Disseminated disease with Strongyloides stercoralis infestation in follicular lymphoma



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Disseminated disease with Strongyloides stercoralis infestation in follicular lymphoma
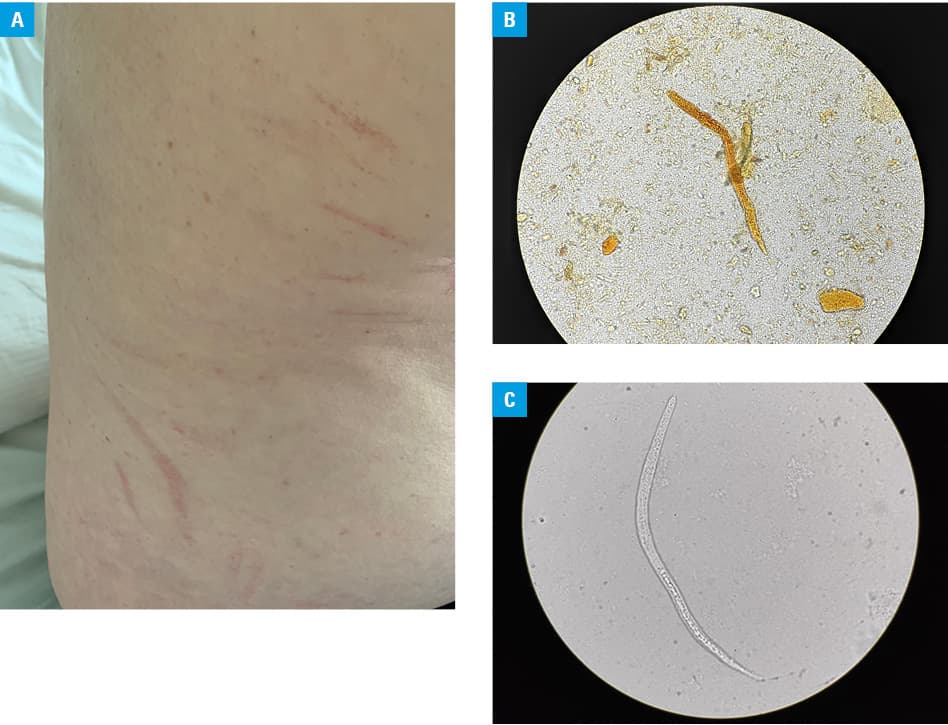
A 75‑year‑old man diagnosed with follicular lymphoma 3 years earlier was admitted to the Department of Rheumatology and Immunology due to expiratory wheezing and worsening dyspnea during the last 3 months. Also, the patient had a 2‑year history of paroxysmal cough and pruritus. He also complained of periodic abdominal pain and borborygmi occurring during the last 3 years. Empiric clarithromycin therapy for suspected bronchitis, administered prior to admission, did not improve respiratory symptoms. Physical examination revealed diffuse expiratory wheezing and multiple erythematous linear streaks on the patient’s trunk and extremities (Figure 1A). The physical examination was otherwise unremarkable. Initial workup revealed eosinophilia (1172 cells/ul; reference range, 40–450 cells/ul) and normal levels of vitamin B12, tryptase as well as immunoglobulins G and E. The patient tested negative for FIP1L1‑PDGFRA, JAK2, and ETV6‑PDGFRB mutations. His medical records showed that eosinophilia gradually increased since immunochemotherapy for follicular lymphoma had been started 3 years earlier (8 cycles of R‑CVP therapy, ie, rituximab, cyclophosphamide, vincristine, and prednisolone, followed by 10 cycles of rituximab every 2 months, with the latest cycle administered a month prior to the described presentation). Chest X‑ray and computed tomography did not demonstrate interstitial infiltrates. Abdominal ultrasonography and echocardiography revealed no significant abnormalities. The patient was unable to undergo spirometry due to dyspnea and cough. Following the initial suspicion of eosinophilic bronchitis, intravenous methylprednisolone (80 mg daily for 6 days, subsequently tapered) combined with inhaled budesonide (2000 μg twice daily) and inhaled bronchodilators were started. The patient continued to deteriorate with dyspnea and wheezing. Stool examination was performed to further evaluate eosinophilia, which remained stable. Microscopic studies of the stool samples revealed the larvae of Strongyloides stercoralis (S. stercoralis) (Figure 1B). Moreover, expectorated sputum samples contained the rhabditiform larvae of S. stercoralis (Figure 1C). The test for human T‑cell lymphotropic virus type 1 and 2 quantitative antibodies yielded negative results. The results of serological evaluation for other parasitic infections (toxocarosis and echinococcosis) were negative. The patient’s history was re‑evaluated and revealed past employment at water well construction.
Steroids were discontinued and albendazole (400 mg twice daily) was administered until stool examination was negative for S. stercoralis for 2 consecutive weeks. The treatment was continued for 28 days and resulted in the improvement of respiratory signs and symptoms and reduction of eosinophil count.
Strongyloidiasis is an infestation caused by S. stercoralis.1 While prevalent in the tropical and subtropical regions of the world,2 data on S. stercoralis occurrence in Poland are scarce.3 Transmission occurs through skin inoculation with larvae residing in soil or via the fecal–oral route through ingestion of the parasite’s eggs.3,4 The affected patients present with nausea, diarrhea, weight loss, abdominal pain, as well as pulmonary and skin symptoms manifesting high‑burden disease.2,4 In some cases (eg, corticosteroid treatment, human T‑cell lymphotropic virus type 1 infection, hypogammaglobulinemia, and hematologic malignancies), patients may develop hyperinfection syndrome or disseminated disease eventually leading to shock and alveolar hemorrhage.2,4,5 Treatment options include either albendazole or ivermectin use, both drugs with proven efficacy.1-3 Eosinophilia, especially in the context of immunosuppression and gastrointestinal, dermatological, or respiratory symptoms should prompt evaluation for Strongyloides infestation and empiric antiparasitic therapy prior to administration of glucocorticoids to prevent fatal dissemination of the disease.
- Alsharif A, Sodhi A, Murillo LC, et al. Wait!!! No steroids for this asthma… Am J Case Rep. 2015; 16: 398‑400. | Crossref
- Khan WA, Santhanakrishnan K. Hypereosinophilic syndrome secondary to strongyloides infection: a case of recurrent asthma exacerbations. BMJ Case Rep. 2013; 2013: bcr2013009587. | Crossref
- Wesołowska M, Rymer W, Kicia M, Popiołek M. Concurrent infection of a young tourist by hookworm and Strongyloides stercoralis during low budget travel in Southeast Asia. Helminthologia. 2018; 55: 166‑172. | Crossref
- Lowe RC, Chu JN, Pierce TT, et al. Case 3‑2020: a 44‑year‑old man with weight loss, diarrhea, and abdominal pain. N Engl J Med. 2020; 382: 365‑374. | Crossref
- Mejia R, Nutman TB. Screening, prevention, and treatment for hyperinfection syndrome and disseminated infections caused by Strongyloides stercoralis. Curr Opin Infect Dis. 2012; 25: 458‑463. | Crossref
ARTICLE INFORMATION