies by consensus among the authors at every stage. In the case of missing data, we contacted the authors of the analyzed study by email. We illustrated the study flow at the subsequent stages of the review by means of the Preferred Reporting Items for Systematic Reviews and Meta‑Analyses (PRISMA) diagram.17,18
Regarding follow‑up, we looked at all‑cause mortality, mortality from cardiovascular causes, stroke, and AMI. For the purposes of the present analysis, AMI was defined according to the definition adopted by the authors of each particular study. Similarly, the definition of stroke depended on the concepts used in the analyzed studies. A GP meant a physician working in primary care and included family physicians and internists. We defined a cardiologist as a specialist in cardiology or a physician undergoing specialist training in cardiology.
We assessed the risk of bias in the studies based on validated tools (the revised Cochrane risk of bias tool [RoB 2.0] for randomized controlled trials and the ROBINS‑I tool for nonrandomized controlled trials).19,20 This information was incorporated and discussed within the framework of qualitative data synthesis and is presented in Table 1.
Author, year, study design | Bias due to confounding | Bias in the selection of participants into the study | Bias in the classification of interventions | Bias due to departures from the intended interventions | Bias due to missing data | Bias in the measurement of outcomes | Bias in the selection of the reported results | Overall bias |
a Confounding expected, important confounding domains measured and controlled (propensity score matching of patients used)
b It was clearly defined how patients were classified to one of the intervention groups ( ie, ≥1 visit to a cardiologist, a GP, or an internist in a specified period of time), and the classification was based on medical records. The extent of the intervention was not clearly specified (eg, there were no details provided such as the duration of visits performed and what elements they contained connected with the assessed outcome). No information was provided on the impact of the knowledge of the outcome risk on the intervention status classification.
c No information about the number of excluded patients owing to missing data in matched groups; data for unmatched patients only
d No clear evidence (preregistered protocol or statistical analysis plan) that all reported results correspond to all intended outcomes, analyses, and subcohorts
Abbreviations: GP, general practitioner; RC, retrospective cohort | ||||||||
Ayanian et al,27 2002; Landrum et al,26 2001, RC | Moderate riska | Low risk | Moderate riskb | Low risk | No informationc | Low risk | No informationd | Moderate risk |
Radzimanowski et al,28 2018, RC | Moderate riska | Low risk | Moderate riskb | Low risk | No informationc | Low risk | No informationd | Moderate risk |
Statistical analysis
In the case of nonrandomized studies, data concerning the matched groups of patients were analyzed with the aim to reduce the impact of any differences in group characteristics on the effect of the studied intervention. According to the protocol, random‑effects summary risk ratios on the basis of the DerSimonian and Laird model using 95% CIs as the measure of effect were used when expected heterogeneity between the studies was significantly high. Statistical heterogeneity was measured using the I2 statistics.21-23 A P value less than 0.05 was considered significant. All the analyses were performed using the Review Manager 5.3 software.24 We performed meta‑analyses for each pair of treatment (cardiologist vs GP care) for each outcome (cardiovascular outcomes and all‑cause mortality). The goal was to investigate any substantial heterogeneity between studies.
Results
A total of 4 articles25-28 met the inclusion criteria. A study by Gerlach et al25 was presented only as an abstract and had to be excluded from further analysis owing to lack of sufficient details. Two articles covered the same population within the framework of the Cooperative Cardiovascular Project, and a single paper26 was a substudy of another study,27 which was confirmed by the authors. As a consequence, we excluded a single substudy and included 2 studies in the final analysis: by Ayanian et al27 and Radzimanowski et al28 (Figure 1). We decided not to pool the data because of considerable heterogeneity between the studies (I2 = 99%), which was probably due to the significant gap between the periods of data collection (16 to 17 years), various methods used to treat patients after AMI during these time periods, and different healthcare systems. We did not find any study analyzing the risk of cardiovascular death, stroke, or myocardial infarction in patients who had a cardiac consultation during the postdischarge period compared with patients who did not have such consultation.
Both studies in our review were observational and included a retrospective cohort. The follow‑up period was 1.5 years in the study conducted by Ayanian et al27 and 2 years in the study by Radzimanowski et al.28 The total number of patients treated by a cardiologist in the matched groups from both studies was 30 236. The mean age of patients was 69.8 years. The total number of patients from both groups that received no care from a cardiologist was also 30 236. Those patients were at a mean age of 69.8 years. The study populations constituting both groups were primarily of male sex. In the study by Ayanian et al,27 propensity‑score matching based on sociodemographic and clinical variables was performed using the logistic regression model as a function of 36 variables that predicted whether a patient would visit a cardiologist. In the study by Radzimanowski et al,28 the matching method was similar, and the overall number of sociodemographic and clinical variables was 26. According to Ayanian et al,27 the most commonly reported conditions before admission were hypertension, angina, and diabetes. In the second study,28 the most frequent complications included a history of chronic ischemic heart disease, hypertension, and dyslipidemia.
Research elements included in the analysis according to the PICO list and the baseline characteristics of the matched groups of patients are shown in Table 2. The studies were assessed as having a moderate risk of bias (Table 1).
Author, year, country, data source | Design, duration, overall sample size | Selected characteristics of the study patients | Inclusion criteria | Exclusion criteria | Intervention in the primary analysis | Comparator in the primary analysis | Primary outcome measured | Funding / CoI |
Abbreviations: AMI, acute myocardial infarction; CCP, Cooperative Cardiovascular Project; CIHD, chronic ischemic heart disease; CoI, conflict of interest; FP, family practitioner; IM, impaired mobility; NA of SHI, National Association of Statutory Health Insurance; NR, not reported; PSMs, propensity score matching methods; others, see Table 1 | ||||||||
Ayanian et al,27 2002, United States, CCP
(Landrum et al,26 2001, United States, CCP—a substudy including a smaller population) | RC, 1994–1995, 35 520 patients | The total study group treated by cardiologists included 24 656 patients.
The total group treated by GPs only included 10 864 patients.
Groups of patients matched by PSMs (comparison 1):
Groups of patients matched by PSMs (comparison 2):
| Patients who were discharged in the United States with a principal diagnosis of AMI, at least 65 yrs with fee‑for‑service Medicare coverage. |
| Patients who had at least 1 office visit with a cardiologist during the 3 months after discharge (with or without a visit to an internist or an FP). | Patients who had at least 1 visit with a GP (an internist or an FP) but no visit with a cardiologist during the 3 months after discharge. | 2‑year all‑cause mortality after discharge | Yes / NR |
Radzimanowski et al,28 2018, Germany, NA of SHI | RC, 2011, 158 494 patients | The total group treated by cardiologists included 81 030 patients.
The total group treated by GPs only included 77 464 patients.
Groups of patients matched by PSMs (comparison 1):
Groups of patients matched by PSMs (comparison 2):
| Patients who were newly diagnosed with AMI, coded as “confirmed” or “status post” by an ambulatory physician. |
| Patients who were consulted by an ambulatory cardiologist at least once within the first year after discharge | Patients without ambulatory cardiology care within the first year after discharge | 18‑month all‑cause mortality | No / no |
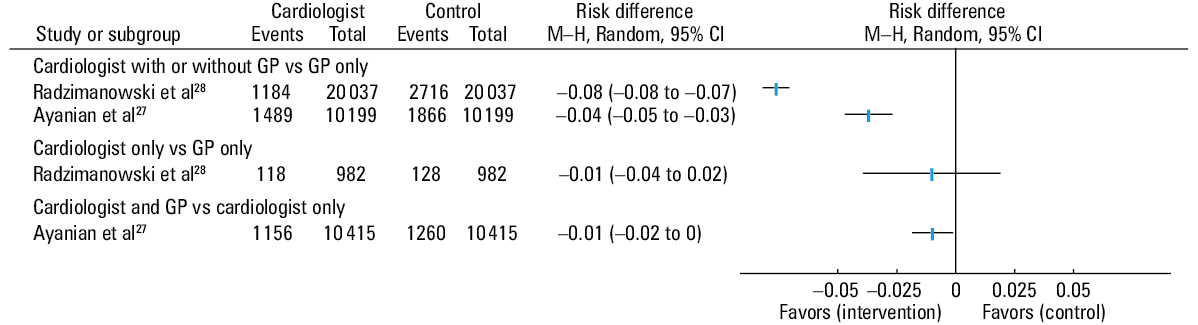
The available data allowed for 3 comparisons: 1) patients treated by cardiologists with or without GP consultation versus those treated by GPs only; 2) patients treated only by cardiologists versus those treated only by GPs; and 3) patients treated by both a cardiologist and a GP versus those treated by cardiologists only (Figures 2 and 3). The first comparison included data from both studies and showed a significantly lower risk of death in patients treated by cardiologists with or without care provided by GPs compared with those treated only by GPs. The second comparison could be based on a single study and showed no significant difference between the groups. The third comparison was also based on the results of a single study and showed a significantly lower risk of death when patients were treated by both a cardiologist and a GP as opposed to those treated only by a cardiologist.
Abbreviations: M–H, Mantel–Haenszel method; others, see Table 1
Discussion
The results of this systematic review showed that patients after AMI who received ambulatory care from both a cardiologist and a GP may have better long‑term outcomes than those treated only by a GP. To the best of our knowledge, our systematic review is the first attempt to summarize the evidence on this topic. There are several reasons that could contribute to a better prognosis in post‑AMI patients treated in outpatient clinics by cardiologists in cooperation with GPs compared with GPs only. Perhaps, the former group has easier access to cardioprotective drugs in effective doses, cardiac rehabilitation, diagnostic workup, and some procedures, eg, repeat revascularizations.
The previously published systematic review described the relationship between a physician’s specialty and the mortality of patients after AMI.12 However, the authors of this survey considered only the specialization of physicians who treated patients in the hospital. It covered 11 studies. The unadjusted mortality rates were lower in patients treated in the acute phase by cardiologists compared with those treated by physicians with other specializations (eg, family physicians). After adjusting for baseline imbalances, the differences were often very small. The multivariable odds ratios for in‑hospital and 30‑day mortality rates in patients treated by cardiologists versus those treated by GPs ranged from 0.95 to 1.29,29,30 while 1‑year mortality rates ranged from 0.99 to 1.3.31,32 As for the lower mortality of patients after AMI treated by cardiologists, this could be due to the fact that cardiologists are more specialized than GPs in managing patients after myocardial infarction, which could lead to more frequent and adequate prescription of medications improving survival, as well as more frequent referral to cardiac rehabilitation and invasive cardiology centers.33 Considering that access to typical AMI treatment (both percutaneous coronary intervention and medical therapy) is nowadays granted, the effect of physician specialty may be lower.
Hartz et al12 underlined the fact that no studies adequately accounted for reasons why a cardiologist did not treat patients who had sustained myocardial infarction. These reasons might include, for example, patient preferences, aggravation of comorbidities, general health status, or resource availability.12 Moreover, results comparing patient outcomes by treating physician’s specialty are often influenced by relevant patient or resource characteristics, which were not taken into account.12
The European Society of Cardiology currently emphasizes that low‑risk patients after AMI can be safely discharged from the hospital 2 or 3 days after an effective primary percutaneous coronary intervention.34-36 A short hospital stay means less time to ensure that the patient is provided with the right information and receives optimal pharmacological treatment. It is therefore becoming increasingly important that a patient consults a cardiologist shortly after hospital discharge and participates in a formal rehabilitation program. Recently, some countries have introduced managed care programs aimed at improving access to cardiologist care following hospitalization for AMI.37,38 For example, in Poland, the National Health Fund (Narodowy Fundusz Zdrowia) requires patients to have at least 3 consultations with a cardiologist within the first 12 months following AMI, with the first consultation within the first 6 weeks.37,39 Managed care programs following myocardial infarction are highly graded by patients.40
In our view, further research should focus on describing the impact of the medical specialty on the mortality of patients after AMI, especially from the perspective of providing more effectively defined interventions (number and duration of visits in a given period of time).
Limitations
The present systematic review had several limitations. First, the studies were observational and nonrandomized. No single double‑blinded study fulfilled the inclusion criteria. Second, only 2 studies were included in the review. Despite extensive database search, we found only these studies and this may result in publication bias. It is important to note that one of these studies contained the data of patients hospitalized from 1994 to 1995, whereas the other study included a considerable amount of recent data. Therefore, their results may not reflect the current practice.27,28 Over the years, the treatment of patients with AMI both during hospitalization and in the postdischarge period has significantly changed. Invasive treatment in the acute phase of AMI has spread, thrombolysis has become less common, numerous new drugs have been introduced in routine clinical practice, eg, clopidogrel, ticagrelor, statins, and renin–angiotensin–aldosterone system inhibitors. This could have caused significant heterogeneity between the studies we have found. Finally, the fact that the first study was performed in the United States and the other in Germany is also a limitation, as these countries have diverse health and healthcare professional education systems, which results in discrepancies in competencies and referral for procedures.41,42
Conclusions
This systematic review suggested that patients after AMI who were consulted by both a cardiologist and a GP may be at lower risk of death compared with those consulted by a GP or a cardiologist alone, although we found no high‑quality, up‑to‑date analyses in this field. We found no evidence regarding the relationship between the specialization of a physician and the risk of patients’ cardiovascular death, stroke, or myocardial infarction in AMI survivors. There is an urgent need for new, properly reported research in this area. These studies should focus not only on all‑cause mortality, but also on recurrent AMI, stroke, and cardiovascular mortality.
- Jernberg T, Johanson P, Held C, et al. Association between adoption of evidence‑based treatment and survival for patients with ST‑elevation myocardial infarction. JAMA. 2011; 305: 1677‑1684. | Crossref
- Puymirat E, Aissaoui N, Cayla G, et al. Changes in one‑year mortality in elderly patients admitted with acute myocardial infarction in relation with early management. Am J Med. 2017; 130: 555‑563. | Crossref
- Gasior M, Gierlotka M, Pyka Ł, et al. Temporal trends in secondary prevention in myocardial infarction patients discharged with left ventricular systolic dysfunction in Poland. Eur J Prev Cardiol. 2018; 25: 960‑969. | Crossref
- Jankowski P, Czarnecka D, Badacz L, et al. Practice setting and secondary prevention of coronary artery disease. Arch Med Sci. 2018; 14: 979‑987. | Crossref
- Sulo G, Igland J, Sulo E, et al. Mortality following first‑time hospitalization with acute myocardial infarction in Norway, 2001–2014: time trends, underlying causes and place of death. Int J Cardiol. 2019; 294: 6‑12. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION